In the nonclinical group, none of the facets of spirituality moderated the relationships between religiosity and fundamentalism or moral TAF. Siev, Chambless, and Huppert (2010) examined religious affiliation as a moderator of the relationship between Morale-TAF and obsessions and compulsions in a student population. Level of religiosity was unrelated to any of the outcome variables and did not moderate the association between religious affiliation and OCD symptoms or obsessive-compulsive cognitions.
Much of this inconsistency is likely due to the continued inadequate measurement of the concept of religiosity/spirituality in the literature. The vast majority of the research literature examining the relationship between religiosity/spirituality and cognitive features of OCD has used the construct of TAF. However, including this moderator in the model only explained an additional 0.9% of the variance.
The positive relationship between religious crisis and the order subscale of the OCI-R (r = .260) approached a medium effect size. The negative relationship between religious involvement and the hoarding subscale of the OCI-R (r = -.251) approached a medium effect size. However, most of the effect sizes of the relationship between measures of religiosity/spirituality and the OCI-R total score and its subscales were of a trivial or small size.
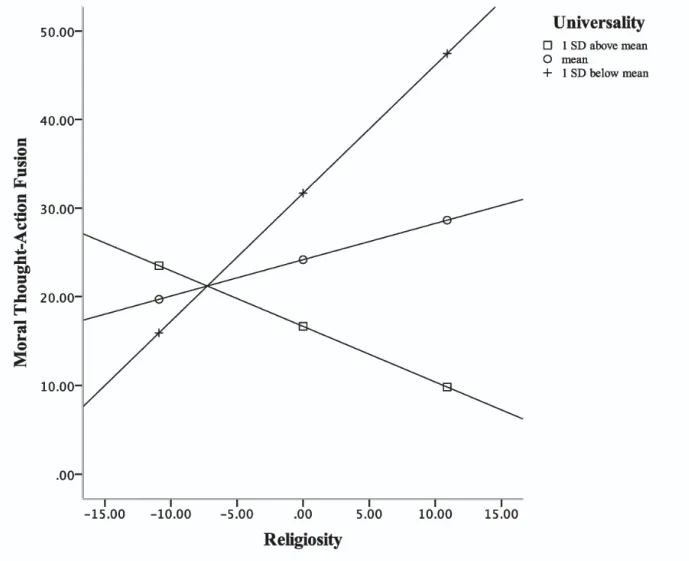
None of the relationships between measures of religiosity/spirituality and the OCI-R and its subscales were statistically significant. Religious fundamentalism was positively associated with the controlling subscale of the OCI-R and evidenced a medium effect size. Spirituality (ASPIRES – STS – Total) was not a significant moderator of the relationship between religiosity (ASPIRES – RSS – RI) and conscientiousness (PIOS).
In the non-clinical sample, the hypothesis was supported in that all mediation analyzes were significant. In a non-clinical sample, relationships between measures of religiosity/spirituality and compulsions (OCI-R) were generally of small effect sizes, with the exception of positive relationships with religious crisis and compulsion subtypes, which were typically medium or near medium effect sizes. The purpose of the current research is to clarify the relationship between religiosity/spirituality and cognitive factors and OCD symptoms given the mixed results of past research and the inadequacy of measuring the religiosity and spirituality constructs common in past research.
In the non-clinical sample, all proposed mediators were statistically significant and the effects were medium in size. For the clinical group, none of the proposed mediators were statistically significant (and this is not unexpected given the small sample size). In the clinical sample, none of the proposed mediators were statistically significant (which is not surprising given the small sample size).
In the nonclinical sample, only religious crisis was significantly positively associated with some coercive subtype scales of the OCI-R.
DO NOT WANT TO TAKE PART IN THE STUDY, ARE THERE OTHER CHOICES?
If you volunteer to participate in this study, you will be asked to complete a questionnaire package online via computer. However, the information gained from this study may help us provide better treatment for patients with anxiety in the future. Your data will not be passed on to anyone except with your consent or in accordance with the law.
All personal information such as your name, address, phone number, OHIP number, family doctor's name will be removed from the data and replaced with a number. The list linking the number to your name will be stored in a secure location separate from your file. The data will be securely stored in a locked office in the research laboratory, with identifying information removed.
For the purposes of ensuring appropriate monitoring of the research study, a member of the Hamilton Integrated Research Ethics Board (HIREB) may review your research data and medical records. However, no records identifying you by name or initials will be allowed to leave the hospital. If, for any reason, you are admitted to another hospital or die of natural or other causes while participating in this study, we will request your medical records to collect information relevant to your participation in the study.
If the results of the study are published, your name will not be used and no information that reveals your identity will be released or published without your specific consent for disclosure. However, it is important to note that this original signed consent form and the information that follows may be included in your medical record. If you volunteer to participate in this study, you can withdraw at any time, which will in no way affect the quality of care you receive at this facility.
The investigator may withdraw you from this research if circumstances justify it.
BE PAID TO PARTICIPATE IN THIS STUDY?
Religiosity, magical ideas, and paranormal beliefs in anxiety disorders and obsessive-compulsive disorder: a cross-sectional study. Consistency between self-report and clinician-administered versions of the Yale-Brown obsessive-compulsive scale. Transcultural aspects of obsessive-compulsive disorder: a description of a Brazilian sample and a systematic review of international clinical studies.
Interrater reliability of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID I) and Axis II Disorders (SCID II). Scrupulosity and obsessive-compulsive symptoms: confirmatory factor analysis and validity of the Penn Inventory of Scrupulosity. Empirical and conceptual value of the Spiritual Transcendence and Religious Involvement Scale for personality research.
The utility of the assessment of spirituality and religious sentiments (ASPIRES) scales with Christians and Buddhists in Sri Lanka. Development and initial validation of the Obsessive Beliefs Questionnaire and the Interpretation of Intrusions Inventory. Obsessive-compulsive symptomatology, religiosity levels, and the illusion-of-control paradigm in a nonclinical undergraduate sample.