Using machine learning to adjust immersion therapy intensity of phobia treatment through vital feedback. The proposed method presented in this paper is that a machine learning model can replace the need for continuous human intervention.
Introduction
Statement of the Problem
Blood pressure and heart rate have been shown to be a reliable measure of anxiety in a patient. There is also research that concludes that virtual environments that incorporate a phobogenic stimuli trigger anxiety in patients.
Limitations
The study was done with 26 participants; of which half were phobic, exposed them to phobic stimuli and found that they can induce anxiety in these participants [7]. Since fear causes anxiety in patients and there is a reliable way to measure anxiety in patients through their vital organs, it only makes sense to see if the active role of the vital organs in the intensity of the scene will make a significant difference.
Purpose of the Study
Research Question
Contribution
Virtual reality seems to be the main tool for treating phobias, as it is difficult to find research papers from this century that suggest alternative practices. Machine learning seems like a good answer to this problem as it can be used to create a variance in the environment.
Definitions of Terms
Two different papers suggest that one of the main limitations of the treatment for acrophobia is the lack of variance in the reference points around the user [3].
Organization of the Thesis
Conclusion
- Limitations of Current Procedure
- Relationship of Anxiety and Vitals
- Self Reporting for Anxiety Levels and Acrophobia
- Height threshold for Acrophobia
This review will cover three main categories: the psychology of anxiety and acrophobia treatment, the current state of virtual reality exposure therapy, and machine learning as it relates to predictive modeling. To objectively access a patient's current level of anxiety, blood pressure has been shown to be a good indication, as a positive correlation exists between anxiety, fear and blood pressure [6].
Virtual Reality Exposure Therapy
- Realism in Virtual Reality
- Validity of heart rate during Virtual Reality
- Predictive Models
- Model for Determining Fear Levels Using Psychological Record-
- Machine Learning for Automatic Adjustment of Intensity
- K Nearest Neighbor
Using heart rate as an indicator of fear during a virtual reality experience should not be the only indicator as heart rate naturally increases when a patient is in a virtual reality experience without fear stimuli. Heart rate still increases when exposed to stimuli in virtual reality, compared to being in virtual reality without stimuli [21]. Currently there is a huge range in virtual reality equipment, and this mainly translates to a difference in screen resolution and a smaller difference in tracking.
It has been demonstrated that low-cost virtual reality equipment can be used for meaningful treatment of acrophobia [22] if the patient is not visually impaired; with the exception of visually impaired patients who wear contact lenses [23]. Another thing to consider is the use of whole body tracking, as it has been shown to provide a more immersive experience and encourage patients to interact more with the experience [19]. Support vector machines are commonly used to study nonlinear relationships, but they suffer from improper selection of input variables, and using indistinct variables results in longer training time and higher error compared to using discrete input variables [24]. ].
The most important psychological records to consider are skin galvanic response, heart rate and electroencephalogram [28]. A positive effect was demonstrated when the difficulty of a virtual reality experience was automatically updated using a deep learning model [28] [29].
Datasets for Fear Recognition
Dataset for Emotion Analysis Using EEG Physiological and
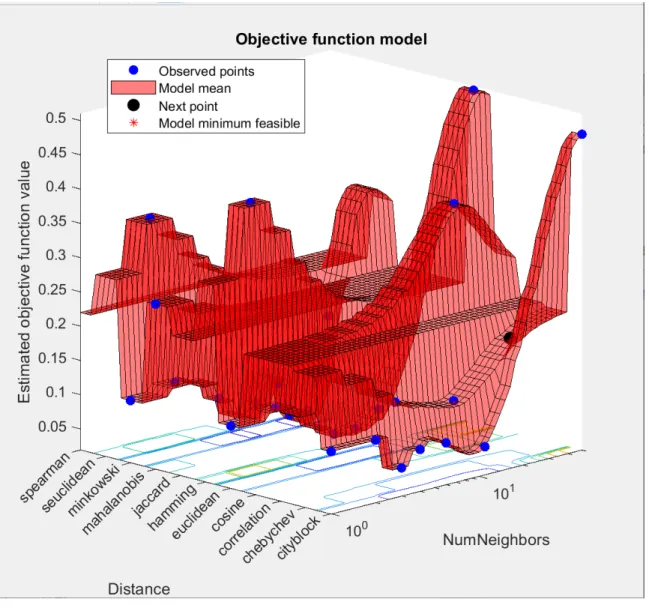
K Nearest Neighbor or KNN is a simple machine learning model that excels at finding correlations when little is known about the dimensions of the input data [31]. It mainly focuses on the Euclidean distance between the input points and the nearest N known points [31]. We can reasonably assume that height plays a role in the fear response, but what about the x and y dimensions. The video list contains 120 one-minute excerpts of music videos and metadata for those videos, including artist, original YouTube link, song title, etc. [32].
