Subclinical neck pain (SCNP) is defined as recurrent pain and stiffness in the neck for which individuals have not yet sought treatment. Two paradigms were designed to assess upper limb movement, one study in the horizontal plane and the other in the vertical plane.
List of Tables
List of Abbreviations
Introduction
This differs from feedback processing which uses sensory information to regulate limb motor output (Kandel et al., 2000). Glazebrook et al., (2006) used spatial variability to compare kinematic differences in upper limb targeting between individuals with and without Autism Spectrum Disorder (ASD).
Review of Literature
- Introduction
- Two-Component Process of Aiming
- Neuroanatomy of Upper Limb Movement
- Lateral Differences in Aiming
- Subclinical Neck Pain (SCNP)
- Measurement of Fatigue
- Summary
Vermis and intermediate hemispheres receive somatosensory information from the spinal cord (Kandel et al., 2000). Furthermore, vestibular information is transmitted from the neck to the flocculonodular lobe of the cerebellum (Kandel et al., 2000).
Study One Manuscript
Introduction
- Methodology
- Participants
- Apparatus
- Procedure
- Data Analysis
- Performance Analysis
- Statistical Analysis
- Results
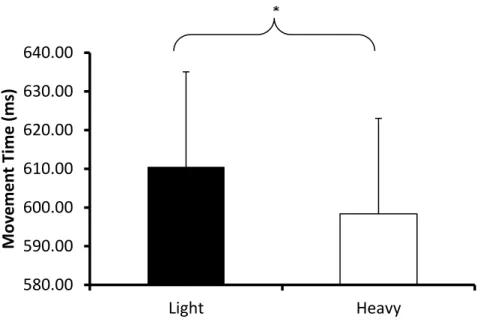
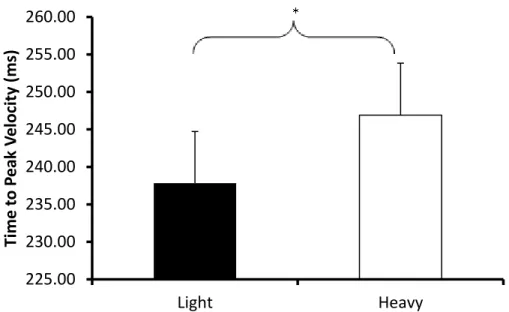
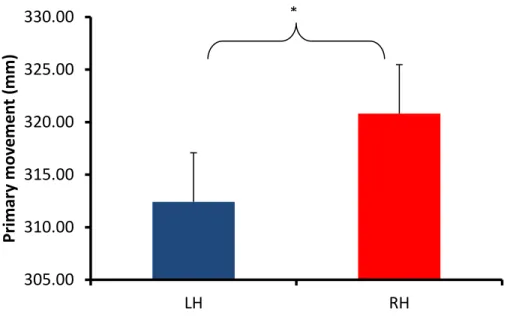
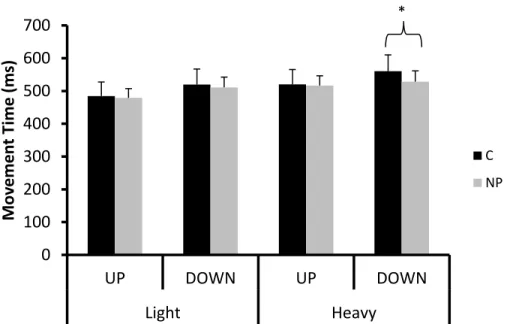
The study found no differences in movement time between the pens and found that the heavy pen took less time to reach peak speed compared to the light pen. Movements in the non-dominant arm resulted in a shorter distance traveled for the primary movement endpoint compared to the dominant arm. Thus, greater spatial variability in peak deceleration in the non-dominant arm indicates a greater tendency to use feedback towards the end.
Studies have shown that this hemispheric system favors feedback processing (Goodale et al., 1990; Fisk & Goodale, 1988). This finding is exacerbated in the non-dominant arm, indicating a greater time required to form internal models. More specifically, output to the motor cortex has been shown to be affected in those with SCNP (Baarbé et al., 2018).
