Symptoms associated with menopause are known to negatively impact the quality of life for many women. Furthermore, concerns about the risks associated with hormone replacement therapy may prompt women to seek nonpharmacological approaches to symptom management.
Introduction
The yoga practiced mainly in the west derives mainly from the postural yoga popularized by B.K.S. Iyengar, who in turn has his roots in the gymnastic tradition of the Mysore Palace and the teachings of T.
Literature review
Experimental evidence to support the benefits of yoga for menopausal women remains largely unsubstantiated by scientific research. Currently, the majority of available information on the health benefits of yoga is heavily Iyengar-influenced.
Influence of a yoga intervention on quality of life and hormone levels in
Introduction
The decline in estrogen that accompanies menopause (Rannevik et al., 1995) is thought to be a factor in the experience of symptoms, and one that may cause. Higher levels of DHEA-S may protect against vasomotor symptoms (Øverlie et al., 2002) and are inversely associated with psychological distress and musculoskeletal pain (Finset, Øverlie, & . Holte, 2004). Fears of health risks such as breast cancer and heart attack associated with the use of HRT (Twiss, et al., 2007) have spurred interest in alternative, non-pharmacological approaches to symptom management (Kronenberg & Fugh-Berman, 2002; Twiss et al., 2007) .
While claims abound about the benefits and risks of various interventions for menopausal symptoms, there is far less research into the efficacy and safety of CAM therapies compared to that available on HRT (Cheung et al., 2003; Maslow, 2003 ). Behavioral interventions, including paced breathing, meditation and exercise have shown potential to alleviate hot flashes and improve quality of life (Elavsky & . McAuley, 2005; Freedman, 2005; Irvin, 1996; Ivarsson et al., 1998; Lindh-Åstrand et al. al ., 2004).
