It is with a grateful heart that I acknowledge the generous contributions of many to this dissertation. I would like to acknowledge the enormous contributions of the critical care nurses with whom I have worked in my clinical practice, as well as those who participated in this study. I wrote this thesis for these nurses as my way of saying thank you for showing me what it means to care for people during their darkest days.
I sincerely hope that this research will help nurses thrive in critical care. Funding for this research was received from the Social Sciences and Humanities Research Council of Canada, Athabasca University, and the Canadian Nurses. This study was conducted to learn more about nurses' resilience in response to workplace adversity.
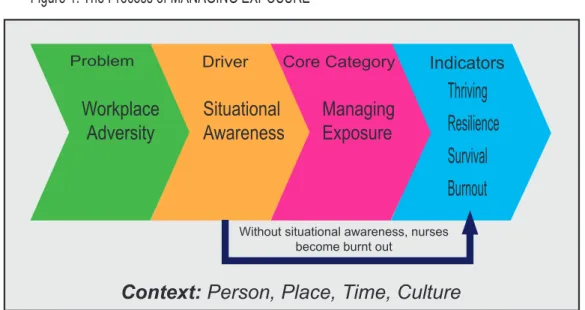
This grounded theory study was conducted in a large, multi-site urban hospital with 11 intensive care nurses. Nurse leaders can intervene in critical care environments to reduce workplace adversity and drive the process of MANAGING EXPOSURE to resilience.
INTRODUCTION
Critical Care Nurses: Nurses in critical care settings are highly skilled, with specialized education (Vanderspank-Wright, Bourbonnais, Toman, & McPherson, 2015). Critical care nurses reported a decrease in the quality of their work environments (Ulrich, Lavandero, Woods, & Early, 2014). Many factors that contribute to workplace adversity in critical care settings are specific to these settings.
Structural factors, such as nursing staffing, can be highly influential in the quality of critical care settings (Ulrich et al., 2014). Critical care nurses may be particularly prone to the negative impacts of workplace disasters such as burnout (Epp, 2012). Nursing burnout has been widely researched and is a well-known problem experienced by nurses in critical care settings.
These factors may make the resilience process for critical care nurses unique to other resilience processes. The proposed grounded theory resulting from this research study provides a framework for understanding the resilience process for nurses in critical care settings in response to workplace disasters.
LITERATURE REVIEW
It is also worth noting that the provision of critical care in the Canadian health care system uses a significant amount of health care resources. Approximately 27% of all deaths at Canadian teaching hospitals occur in critical care settings (Heyland et al., 2000). While specific rates of burnout are not known for Canadian critical care nurses, critical care settings have the highest level of nursing staff turnover rates in Canada (O'Brien-Pallas et al., 2010).
Job stress is cited as the main reason for critical care nursing burnout (Epp, 2012; Khamisa et al., 2013). Resilient nurses identified their spirituality and social support as the two most common supports in the critical care setting (Mealer et al., 2012). Critical care nurses also experience high levels of burnout, and it is likely that resilience would mitigate workplace difficulties in a critical care setting.
It is possible that critical care environments can optimize buffering factors to promote nurse resilience. This study demonstrates that it is possible for nurses to develop effective coping strategies in critical care environments.
METHOD
The roots of grounded theory research include aspects of the empirical paradigm, especially for followers of Glaser's thought (Engward, 2013). The use of the grounded theory method inherently recognizes that the context of a theory is inseparable from the theory itself (Milliken & Schreiber, 2012). This study was a grounded theory investigation of the research question: what is the process of resilience in critical care nursing in the face of workplace adversity.
All participants were women and varied in age and years of experience in intensive care. Posters were used to inform potential participants of the opportunity to participate in the study (Appendix B. Please note: this appendix has been edited to avoid identifying the study setting). The use of theoretical sampling helps create grounded theory by guiding data collection based on the findings of concurrent data collection and analysis (Breckenridge & Jones, 2009).
Data management was supported, and sometimes hindered, by the use of the research software NVivo. I knew I had reached a possible explanation of the phenomenon when: (a) each of my categories and subcategories was directly supported by research data (b) the theory resonated with my own experiences as a nurse (c) the work Corbin and Strauss satisfied (2008) conditions for grounded theories and (d) the theory felt right. I experienced various stages of uncorking, when I had a breakthrough or new insights that advanced my understanding of the grounded theory.
After the 11th interview, I felt I had a comprehensive understanding of EXPOSURE MANAGEMENT theory. At the conclusion of the research study, I reflected that my assumptions about resilience and adversity were challenged. Together, I used a spreadsheet to track the amount of time spent on each aspect of the research process.
