In The Leapfrog Group's Barcoded Medication Administration Report (2018), approximately 7,000 deaths annually are attributed to medication errors. Barcode medication administration has been introduced in many areas of healthcare; however, there is limited research on its use in the ED setting or nurses' attitudes toward BCMA. The adoption of technology by ED nurses is a major factor in BCMA's success.
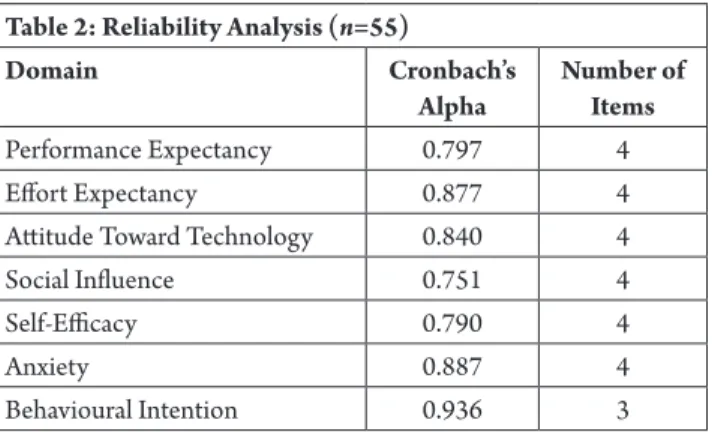
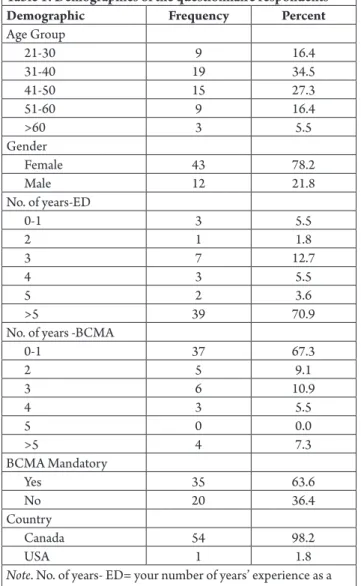
Fifty-five nurses participated in the study; the demographic details of the sample are shown in Table 1. However, the group reported that the attitudes outlined in the PE and ATT domains were not positive towards the adoption of the technology. Recent adoption also means there is leadership support in using the technology.
SI3 Senior management in our emergency department was helpful in using the BCMA. BCMA technology is not commonly used in the ED, so there is minimal literature on ED nurses' attitudes toward BCMA. Challenges in implementing barcoded medication administration in the emergency room versus medical surgical units.
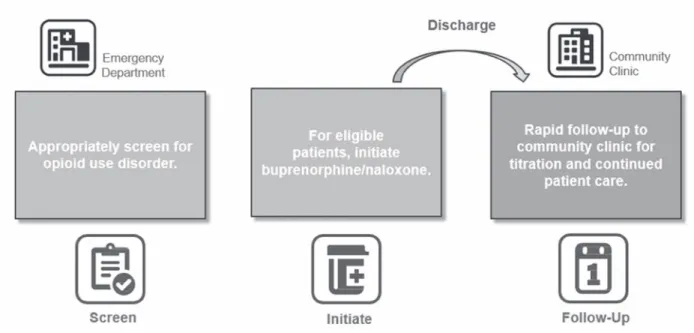
Identify opioid use Disorder
The guideline also identifies buprenorphine/naloxone as the recommended first-line OAT for OUD where feasible. Buprenorphine/naloxone allows for greater patient flexibility and autonomy, resulting in greater treatment compliance, retention, and reduced substance use (CRISM, 2018; Holland et al., 2014). Buprenorphine/naloxone is a 4:1 combination medication that is usually taken once daily when patients are on stable maintenance doses.
Buprenorphine/naloxone has been in Canada since 2007, but was typically only available in addiction medicine outpatient clinics. ESCN recognized a potential opportunity to help patients by having the medication available in the ED. Due to the increasing number of ED opioid-related presentations in Alberta, EDs provide an effective opportunity to intervene and initiate treatment that addresses the underlying condition of OUD that goes beyond the extremely important practice of offering naloxone- set.
In 2018, 13% of individuals in Alberta with an apparent fentanyl-related accidental death had presented to an ED within 30 days before they died, highlighting the ED's opportunity to intervene and the potential to prevent a catastrophic event ( Government of Alberta, 2019). ED patients are more likely to remain engaged in treatment if they initiate buprenorphine/naloxone in the ED. In a pivotal study ED patients randomized to buprenorphine/naloxone treatment remained in treatment 30 days later compared to patients referred to treatment without initiation of buprenorphine/naloxone (D'Onofrio et al., 2015).
The emergency department buprenorphine/naloxone rollout program was the first of its kind in Canada with a provincial scope. ESCN supported training and implementation of a standardized treatment protocol for patients presenting with OUD in all adult emergency clinics in Alberta. Other jurisdictions across the country have programs that offer buprenorphine/naloxone, and each clinical pathway may vary in terms of dosing, assessments, and treatment options.
The ED nurse plays an important role in establishing a safe and open environment where the patient feels respected and understood in a way that has the potential to motivate change. It is important to view every patient interaction as an opportunity to engage, educate and provide support.
