This report originates from a report by the working committee for mental health, which consists of the following people: Dr. In the fourth chapter, the members of the Conseil de discuss the organizational modalities of medical care using a population-based approach, given the high prevalence of mental disorders and disability and associated costs.
The heavy burden of mental disorders
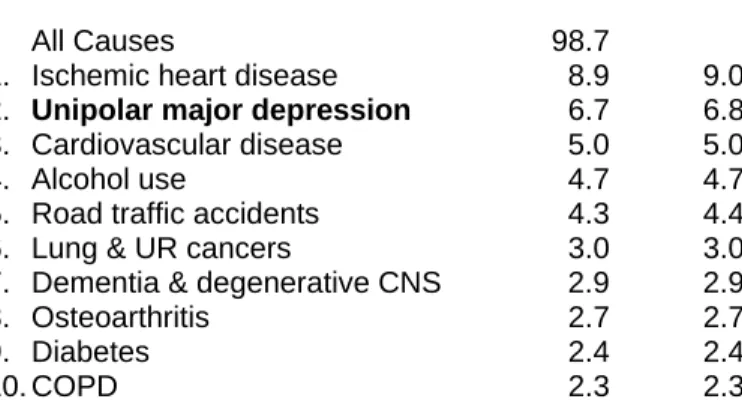
According to Murray and Lopez, authors of the Global Burden of Disease study, the burden of mental health disorders, including suicide (see table below), is second only to cardiovascular disease, just ahead of cancer. All cardiovascular diseases 18.6 All mental diseases, including suicide 15.4 All malignant diseases (cancer) 15.0 All respiratory diseases 4.8 All alcohol use 4.7 All infectious and parasitic diseases 2.8 All drug use 1.5.
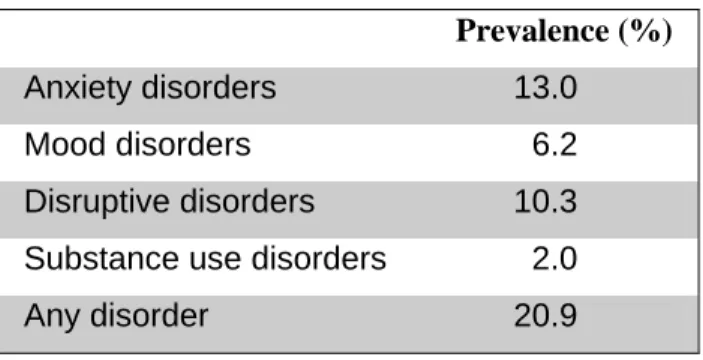
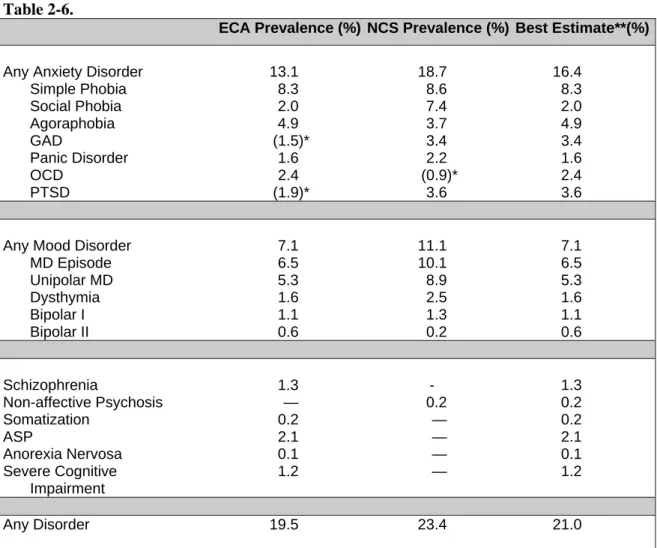
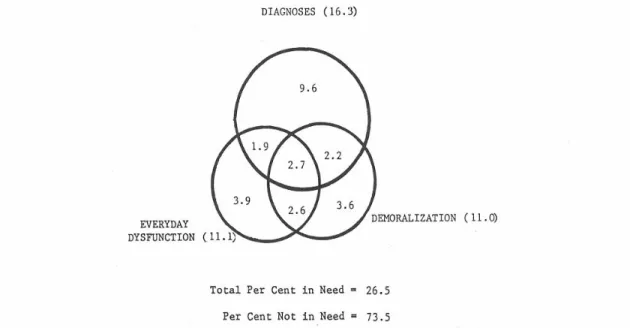
High prevalence rates
The unduplicated GAD and PTSD rates were added to the overall best estimate for any anxiety disorder (3.3%) and any disorder (1.5%). Among other countries, Australia8 reports similar prevalence rates for mental disorders evaluated in large epidemiological studies and rates of schizophrenia and non-affective psychosis similar to those reported in US studies.