Study Two Manuscript
Introduction
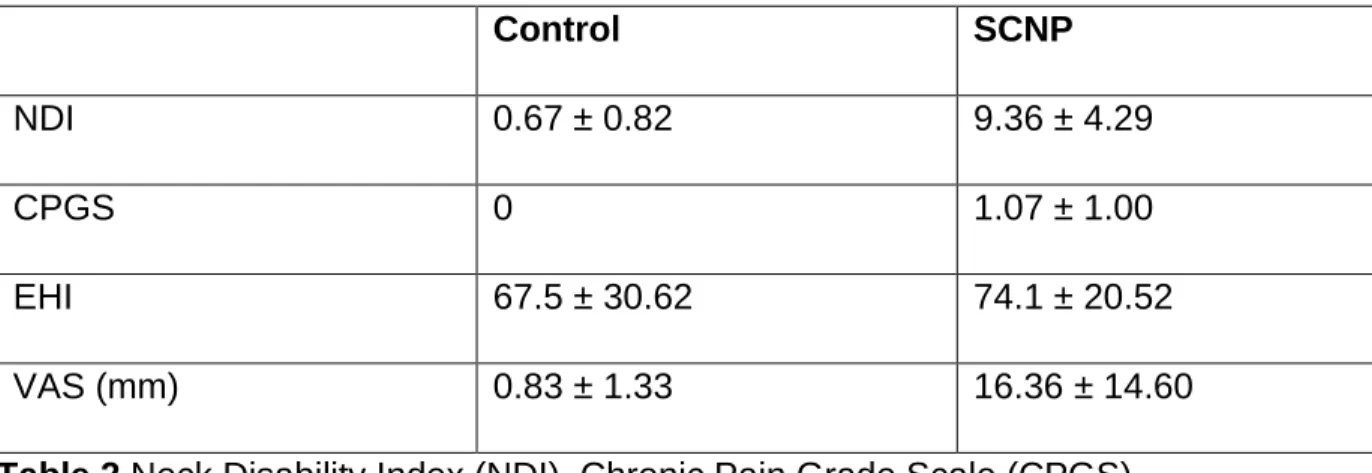
With the increasing use of technology, neck pain has become a growing problem, affecting approximately 30-50% of people (Hogg-Johnson et al., 2008). Those with SCNP experience recurrent neck pain and stiffness but do not seek medical treatment (Lee et al., 2005). Previous research from our laboratory has demonstrated altered cerebellar processing in humans with SCNP ( Daligadu et al., 2013 ).
The cerebellum has also been shown to update internal models using feedback information ( Popa et al., 2013 ). Previous studies have shown that those with SCNP have a greater tendency to rely on visual feedback, perhaps to compensate for their altered body schema (Harvie et al., 2015). This is especially true with downslope motions, as overshoot corrections must be made against gravity (Lyons et al., 2006).
Methodology
- Participants
- Apparatus
- Procedure
The height of the monitor was adjusted so that the position of the house was placed at the participant's eye level. Participants were given prior knowledge of the stylus they would be using before starting it. A solid body was attached to the top of each stylus and digitized at the tip of the pen.
Before starting the experiment, the experimenter asked the participant to rate their perceived level of neck fatigue; and shoulder and arm of the starting limb using the Borg CR-10 scale. Participants were asked to rate their perceived level of fatigue at the end of each block in each of the aforementioned categories. Onset trials began when participants placed the pen at the start position.
Data Analysis
- Performance Analysis
- Statistical Analysis
Before data output, trials in which IRED visibility was disrupted and participants expecting movements were removed (approximately 9% of the total trials). The main dependent variables were movement time (MT), time to peak velocity (TTPV), time after peak velocity (TAPV), primary movement endpoint in the direction of movement (PSM), constant error (CE), variable error (VE; standard deviation from CE) and reaction time (RT). In addition, trajectory variability was examined using the variables PA, PV, PD, and END (Khan et al., 2002).
In addition, outliers were removed (approximately 1 % of total trials) according to Grubb's test performed on movement time and constant error. Statistical analyzes were performed on dependent variables a two group (SCNP and control) by two hand (dominant and non-dominant) by two stylus (light and heavy) by two direction (up and down) mixed factors ANOVAs, with repeated measures on the last three factors. One exception was the analysis of trajectory variability at kinematic landmarks comparing two groups (SCNP and control) by two hands (dominant and non-dominant), by two stylus (light and . heavy), by two directions (up and down) using kinematic marker (PA, PV, PD and END) repeated measures ANOVA.
Results
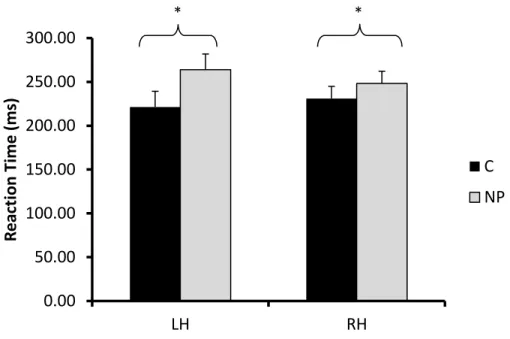
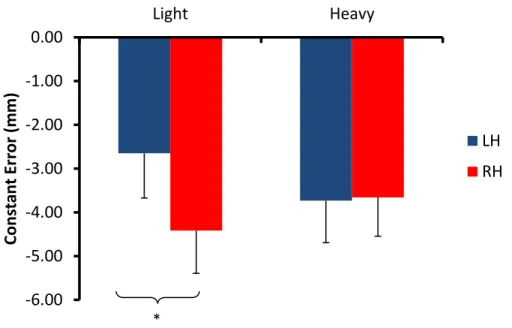
These effects were offset by a three-way interaction between stylus, direction and hand (F p < 0.05, ŋp2 = 0.245), where movements with the light stylus using the non-dominant arm in the upward direction achieved a higher peak velocity (889 mm / s) compared to the downward direction (832 mm/s). Accordingly, the reaction times performed by the non-dominant arm with the light stylus were greater in the downward movement (271 ms) compared to the upward movement (255 ms), while the reaction times performed by the dominant arm with the heavy stylus were longer in the downward movement (265 ms) compared to the upward movement (251 ms). Accordingly, in the non-dominant arm, controls had greater target undershoot with the light stylus (-1.49 mm) compared to the heavy stylus (-0.32 mm), while the dominant arm in the SCNP participants had a greater undershoot of target with the light stylus (-1.94 mm) compared to the heavy stylus (-0.74 mm) (Figure 15).