All of these are scored using a driving force of 1–9, except for familiarity which was an integer from 1–5 [ 32 ]. The original data contains 32 channels of EEG, 12 channels of peripheral channels, 3 unused channels and a status channel for a total of 48 channels recorded at 512hz [32].
Spider-Fearful Individuals Watching Spider Video Clips Dataset 19
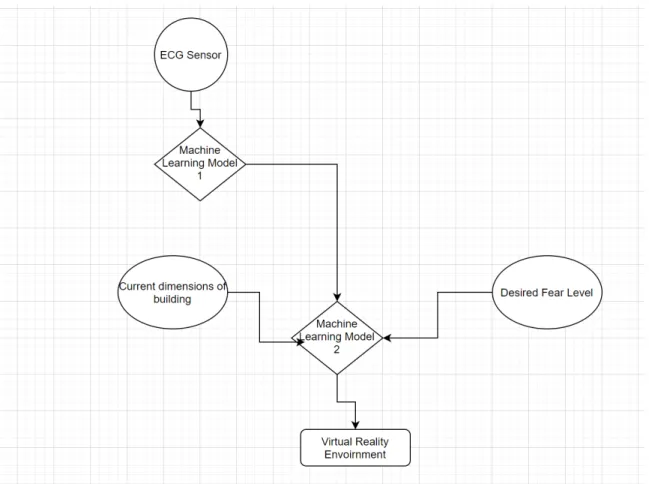
It seems worthwhile to explore the idea of having a few scenes available and having a predictive model to change the intensity of those scenes; an example would be if a patient was found to have a fear of heights tied to bridges instead of developing multiple scenes with bridges at different height levels the model would instead output the desired height value and a scene could change itself to this level. For model selection, a two-model approach seems interesting, one model to translate psychological recordings into fear levels and one to take the fear levels and generate a scene using this information with a random input vector to add some variance to the experience. For psychological recordings, the most useful appear to be the ECG, galvanic skin response, and potential electroencephalogram.
For this research, it is clear that a model that captures the EKG and outputs 4 different levels of fear is possible and promising.
Summary
The aim of this study is to find out whether machine learning is useful, which when combined with exposure therapy has a strong synergistic effect and provides value to the patient in terms of efficiency and effectiveness of the treatment. This section is structured as follows: first the research design is described in detail, which includes the rationale for the methods chosen for this study, then the data collection methods follow, followed by the data analysis methods. This is followed by the software definition and design, followed by the experimental framework, the research validation, the assumptions of the study, the limitations of the study, and finally the summary for this chapter.
Research Design
Data Collection methods
Data Analysis Methods
Software Definition and Design
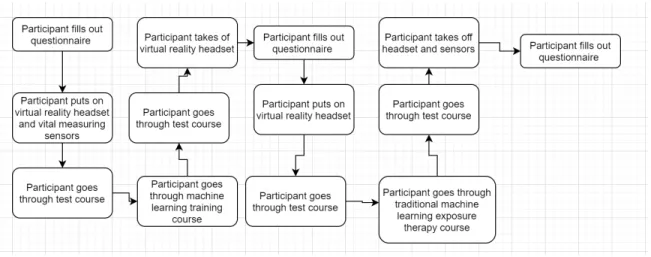
This model will then be output to a Tensorflow compatible model as Unity has great support for this model type. The test course will be a simple course with progressively more scenarios that trigger acrophobia: an example of a basic scenario could be looking over a low edge and could escalate to reaching over the edge of a tall building. The training course will be the section that uses the machine learning model trained earlier to generate a dynamic virtual reality scene from the machine learning model.
The training course would have scenarios similar to the test course, but the height of these scenarios would be dynamically adjusted by the machine learning model.

Experimental Framework
As this is taking place during Covid, there will only be myself instead of having multiple participants.
Research Validation
Assumptions of the Study
Limitations of the study
Summary
This experiment was conducted during Covid 19, so all data collection and testing will be done on myself. It doesn't make sense to repeat this study on myself as there would be diminishing returns. The next part of this chapter will be how the software was constructed and how the testing is planned to be done.
