www.elsevier.es/rmuanl
SCIENTIFIC
LETTER
Askin
tumor:
Case
report
and
literature
review
R.G.
Cueto-Ramos
a,
A.N.
Ponce-Escobedo
a,∗,
C.A.
Montero-Cantú
a,
G.E.
Mu˜
noz-Maldonado
a,
E.
Ruiz-Holguín
b,
N.
Vilches-Cisneros
baGeneralSurgeryServicesatthe‘‘Dr.JoséEleuterioGonzález’’,UniversityHospitaloftheUANL,Monterrey,Mexico
bDepartmentofPathologicalAnatomyatthe‘‘Dr.JoséEleuterioGonzález’’,UniversityHospitaloftheUANL,Monterrey,Mexico
Received9July2015;accepted7September2015 Availableonline2May2016
KEYWORDS Askintumor; Neuroectodermal tumor;
Primitive
Abstract Askintumorisanuncommonmalignantneoplasmofaneuroectodermicoriginthat arisesfromthesofttissuesofthethoracopulmonarywall.DefinedhistologicallybyAskinand Rosaiin1979asamalignantsmallroundcelltumor.Itisdescribedwithinagroupofmalignant neoplasmswithanaggressivebehavior.Thelackofclinicalguidesthatestablishastandardized managementcontributestoitspoorprognosisandshortoverallsurvival.Onceaprimitive neu-roectodermaltumorhasbeendiagnosed,treatmentwillconsistofamultimodalmanagement. ©2016UniversidadAut´onomadeNuevoLe´on.PublishedbyMassonDoymaM´exicoS.A.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
Askintumorisanuncommonmalignantneoplasmofa neu-roectodermaloriginthatarisesfromthesofttissuesofthe thoraco-pulmonarywall.1HistologicallydesignatedbyAskin
andRosaiin1979asamalignantsmallroundcelltumor,2it
isdescribedwithinagroupofmalignantneoplasmswithan aggressivebehavior,classifiedbytheWorldHealth Organiza-tion(WHO)in2002asEwing’sSarcoma/PeripheralPrimitive NeuroectodermalTumor(SE/PPNETS),organizingtumorsof neuroectodermal, bone and soft tissue origin as a single
∗Correspondingauthorat:ServiciodeCirugíaGeneraldelHospital
Universitario‘‘Dr.JoséEleuterioGonzález’’,UniversidadAutónoma
deNuevoLeón,Av.FranciscoI,MaderoyAv.Gonzalitoss/n,colonia
MitrasCentro,C.P.64460Monterrey,Mexico.
E-mailaddress:[email protected](A.N.Ponce-Escobedo).
entity.Ewing’ssarcomaofthebone,neuroepithelioma, neu-roblastomaandperipheralprimitiveneuroectodermaltumor (PNET),areneoplasmsincludedinthisgroup,andwithinthe PNETs,theAskintumor.3
Accordingtomedicalliterature,thereisagreater inci-dence in younger patients.1---6 It presents a non-specific
clinical behavior, making its precise diagnosis difficult in its early stages.2---6 Its high rate of local recurrence and
the lack of clinical guidelines which establish a stan-dardizedmanagement contribute toa less thanfavorable prognosis and a short survival rate.4 Due to late
diag-noses, large size masses are found, which compromise thetumor’ssurgical resectionbecauseof thepresence of adjacent vital anatomicstructures.1 There are,however;
studies proving a higher survival rate in patients treated with neoadjuvant chemotherapy followed by a surgical approachand postoperativeradiotherapy.5,6 The
contribu-tionmadebyDemiretal.onsurgicaltreatmentclarifiesthe
http://dx.doi.org/10.1016/j.rmu.2015.09.003
1665-5796/©2016UniversidadAut´onomadeNuevoLe´on.PublishedbyMassonDoymaM´exicoS.A.Thisisanopenaccessarticleunderthe
need for a multimodal management,showing that induc-tionwithchemotherapycontributestotumor-freeresection margins.5