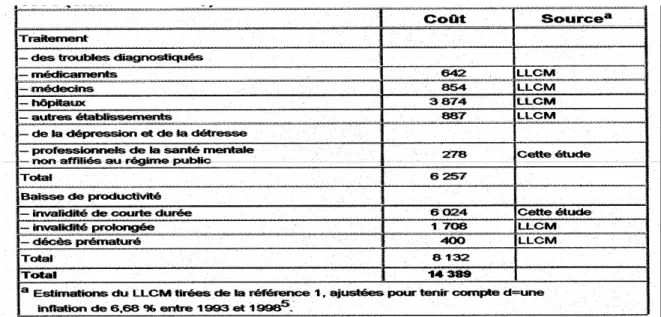
Costs among the highest: invalidity, premature death, comorbidity with
Mental disorders, including anxiety and depression, are often a comorbidity of acute or chronic physical illnesses. On the other hand, if mood disorders, anxiety and depression turn out to be the most expensive mental disorders, the effect of short-term treatments is good.
Essential definitions
So defined, mental health is much more than the absence of mental illness. A mental health problem can refer to signs and symptoms of a mental disorder, regardless of whether the criteria for clinical diagnosis are met or not.
Popular beliefs: diseases or states of mind
Hayward and Bright concluded, from a review of previous literature, that people with mental illness were perceived as dangerous and unpredictable, difficult to talk to, with only themselves to blame, with a poor outcome and that responded poorly to treatment. The most negative opinions are related to people with schizophrenia, alcoholism and drug addiction, with more than 70% of respondents considering these people as dangerous to others and unpredictable. Moreover, it is estimated that alcoholics, drug addicts and people with eating disorders are to blame for their problems.
Regarding people with depression, 62% of respondents indicated that they are difficult to talk to, and to a lesser extent, that they are dangerous to others and that they will not eventually recover. The diagnosis itself is stigmatizing: almost half of people with a formal diagnosis say they are embarrassed by their symptoms, compared to 17% of those who have not been diagnosed. Twice as many people with a formal diagnosis are afraid to talk to their friends about their mental health problems, and only 40% of them believe their symptoms mean they have a mental disorder.
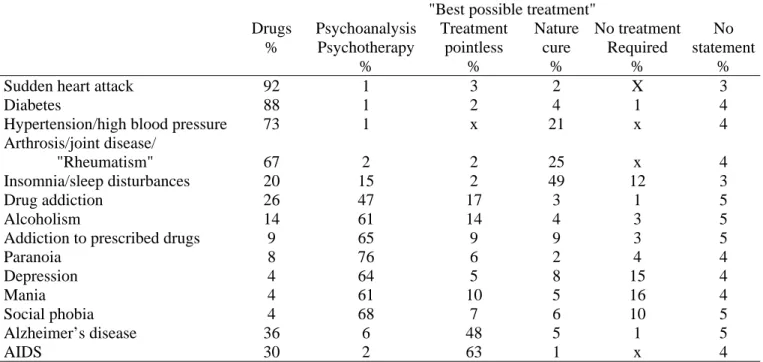
Popular beliefs: treatments
We believe it is important to understand this, as developments in modern psychopharmacology are leading to major advances in the treatment of mental disorders and to reductions in associated disability. And media16 play a crucial role in presenting these topics, as they appear to be the most important source of information for a large part of the population. The influence of the media on the acceptance or rejection of psychotropic drugs is even stronger than the influence of the individual's own values.
Then there is the perception of the prognosis: the poorer the prognosis, the less the inclination to choose a confidant. The Conseil is all the more convinced of the importance of fighting these prejudices as a growing number of people are exposed to their consequences. This forces them to hide their psychiatric history and divulge information when they request a job, adding to the pain and stress of the illness of being discovered, a constant fear.