After that, it will be the data collected during the development and experimentation process.
Software Development and Testing Strategy
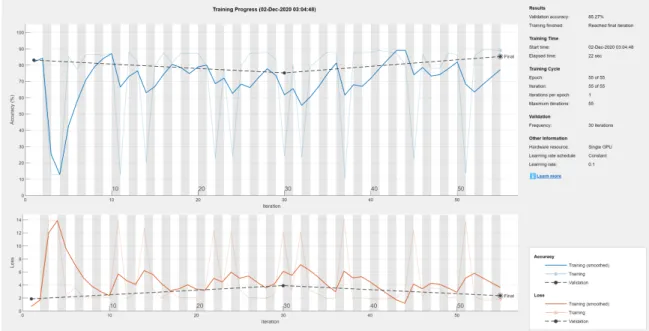
The problem with this data set was that it only identified the participant as fearful or non-fearful, so I ended up calculating the heart rate based on the EKG signals. I chose 4 groups as the "Non-fearful group" was taken from when the participant was resting, the other groups were from the fearful state and was done by summing the heart rates and creating three equal groups where the slightly fearful had the lowest heart rates per minute and the scared lottery had the highest beats per minute since that's what makes the most sense because the more scared you are, the higher your heart rate is. Once clustering was done, it was fed into a neural network consisting of an input layer of 501 neurons (5 seconds of ECG at 100 Hz and heart rate), followed by three hidden layers of 150 neurons each and a classification layer of 4 neurons. one for each of the possible outcomes as discussed earlier).
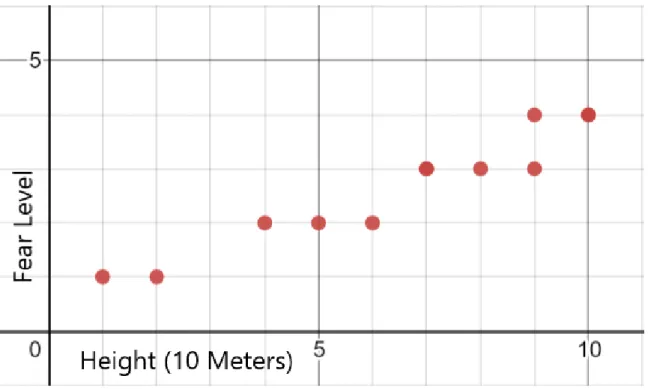
The next model to be trained was the model that generated the building that the participant would stand on top of. This was done by generating buildings of random x,y,z dimensions and recording my average anxiety level for 30 seconds. This was trained using a knn network as this made the most sense as similarly sized buildings would exhibit similar anxiety levels.
This was done by creating a script that had a collection of building models and could modify them in all dimensions and place them in the scene. The testing was carried out in the same way as described in Chapter 3, with the difference that I was the only participant in this study.
Data Analysis
The rest of the software I created was the code that read the ECG data from the sensor and fed it into Unity, this turned out to be trivial as there was a Unity plugin available. For the actual experiment, I was able to progress to a height of 50 meters in 10 seconds before I had to give up due to fear.
Report Findings
Summary
Introduction
Discussion
Conclusion
A dynamic environment is better than someone manually choosing height values for a building during immersion therapy for fear of heights based on the increase in relative height as discussed previously (a 33% increase for the dynamic environment versus the 20% increase for the traditional method).
Recommendations
Deep Learning Toolbox Version 14.1 Image Processing Toolbox Version 11.2 Parallel Computing Toolbox Version 7.3 Signal Processing Toolbox Version 8.5. Assessment of patient's anxiety and expectation related to hemodynamic changes during surgical procedure under local anesthesia.Revista de Odontologia da UNESP. Anxiety and presence during vr immersion: A comparative study of the responses of phobic and non-phobic participants in therapeutic virtual environments derived from computer games.
In Proceedings of the 22nd ACM Conference on Virtual Reality Software and Technology, VRST ’16, pages 315–. Automated psychological therapy using immersive virtual reality for the treatment of fear of heights: a single-blind, parallel-group, randomized controlled trial. The differential effect of neutral and fear-stimulus virtual reality exposure on physiological indicators of anxiety in acrophobia.
Efficacy of self-guided application-based virtual reality cognitive behavioral therapy for acrophobia: a randomized clinical trial. A survey of various machine and deep learning techniques applied in automatic fear level detection and acrophobia virtual therapy, January 2020.