Clinical
case
A25-year-oldmalewithabackgroundofactivesmoking(12 packs/year),isadmittedafterpresentingintermittent pleu-riticpain in the lefthemithorax, of variableintensity, of atwo-monthevolution; accompanied bya non-productive cough, non-quantified fever and a 10kg weight loss in a course of three months, without a history of occupa-tionalexposurehemoptysis or wheezing.Patient refersto have received a previous ambulatory treatment with sul-famethoxazole/trimethoprim,clindamycinandlevofloxacin for7dayswithoutimprovement.Duringphysical examina-tion,we observed ina central trachea,cylindricalthorax and symmetric respiratory movements without the use of accessory muscles and with no evident or palpable masses. At auscultation, a reduced vesicular murmur is foundin thebase of thelefthemithorax,withnoclinical data added. Blood studies were within normal parame-ters.ThoracicX-raysareperformed,wherearadio-opacity is found in the left hemithorax with effacement of the costophrenic angle (Fig. 1). Computed contrasted tomo-graphy of the thorax showed the presence of an extra pulmonarytumor(17.6cm×12.6cm×11.3cm),dependent on soft tissue of the left thoracic wall, extending from the fourth to the twelfth posterior costal arches, with a heterogeneousrise of the contrastmaterial, without evi-dence of mediastinal adenopathies (Fig. 2). An incisional biopsy is performed through a left posterolateral thora-cotomywith atrans-operatory histopathological reportof aslightlydifferentiatedmalignantneoplasia. Ourpatient courses witha post-operative evolution with no negative eventualities. After performing a definite histopatholog-ical analysis, the presentation of a confirmed primitive neuroectodermal tumor through the presence of small roundcells is described (Fig. 3), with immunohistochem-ical markers positive for FLI-1 and CD99, and negative for cytokeratin, vimentin, TdT, CD45, CD43 and CD56,
Figure1 ThoracicX-rayatthetimeofadmission.Radiopacity inthelefthemithoraxisobserved.
Figure2 ContrastedthoracicCATscan.Tumordependenton thesofttissueoftheleftthoracicwall.
Figure 3 Panoramic view at 5× of the neoplasmic lesion
composed of small cells,round and blue, between septa of connectivetissue.
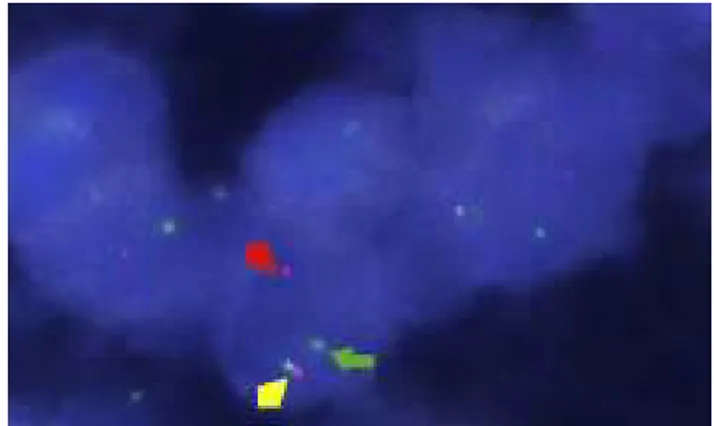
with a positive flurosescence in situ hybridization (FISH) for rearrangement of the EWSR1 gene (Fig. 4). Oncologi-cal management with chemotherapy is started, under an alternate scheme using: vincristine 2mg/m2, doxorubicin
75mg/m2,cyclophosphamide1200mg/m2(Day1)with
ifos-famide 1800mg/m2 and etoposide 100mg/m2 (Day 1---5)
every 3 weeks, dosage dependent on patient’s tolerance underradiographiccontrolofthetumor.Atthetimeofthe edition of this article, the patientis stable, receivinghis firstcytotoxiccycle,andexpectingareductioninthesize ofthetumor,thusmakingresectionofthelesionpossible.
Discussion
Despitetheadventofnewdiagnostictechniquesandtools, Askintumorhasmaintainedalowincidencesinceitwasfirst described,whichmakesuswonderaboutthefactors associ-atedwiththeonsetoftheresponsiblegeneticmutation.