Solutions
The committee carried out the project in several steps, from the analysis of the needs of different groups to the analysis of the results and follow-up to preserve the acquired knowledge. Bridging the gap between health professionals' and the public's differing beliefs about beneficial treatments and interventions. Other programs have chosen to take action at the media level by publicly criticizing them when they portray mental illness negatively, or better yet, by supporting quality journalistic reporting and awarding awards for excellence in journalism (Rosalynn Carter Fellowships for Mental Health Journalism). .
Other programs prefer to introduce bills, such as the 'Mental Health Early Intervention, Treatment and Violence Prevention Act of 2000' in the United States, which includes, among other things, an anti-stigma campaign to educate the population about the causes of mental illness, effective treatments, and resources available for patients and their families. Implementing an information campaign to improve the population's knowledge of the most common mental disorders, their prevention and effective treatments; Conveying targeted messages to the public and various professional groups, in particular groups from the media, science, justice and the professional field;
Facilitate the dissemination of evidence-based data to better inform the
A group of investigators from the Australian National University1 developed a mental health first aid course integrated into physical first aid training. To ensure that any basic first aid training includes a mental health first aid course. The government of British Columbia3 took a multimodal approach in a pilot project to educate the general population promoting self-care for common physical health problems, but not mental health.
To mandate the Institut national de santé publique du Québec (INSPQ), in collaboration with the Agence d'évaluation des technologies et des modes d'intervention en santé (AETMIS) and the Conseil consultatif de pharmacologie, to implement a website with quality information on mental health, which the public could consult with confidence. To ensure that they get the necessary cooperation from the mental health research field, the academic field and professional associations. There are very few evaluations of the therapeutic possibilities for mental health offered by the Internet: one study mentions some benefits of self-monitoring7, another of computer-administered treatment programs8.
Facilitate harmonization of research-based knowledge with effective and
- Development and quality criteria
- Dissemination and implementation criteria
- Monitoring results
Clinical practice guidelines that answer questions about a specific clinical situation and that are based on the best available information assessed for clinical validity, relevance, and applicability12 are considered high-quality guidelines. To support the leadership of the College of Physicians, in cooperation with the professional associations involved and with the support of research and evaluation resources, in the development, implementation and updating of medical practice guidelines for the detection, diagnosis and treatment of mental disorders;. How practice guidelines are disseminated is critical to their adoption and implementation by professionals.
At the regional level, support a formal organizational structure for the implementation of mental health practice guidelines;. Ensure that the necessary technical and human resources to implement these practice guidelines are adequately funded. Since the ultimate goal of clinical practice guidelines is to help improve care by optimizing practices, they obviously need to adhere to the reality of different clinical needs.
Facilitate the integration of research-based knowledge in healthcare
In addition to analyzing the relationship between researchers and decision-makers, this study very relevantly shows the influence of "knowledge carriers", presented as a very heterogeneous group, including public relations organizations, the media, foundations, think tanks, representatives of the commercial sector and from various scientific publications. A move towards evidence-based decision-making will involve tempering these anecdotes and stories from various interests with facts and evidence from research16. The Conseil believes that the implementation of the measures proposed in this chapter will help to improve evidence-based decision-making.
Aware that different organizational models have been proposed for mental health care and services, the members of the Conseil consider in this chapter the needs for medical services with a population-based approach, given the high prevalence of mental disorders and the disability and costs associated with them to go. with them. They took into account the opinions of the Ministère de la Santé et des Services sociaux1,2,3,4 and professional organizations such as the Association des médecins psychiatres du Québec5,8, the Collège des médecins du Québec6, the Fédération des médecins omnipraticiens du Québec5 , the College of Family Physicians of Canada7, the Canadian Psychiatric Association7, the Quebec Hospital Association9, as well as previous recommendations of the Conseil médical du Québec regarding the hierarchical organization of services10,11, also used in the report of the Clair Commission (Commission d'étude sur les services de santé et les social services)12. Members analyzed the contribution of primary and secondary health services to reducing the burden of mental disorders, based on principles of accessibility, evidence-based quality practices and continuity of care related to service integration.