Initiate buprenorphine/Naloxone in or out of the emergency Department
After identification of OUD, patients may need encouragement and education from ED health care professionals to consider treatment. Some patients may not be ready to make challenging life changes during their ED visit and may need more time to make that decision.
Provide Rapid Community Clinic Referral for Continued Patient Care
This article is about the effectiveness of nurse practitioners working in the Strathcona emergency department (ED), as well as the effectiveness of two nurse practitioner-led clinics that run parallel to the ED. The Intravenous Therapy (IVT) Clinic is an outpatient clinic that provides IV therapy services 16 hours/day and the Ambulatory Care Clinic (ACC) where there is an Emergency Department Transition Clinic (EDTC) run by NPs working five days in week to ensure follow-up appointments for patients recently seen in the ED. It also allows patients to be treated outside of the emergency department, thus freeing up time/resources/providers in the ED and likely reducing the overall costs associated with the ED visit.
The EDTC provides timely, high-quality care to patients seen in the emergency department who require ongoing and transitional care. Second-year evaluation data also proved that NPs improve access to care and improve patient flow in the ED. Nurse practitioners in the ED are tasked with following up with patients who leave before being seen by a provider or before treatment ends.
The revisit rate was one of the lowest among comparison sites in the Edmonton Zone (Olsen, Yu, & So, 2018). Eighty-nine percent of emergency room patients surveyed were satisfied with the quality of care they received from emergency room physicians (Tessera & Gibbons-Reid, 2016). The three different areas where NPs work at Strathcona Community Hospital prove that NPs can be integrated into a hospital.
Daily assessments of higher acuity patients in the IV clinic result in fewer hospital admissions. Nurse specialists improve patient flow in the emergency department by initiating treatments and diagnostics in the emergency room waiting room. Nurse Practitioner at Strathcona Community Hospital in the Emergency Department, IV Clinic and Emergency Transition Clinic.
Patients seeking care in the ED often experience extended wait times for assessment, diagnosis, and treatment. As the number of patients increases in the ED, other patients face delays that increase their risk for adverse outcomes (White et al., 2012). After approval from the Conjoint Health Research Ethics Board, emergency medicine research assistants recruited eligible participants in the ED.
Of the three, the first two refer to the events in the hospital, which remain the focus of this paper.
Communicating about the waiting process
These include item #10 ("I had confidence in the providers involved in my care"), item #13 ("I was satisfied with the opportunity to talk and ask questions with the providers involved in my care ") and finally, item #15 ("A well-developed and realistic succession plan was prepared and explained to me)". Comparatively, the item means for the relational subfactor show more variation than the informational subfactor. That is, the respective means for five of the eight items lie below the overall mean for the entire sub-factor.
That is, they understood that a doctor had to make an assessment before they could receive pain medication. And even if you're in a lot of pain, they make sure you know it's not life-threatening; its only pain. So you have to wait your turn even if you are in pain.” Participant C005.
Participants felt they could have benefited from better pain management while waiting for an assessment.
Work collaboratively with departments outside the ED, particularly PCUs and surgical suites, to develop processes to eliminate unnecessary transport of patients awaiting surgery while in the ED. Set discharge orders during morning rounds, use parole orders and adjust discharge meeting times to encourage family participation in discharge learning. Give patients and their families information about the waiting process and what to expect so they don't feel left out in the crowd.
Kara has worked in General Surgery/Surgical Oncology, Trauma Surgery and the last 12 years in the Emergency Department. Kara has been involved in various committees while in the ED and completed her Masters in Nursing in the summer of 2018 with a major project investigating the continuity of care for surgical patients admitted from the Emergency Department. The use of performance improvement methods to increase patient satisfaction in the United States emergency department: a critical review of the literature and suggestions for future research.
Association between length of stay in the emergency department and outcome of patients admitted to either a ward, intensive care, or high dependency unit. ED overcrowding: An assessment tool to monitor ED registered nurse workload accounting for admitted patients residing in the emergency department. Improving patient flow and reducing emergency department crowding: A guide for hospitals (Prepared by Health Research . & Educational Trust).
When patients are discharged from the emergency department, the educational information they receive may not be consistent or well enough understood to prevent complications. The purpose of this study was to investigate the effectiveness of an educational intervention for preventing complications in patients diagnosed with atrial fibrillation (AF) and discharged from the emergency department. Clinical data were assessed for both groups during one year of follow-up, with the primary variable being AF or treatment-related complications and the secondary variable being emergency department (ED) visits.
The study looked at patients over the age of 18 who presented to the emergency department in Barcelona, Spain, were diagnosed with atrial fibrillation (AF) and were discharged from the emergency room; patients with cognitive impairment were excluded. The intervention group also received education from a select group of nurses who provided information about the arrhythmia, complications, precautions to consider, how to self-assess the heart rate and when to return to their doctor or the emergency department. . Although this study recognizes that discharge education is typically the role of the emergency physician, rather than the emergency nurse in this department, the importance of patient education following an emergency department visit is recognized by NENA as a core competency (NENA, 2014). ).
This study protocol cannot be exactly replicated in Canadian EDs because the study institution is not in the practice of discharge teaching nurses and because they do not articulate exclusion criteria for cognitive impairment.