Figure4 Break apart-typeFISHtestfor therearrangement ofEWSR-1.Inthistest,2redsignalsand2greensignalscanbe observed.Thetestispositivewhentheredandgreensignals areseparated.
conformationstheyshow,differentiatingfromoneanother by their degree of neuroectodermal differentiation. They alsopresentchromosomictranslocation(11;22)(q24;q12) which fusion expresses the gene EWS/ETS or EWS/FL1.3
Thischimericalgeneisobservedin85%ofSE/PPNETgroup tumors, making its determination a crucial tool in the cytogeneticdiagnosis.7
Itsincidenceis greaterin males,and80%of diagnosed patients are under 20 years of age; however, there are reported cases of elderly patients.1 The most common
causesofdeathareassociatedwithlocalrecurrence,distant metastasesandinfiltrationofthepulmonaryparenchyma.1,4
Among themostrecent reports,Contesso etal.showed a generalsurvival rateof 14% at6 yearsanda disease-free survivalrateof17%at6years.8
The clinical picture usually describes ambiguous symp-tomsincluding:apalpablemassinthethorax,eitherpainful or painless (the most common finding),1,9 pleuritic pain,
dyspnea,fever,cough andweightloss,generallyof insidi-ousonset6monthspriortodiagnosis,and,lessfrequently, Horner’ssyndrome.1,2,8,10Thelackofclinicalsuspicionoften
leads to an erroneous diagnostic impression, treating the patientinitiallyasapleuraleffusion.10Unlikethereportsof
aclassicpresentation,inthecaseofourpatientwedidnot observeapalpablemassasaninitialsymptom,despitethe dimensionofthetumormass.Nevertheless,itpresentsthe characteristic ambiguous symptomatologyassociated with thechronicevolutionoftheclinicalpicture.Furthermore, we pointouttheimportanceof consideringtumorsof the softtissueofthethoracicwallwithinthedifferential diag-nosisinthosepatientswhosesymptomatologyiscompatible withthatof anunresolvedinfectiousprocess.Fewstudies evaluatingtheradiologicalcharacteristicsofthistumorhave beenconducted.However,theaidofacomputed tomogra-phy(CT)scanormagneticresonanceimaging(MRI)iscrucial todeterminetheextent,thepossiblepulmonaryinvasionof the tumor, and invasion of local and distal structures, as well asresponse totreatment.4 Findings by CTwith
con-trastinclude:asoft-tissue-dependentmass,usually>5cm, withdisplacementoftheadjacentstructures,accompanied byaheterogeneousriseofthecontrastmaterial.The pres-ence of calcifications, lymphadenopathies, necroticareas andhemorrhagesarelessfrequent findings.Regardingthe
MRI,massesof intermediatetohyperintense intensity are described, located in T1 and T2, with a heterogeneous risewhencontrastdye wasappliedin thenecroticareas. AlthoughSabateetal.concludedthatradiologicalfindings ina CTandMRI arenotspecific andareindistinguishable fromothermalignanciesofthethoracicwall.4Regardingour
patient’simagingassessment,performingasystemicreview ofthethoracicX-raywashighlybeneficial,henceitpresents anhomogeneousradiopacitywithcleanedgesandsuperior convexity,thatinretrospectionisofgreatimportancewhen thereissuspicionofathoracictumor.