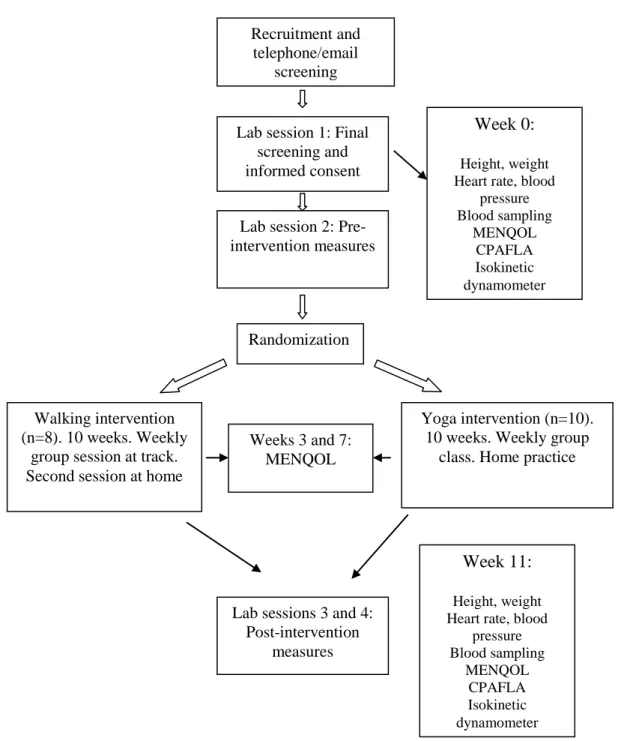
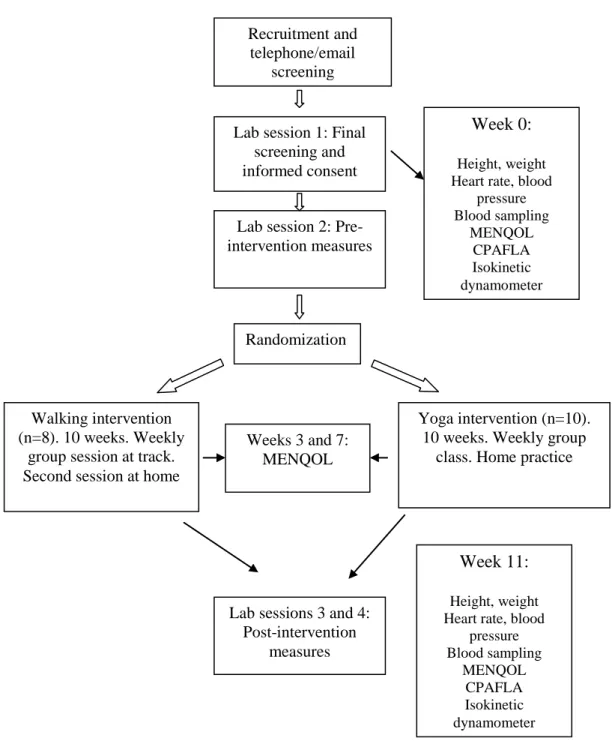
Materials and Methods
During the first session, resting heart rate and blood pressure, height and weight were measured, and resting blood samples were collected. Running intensity and duration were prescribed according to the Canadian Society for Exercise Physiology guidelines (CSEP, 2004). All logs were collected at the end of the activity interventions for use in data interpretation.
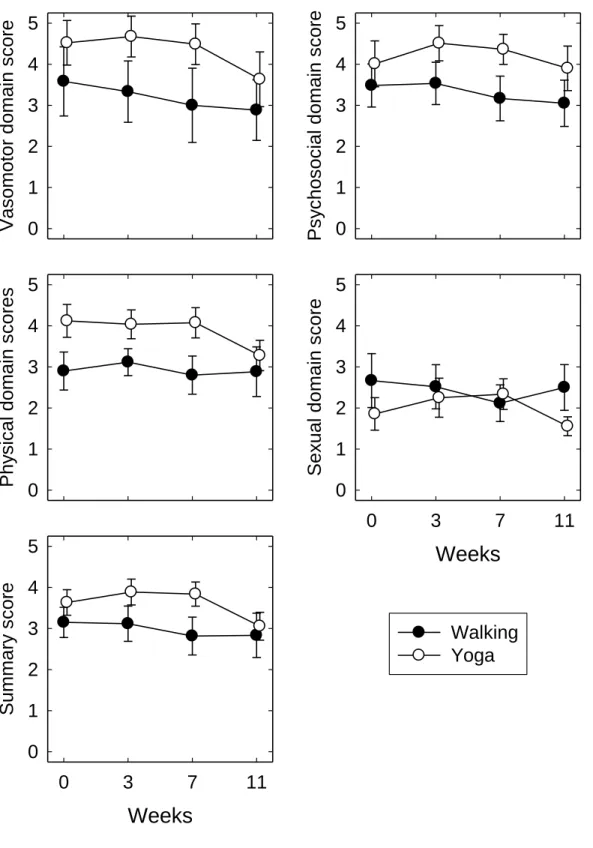
Participants completed the Menopause Specific Quality of Life (MENQOL) questionnaire before and after the intervention (Lewis, Hilditch, & Wong, 2005) and twice more within the 10-week period. Repeated measures ANOVA were also conducted to determine whether the 10-week intervention or activity type affected the concentrations of the hormones DHEA-S and FSH.
Results
Wherever the test for sphericity was significant (p<0.05), the degrees of freedom were adjusted using the Geisser-Greenhouse correction. Repeated measures ANOVA indicated that there were no significant changes for any domain or summary score in either group. Overall, there was a trend toward reduced symptoms with consistent changes over time between the two groups.
Resting serum concentrations of FSH and DHEA-S before and after the activity intervention are shown in Table 3.2. Repeated measures ANOVA was used to examine changes in hormone levels over time and compare groups.
Discussion
The results of this study support previous research showing a trend toward reduced vasomotor symptoms and improved quality of life after 8-10 weeks of yoga. The results of this study are similar to others that have shown beneficial results from yoga practice. The relatively short duration of the intervention, 10 weeks of yoga or walking, may be insufficient to induce changes in the hormonal profiles of menopausal women.