Movements with the light stylus were more variable at peak velocity in the non-dominant arm (13.75 mm) compared to the dominant arm (11.39 mm), while movements with the heavy stylus were more variable at peak delay (20.91 mm) in the non-dominant arm. -dominant arm compared to the dominant arm (16.77 mm). It showed higher peak velocities with the light stylus in the downward direction in the dominant arm (883 mm/s) compared to the non-dominant arm (832 mm/s). This interaction was also observed with the heavy stylus in the upward direction (dominant = 802mm/s, non-dominant = 770mm/s) and the downward direction (dominant = 813mm/s, non-dominant = 774mm/s).
Discussion
Participants illustrated a shorter distance traveled in the primary movement with the heavy stylus compared to the results of Burkitt and colleagues (2015). This study demonstrated longer movement time, time to reach peak velocity, and time after peak velocity in the non-dominant arm compared to the dominant arm. Additionally, the non-dominant arm illustrated a shorter distance traveled in the primary endpoint of the movement.
The constant error (i.e., mean endpoint location) of non-dominant arm movements was more towards the center of the target compared to the dominant arm, although more variable in nature. Conversely, faster movement times with the dominant arm resulted in endpoint accuracy less than the center of the target. Therefore, Borg's assessment of perceived fatigue analysis was presented at the beginning of the study for 17 of the 23 participants (Borg, 1990).
General Discussion
In the first study, we demonstrated differences in handedness that are consistent with previous literature suggesting that the nondominant system tends to use feedback processing in goal attainment ( Goodale et al., 1990 ; Fisk. & Goodale, 1988 ). Directional effects were also consistent with previous literature, illustrated by increased time spent after peak velocity with the heavy stylus in the downward direction. A possible reason for this may be due to the familiarity of the task in the initial study.
Movements performed in the vertical plane are more complex and require the formation and use of new internal models to accurately reach the target. Handedness effects indicate a greater propensity for the non-dominant arm to spend more time using feedback processing to accurately reach the target indicated by longer time spent following peak velocity and greater deficits in the primary movement endpoint. Directionality by styli effect illustrated longer time spent after peak velocity in the downward direction, perhaps to avoid energy-costly overshoots.
The role of the right hemisphere in the interpretation of figurative aspects of language. A positron emission tomography activation study. Patients with chronic neck pain exhibit altered patterns of muscle activation during performance of a functional upper limb task. The effects of unilateral brain damage on visually guided span: hemispheric differences in the nature of the deficit.
The direct connections of the C2 dorsal root ganglia in the Macaca irus monkey: relevance to the chiropractic profession. A kinematic analysis of how young adults with and without autism plan and control goal-directed movements. Relationship between perceived exertion and average power frequency of the EMG signal from the upper trapezius muscle during isometric shoulder elevation.
Appendix
This questionnaire has been designed to provide information to your therapist about how your neck pain has affected your ability to cope in your daily life. Please answer each question by checking ONE box that applies to you. We understand that 2 statements may describe your condition, but please check only ONE box that most accurately describes your current condition.
Chronic Pain Grade Scale Pain intensity items
Disability points
Disability days (0-180) Disability score (0-100)
A new conceptual model of neck pain linking onset, course, and care: the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and its Associated Disorders. Can you think of an accident or other event that caused pain or stiffness?
Safety checklist
Please note, if you are taking medication or using recreational drugs, please read the medication list on the next page to see if you are using a contra-indicated medication or medication. You do not have to tell the researcher what medicine or medications you are using unless you want to. However, all researchers have signed confidentiality agreements and this information will not be recorded in writing if you wish to discuss this matter.
Regular use of cannabis more often than once a week and/or use of cannabis in the last 4 days.
Chiropractic Adjustment Safety Checklist
You will have the opportunity to review the study details and ask any questions before participating. If you are not randomized to the treatment intervention, you will be given an additional assessment at the end of the study (to determine if you would benefit from chiropractic care) and offered free treatment. Only safe, high-speed, low-amplitude conventional manipulation techniques will be used in this study.
If you are not interested in this option or are not enrolled in any of the eligible courses, you will be compensated with two. If you have neck pain and you are randomized to the no-treatment group, you will receive a free assessment and treatment at the end of the study. The data collected in this study will be coded so that it is confidential and will remain.