Primary care: accessibility, inclusiveness and continuity of general medical
- Role of the primary care
- Barriers to primary care diagnosis and treatment
- Primary care physician needs
In this context, a general practitioner must pay careful attention to detecting mental disorders, in addition to contributing to health promotion and disease prevention. The GP must make an accurate diagnosis in order to choose the necessary treatment and provide the patient with effective and specific treatment23. There are several barriers to the first-line diagnosis and treatment of mental disorders.
A family doctor may not have all the necessary knowledge and skills to detect, diagnose and treat various mental disorders. Since it is now recognized that mental and physical health care must be integrated into the same service structures (the mainstreaming concept), the family doctor needs more time and an appropriate remuneration for these clinical activities. The psychiatrist who will work together with his colleague at the interface between primary and secondary mental health services25 should be aware of all the special aspects of primary psychiatry.
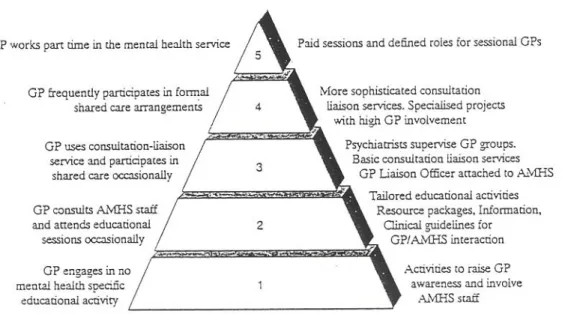
Models of working at the interface between primary and secondary mental
- Models
- Impacts of consultation-liaison and shared care models
- Costs and cost-effectiveness ratio?
- Conditions for success and implementation strategies
In this model, only the psychiatrist sees new patients and does the necessary follow-up in the offices of a primary care clinic. The consultation-liaison model can also be linked to a shared care approach, where some patients receiving secondary care are referred for management to primary care. The Ontario approach does not differentiate between primary care patients and patients transferred from secondary care services, as both types of patients are registered at participating clinics and physicians are paid on a capitation basis.
The secondary care team, including a psychiatric nurse who acts as a case manager and a psychologist who coordinates the project, works together to ensure that the transferred patients agree to the transfer and have the necessary characteristics for primary care follow-up. However, this study did not estimate the cost of treating these patients in primary care. Assess the necessary conditions for the improvement of screening, diagnosis and treatment of mental disorders in the implementation of family medicine groups and group clinics of primary health care;
Secondary care services: specificity, complexity, accessibility through
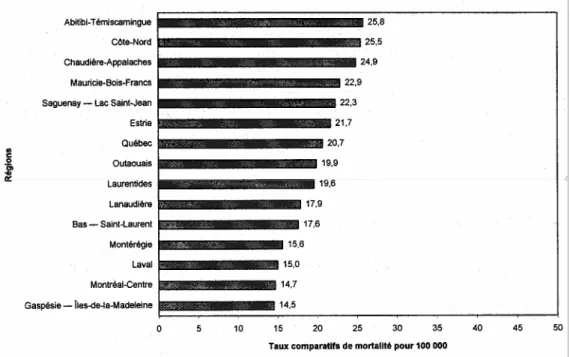
Politique de santé et de bien-être, Québec, ministère de la Santé et des Services sociaux, 1992. S'entraider pour vivre : la Stratégie québécoise d'action contre le suicide, Québec, ministère de la Santé et des Services sociaux, 1998 [p. Rapport de mise en œuvre de la politique en santé mentale, Québec, ministère de la Santé et des Services sociaux, 1997.
Indicateurs de la politique québécoise de la santé et du bien-être : exercice de suivi 1995, Québec, ministère de la Santé et des Services sociaux, 1995. Indicateurs de la politique québécoise de la santé et du bien-être : suivi de l'exercice 1998, Québec, ministère de la Santé et des Services sociaux , 1998. Orientations pour la transformation des services de santé mentale : document de consultation, Québec, ministère de la Santé et des Services sociaux, 1997.
Plan d'action pour transformer les services de santé mentale, Québec, ministère de la Santé et des Services sociaux, 1998. Les défis de la transformation des services de santé mentale : Répondre de manière efficace et efficiente aux besoins des personnes atteintes de troubles mentaux graves, Québec, ministère de la Santé et des Services sociaux, 1997 .