In contrast, the walking participants were fully able to engage in their activity from the beginning of the intervention and progressed. The generalizability of the results may be limited by the self-selected nature of the volunteer participants.
It also appears that in menopausal women, 10 weeks is too short a duration of physical activity to produce pronounced and significant changes in either menopausal symptoms across all domains of MENQOL or levels of hormone associated with these symptoms. Further psychometric property development of the Menopause-Specific Quality of Life questionnaire and development of a modified version, the MENQOL-Intervention questionnaire. Vasomotor symptoms and quality of life in previously sedentary postmenopausal women randomized to physical activity or estrogen therapy.
Perimenopausal symptoms, quality of life, and health behaviors in hormone therapy users and nonusers. Symptoms during the menopausal and early postmenopausal transition and their relationship to endocrine levels over time: Observations from the Seattle Midlife Women's Health Study.
Influence of a yoga intervention on musculoskeletal fitness, heart rate,
Introduction
More recently, interest has emerged in the purported benefits of yoga for women coping with the changes associated with menopause. Although the role of estrogen in protection against cardiovascular disease remains ambiguous (Pérez-López et al., 2009), estrogen withdrawal appears to be a factor in increased sympathoadrenal activity (Menozzi et al., 2000) and adrenergic sensitivity (Vongpatanasin, 2009). which can result in increased blood pressure during menopause. Extensive studies have provided strong evidence that yoga practice can lead to improvements in cardiovascular disease index (Innes et al., 2005).
Although typically not as intense as conventional exercise, yoga is an increasingly popular recreational activity, especially among women who make up 72% of the estimated 5.8 million practitioners in the US ("Yoga in America Study. There are from both groups expected to improve flexibility and reduced resting blood pressure and resting heart rate, with a greater effect seen in the yoga group, and weight loss seen in the walking group.
Materials and Methods
Participants attended two testing sessions, one week before the start and one week after the end of the intervention. Participants were familiarized with the use of the HUMAC isokinetic dynamometer for isometric knee extension and flexion. Running intensity and duration were prescribed according to the recommendations of the Canadian Society for Exercise Physiology (CSEP, 2004).
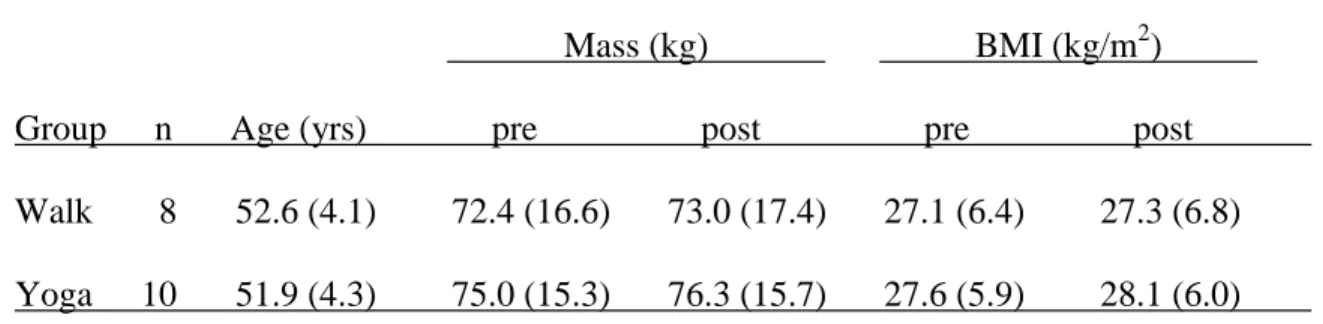
Resting heart rate was measured via palpation of the radial artery and recorded as beats per minute. An independent t-test was used to determine whether there were significant differences between the groups in age, body weight, and body mass index at the beginning of the intervention.