The periosteumandsofttissuesfromthe thoracicwall are typically involved, with extension to the pleura and pulmonary parenchyma.1 There are reports of cases with
distantmetastasestodistallongbones,bonemarrow,liver andthe centralnervoussystem (CNS). The neuroectoder-maloriginofthetumorexplainstheinvasionofsympathetic chainganglia,resultinginatypicalpresentations.10
Diagnosticprecisionisunavoidable,becausethechoice oftherapeuticmanagementdependsonit.Thetumorsare solid, circumscribed, opaque brown with focal areas of necrosisandhemorrhage.3Histologically,weareabletofind
thedemonstration of round, small,slightly differentiated cellsorganizedinstrands.2Also,itispossibletoidentifythe
presenceofpseudorosettesaswellastheabsenceoffixation oraweakfixationtoperiodicacidSchiffstains(PAS).With theuseofelectronicmicroscopy,weareabletoobservethe presenceofneurosecretorygranules,inadditionto under-developedcytoplasmicorganelles.11
The immunohistochemistry in this tumor in particular provides a definite base in the differential diagnosis in relation to the variety of malignancies within the group of tumors in round and small cells, such as: neuroblas-tomas, rhabdomyosarcoma and non-Hodgkin’s lymphoma, chondrosarcomaandretinoblastoma.11
The neuroectodermalorigin canbe confirmedwiththe presence of immunohistochemical markers with a posi-tive result for CD99, FLI1,NSE and vimentin. TdT, CD45, LCA,EMA,cytokeratin,desminandactin markersmustbe includedintheimmunohistochemicalpanelinorderto per-forman exclusion of other round-cell malignancies. CD99 (mic-2)proteinis found in the cellularmembrane consis-tentlyinneoplasmsofneuroectodermalSE/PPNETSorigin. Itishighlysensitive,butunspecific,thusitmustbeusedas acomplementwithotherimmunohistochemicalmarkers.12
Fluorescenceinsituhybridization(FISH)andthe amplifi-cationofgenomicparticleswithapolymerasechainreaction (PCR) are necessary as complementary tools for chromo-somictranslocationdetection (11;22)(q24; q12),which is present in 95% of the cases of theseneoplasms.6 Despite
thefact thatthereis nostandardized study algorithm,in ourpatient,differentdiagnosticmodalities,aswellas mul-tidisciplinarywork,wereincluded.However,similartowhat hasbeendescribed, thehistopathologicalreportwas con-firmatory, highlighting the presence of small round cells andimmunohistochemicalmarkersfor CD99,withthe cor-respondingstains, whichallowsus tomake adiagnosis by exclusion,aswellasthepositiveFISHfortherearrangement oftheEWS/FL1geneidentifiedinthiscase.
Atfirst,thetreatmentofthispathologywasperformed throughasurgicalapproach.2Evenwhendifferentattempts
beenmade,trustworthystudiesproposingadefinitescheme arefew.Treatmentsnowadaysarebasedonfindingswhich have marked a milestone in multimodal use, including neoadjuvant chemotherapy schemes as well as systemic treatmentforeverycase,inconjunctionwithlocaltherapy basedonsurgicalresectionand/orradiotherapy.1,6
The choice of these treatment modalities is based on each patient individually. Neoadjuvant chemotherapy reduces the possibility of microscopic residual disease, increases the possibility of a complete resection and increases the disease-free survival rate.5 Sirivella et al.
placeanemphasisonthenecessityofmakinganearlystage diagnosisthroughtheuseofafineneedlebiopsy,beforeany surgicalresection.Theyreportanextensionofsurvivalfree ofdiseaseof10yearsuponimplementingtheuseof neoad-juvantchemotherapy,inupto84%ofpatientswhosetumors were found when the disease did not present metastatic spread,comparedtothosewhopresentedmetastaticspread andcostovertebralcompromise,whoshowedasurvivalrate of33% at 10 years.Patientswhoshowed a poorresponse tochemotherapywerebenefittedbytheuseoflocal radio-therapywiththegoalofreducingthesizeofthetumor.13
Thesurgicalapproachisessentialinthemanagementand removalofthetumor, andfacilitating directradiotherapy withlessexposure.Veronesietal.madeasummaryofthe benefitsofapplyingaggressiveneoadjuvantchemotherapy treatment in comparison to postoperative chemotherapy, suggesting that thereis a reductionof the intraoperative riskoftumorruptureanddisseminationofthetumorcells, making a complete surgical resection possible.14 Surgical