The participants were aware that I intend to publish and present the results of the research study at the end. One will be able to identify the basis of the theory from the participants' quotes (Gillis & Jackson, 2002; Richards & Morse, 2013). All of these efforts resulted in a rigorous proposed theory of the process of resilience to critical care nurses facing adversity in the workplace.
FINDINGS Overview
These types of workplace adversity have the potential to spread negativity around a critical care environment. The sources of adversity in the workplace are diverse and range from the critical care environment to the wider community. Adversity at work is a toxic factor in the critical care environment that can have a negative impact.
The duration of exposure also determines how a nurse is affected by workplace adversity in critical care settings. There are a variety of forms of workplace adversity in critical care settings, listed in Figure 2. The politics of health care delivery is a form of workplace adversity for nurses in critical care settings.
The final aspect of workplace adversity at the meso level is the nature of critical care nursing. The final level of workplace adversity is the interpersonal level, referring to interactions between people in the critical care environment. Challenges with patients and families were often cited as workplace adversities in critical care settings.
In the intensive care setting, the impact of workplace distress on a particular nurse is based on its importance to that person. The projection is based on the perceptions and knowledge of the nurse and experiences in the intensive care environment. The same logic may apply to addressing the impact of workplace distress for the critical care nurse.
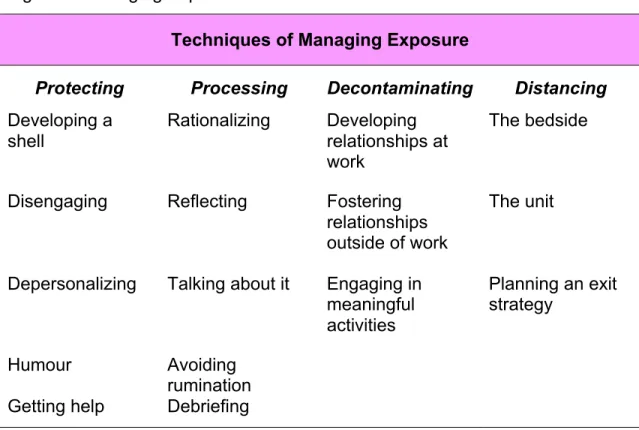
These supportive workplace relationships can assist nurses in decontamination from the intensive care environment. Nurses will move away from the source of workplace problems to manage their exposure in the intensive care setting. In addition to EXPOSURE CONTROL, it is also important to critically assess the presence of workplace problems in intensive care settings.
Survival can represent a victory on days when the workplace in a critical care environment has a high level of difficulty. Success is possible for nurses in critical care settings when they are able to manage exposure to workplace stressors.
DISCUSSION
Canadian health care culture is also influential in the EXPOSURE MANAGEMENT process for critical care nurses. Negative portrayals of nurses in the media contribute to workplace difficulties in critical care settings. In the current study, nurses identified the negative impact of noise in the critical care environment.
Additionally, nurses in the current study reported that they may feel intimidated by the knowledge base required in critical care settings. In the present study, nurses reported feeling intimidated by the knowledge base that is necessary to practice safely in critical care settings. In the current study, nurses identified protective techniques as part of their EXPOSURE MANAGEMENT process.
In the current study, nurses identified vacation as an important part of their exposure management process. The aim of the current study was to map the process of resilience in intensive care nursing. This study proposes substantively grounded theory on the process of managing exposure for critical care nurses to promote nursing resilience.
MANAGING EXPOSURE contributes to the understanding of nursing in critical care settings, in the context of the Canadian healthcare system. In the current study, nurses reported that when they did not have options to leave the intensive care environment, their resilience was. It is possible that continuing education programs that focus on EXPOSURE MANAGEMENT could be useful for nurses in critical care settings.
Administrative nurses can be sensitive to the theory of EXPOSURE MANAGEMENT and provide professional advocacy to create supportive structures in critical care settings. MANAGING EXPOSURE provides a framework for nurse leaders to reduce workplace adversity and promote resilience in critical care settings. The theory of EXPOSURE MANAGEMENT may have implications for populations outside of the critical care setting, and also outside of health care.
CONCLUSIONS
Capability to Care: A Metaethnography of Nurses' Experiences of the Acute Care Nurse-Patient Relationship. Retrieved from: http://www.sna.org.sg/site/singapore-nursing-journal/index.php College of Nursing of Ontario. Serious Beliefs: Stories of the Supernatural and the Terrible Among Canada's Great Soldiers in the Trenches of War.
Longitudinal analysis of psychological resilience and mental health in Canadian military personnel returning from overseas deployment.