Results
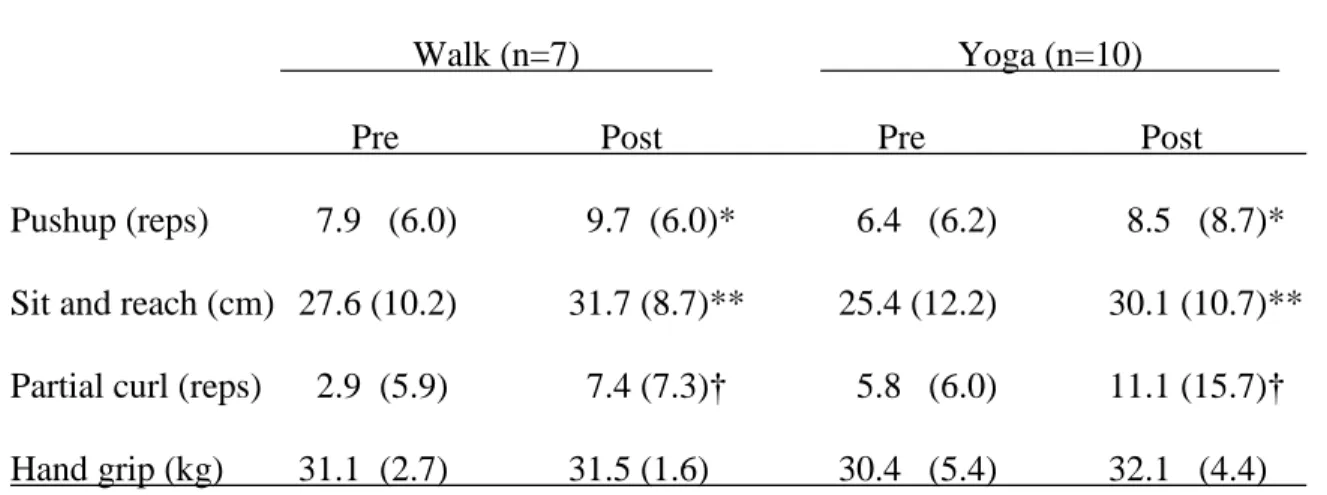
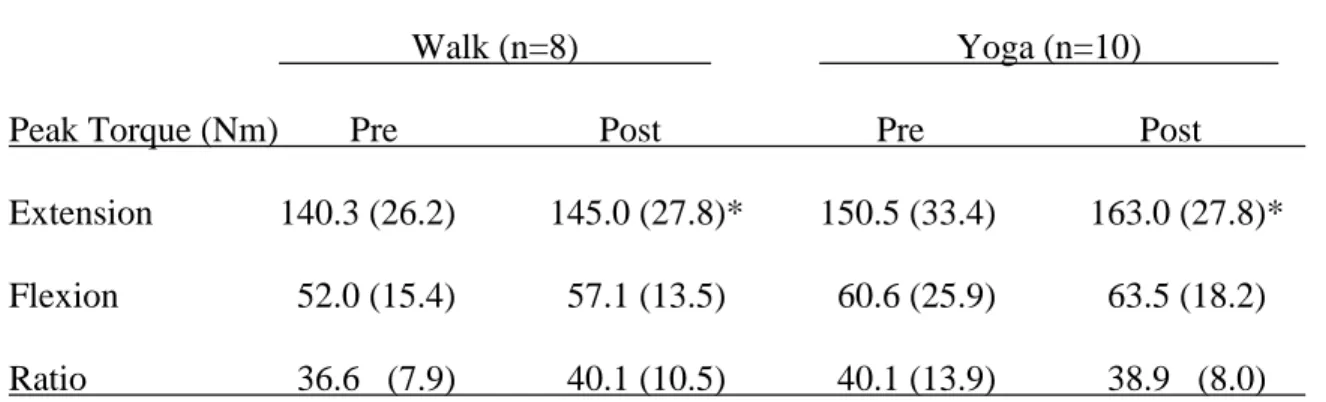
Repeated measures ANOVA was also performed to determine whether time or type of activity affected resting heart rate, blood pressure, or body mass index (BMI). Musculoskeletal fitness assessments from CPAFLA are shown in Table 4.2 and lower body isometric strength measured by isokinetic dynamometry in Table 4.3. The number of push-ups performed increased by two repetitions in both the walking and yoga groups, and the number of partial curls increased by three and four repetitions in the walking and yoga groups, respectively.
Although the yoga group experienced a more significant increase in peak torque than the walking group, 13 vs. 5 Nm, the difference between the groups was not. The walking group experienced a small weight gain of 0.6 kg, while the yoga group experienced a slightly larger weight gain of 1.3 kg.
Discussion
The results support previous research that found that yoga improves parameters of physical fitness (Tran et al., 2001), such as upper and lower body muscle strength and lower body muscle endurance and joint mobility. Reduced body weight was previously observed in one study (Yang, 2007), but remained unchanged in another (Tran et al., 2001). The greater weight gain in the yoga group, although not significant, may be due to the lower intensity of the exercise compared to walking.
Gain in body weight during menopause is typical, with an average of 2.25 kg gained over three years associated with an increase in other risk factors for coronary disease, such as high blood pressure and blood lipids (Wing et al., 1991). Behavioral lifestyle interventions such as dietary changes and physical activity have been shown to mitigate this weight gain (Blanck et al., 2007; . Krumm et al., 2006; Simkin-Silverman et al., 2003), indicating that long-term physical activity is an important component for weight management in menopausal women and that habitual physical activity is essential for this population for weight management and avoidance of comorbid conditions that contribute to cardiovascular disease risk.
Further studies in this population using longer intervention times, greater frequency of practice, sedentary comparison groups and additional measurement criteria such as food intake and body fat percentage would increase knowledge about the effect of yoga in menopausal women. Although not the primary aim of the study, it appeared to be successful in engaging sedentary women in physical activity at a time when the role of activity in health management is critical. The therapeutic potential of yoga practice to alter cardiovascular risk profile in middle-aged men and women.
Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Cardiovascular risk in menopausal women and prevalent related co-morbid conditions: facing the post-Women's Health Initiative era.

Acute effects of a single session of yoga on adrenal androgens in
- Introduction
- Materials and Methods
- Results
- Discussion
- References
Therefore, the aim of this study was to evaluate the effects of a single yoga session on circulating levels of cortisol and DHEA-S compared to a rest session. The results add to already conflicting evidence on the effects of yoga on HPA axis hormones. While a single session of yoga in younger women appeared to result in reduced cortisol, there was no control for diurnal variations (Michalsen et al., 2005).
Increased acute levels of post-exercise dehydroepiandrosterone (DHEA) and cortisol have previously been observed for resistance training in women with 13 weeks of experience (Copeland & Tremblay, 2004), but it appears that 10 weeks of yoga experience may be too short to stimulate changes in the hormonal profiles of menopausal women, or that yoga lacks the intensity required to induce a similar increase. The lack of changes in cortisol levels during a single yoga session also implies that the relaxation response did not alter HPA activity to the extent that a decrease in cortisol was observed.
Discussion and conclusions
Comparing the active yoga session with the rest control session showed that yoga had no effect on circulating levels of these hormones. In addition, yoga poses are intended to be modified according to the needs of the individual practicing it, and it would be the protocol methodology that requires individuals to practice standardized versions of the poses. The study design required participants to limit their activity to the given intervention, and it is possible that the combination of activities had an additive or synergistic effect.
Regardless of the activity chosen, starting physical activity for short-term relief from menopausal symptoms can have long-term consequences if the activity is enjoyable enough to adopt as a permanent lifestyle change. The results of this final project support the claim that yoga can be beneficial to the health of menopausal women, but within 10 weeks these benefits do not differ from those of walking, nor do the benefits appear to be achieved through changes in circulation. levels of the hormones examined.