resectionfollowingneoadjuvantchemotherapyallows neg-ativemarginsof71%,comparedtothe37%ofpatientswho aresubjectedtosurgeryasaninitialapproach.12
Surgical strategy should consist of making a radical resection of the tumor mass, including the costal level involved, aswell asthe adjacent inferior or superior rib, circumscribed muscle and adherent soft tissue, procuring tumor-freemarginsof3---4cm,andreconstructingthe tho-racic wall withflaps or muscular tissue.12 In cases where
the pulmonary parenchyma is compromised, a lobectomy orpneumonectomyshouldbeperformed,ifthecasemerits it.Theimportanceofacompletesurgicalresectionisthat itprolongsdisease-freesurvival,althoughdevelopmentof localrecurrenceswillremainconstant.5
Thechemotherapyoutlinesusedhavebeentestedin dis-tinctstudies withthe intentof homogenizingan effective treatment.Outlinessimilartothoseusedtotreat Ewing’s Sarcomahavebeenused,whichareperformedthroughthe useofvincristineat1.5---2mg/m2,doxorubicinat40mg/m2,
cyclophosphamide at 1200mg/m2 and Actinomycin D at
1.25mg/m2(VACA)orvincristine,adriamycinandifosfamide
at1800mg/m2andEtoposideat100mg/m2,accordingtothe
protocolstudiedatEICESS92,withcyclesevery3weeks.6,15
Radiotherapy is used asan aid in the local control of theprimarylesion,posteriortosurgicalresection,withthe aimofeliminatinganyfragmentofthedisease.Treatment shouldbedirectedtoavoid adosewhichwoulddamagea nearorgan.IntheCESS81,CESS86andEICESS92studies, theuseofpostoperativeradiotherapy,includingitsuse as alocaltreatment, showedfavorable resultsin relation to localrecurrence.Currently,thedoseusedinradiotherapyis from20to60Gy.6,15
Diagnosticagehasbeendeterminedinmultiple studies tobeafactor in anegativeprognosis,considering an age over18tobearisk.Poorresponsetoinitialchemotherapy andthepresenceof pleuraleffusion havebeen other fac-tors associated withunfavorableprognoses.1 Demiret al.
observedthatthesizeofthetumorandtheinitialresponse totreatment,aswellasthelocationofthetumor,negatively impacted survival rate. An osseous or pulmonary origin, or a tumor located in the costovertebral union, showed decreasedsurvivalrates.5
Theimportanceofidentifyingtheseneoplasmsresidesin itsaggressive behaviorand initshigh rateof recurrence. Even though there arenumerous case reports, itsclinical course,diagnosisandtreatmentarenotveryclear. There-fore,itisofgreatimportancethatamultidisciplinaryteam isfamiliarwiththesetumors,tomakeanadequate correla-tioncorrelation withthepatient’shistory,whichwillbring ustoabetterunderstandingofitsbehaviorandestablisha treatmentwhichwillimprovetheprognosisandsurvivalof thepatient.
In conclusion, the Askin tumor should be considered withinthedifferentialdiagnosisofthoracicneoplasms.Once thediagnosisofaprimitiveneuroectodermaltumorismade, optimal treatment will consist of a multimodal manage-ment,usingneoadjuvantchemotherapyinassociationwith surgicalresectionand/or postoperativeradiotherapy,with whichadecreasedlocalrecurrenceandagreater disease-freeperiodcanbeachieved.Duetoitsaggressivebehavior, follow-upofthesepatientsshouldbeperformedunderstrict adherence.
Conflict
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.LaskarS,NairC,MallikS,etal.Prognosticfactorsandoutcome inAskin---Rosai tumor:areview of104patients.IntJRadiat Oncol.2011;79:202---7.
2.AskinFB,RosaiJ,SibleyRK,DehnerLP,McAlisterWH.Malignant smallcelltumorofthethoracopulmonaryregioninchildhood: adistinctiveclinicopathologicentityofuncertainhistogenesis. Cancer.1979;43:2438---51.
3.Ushigome S, Machinami R, Sorensen PH. Sarcoma/primitive neuroectodermaltumour.In:WorldHealthOrganization Clas-sificationofTumors.PathologyandGeneticsofTumoursofSoft TissueandBone.1sted;2002.p.298---300.
4.SabatéJM,FranquetT,ParelladaJA,MonillJM,OlivaE. Malig-nantneuroectodermaltumourofthechestwall(Askintumour): CTandMRfindingsineightpatients.ClinRadiol.1994;49:634---8.
5.DemirA,GunluogluMZ,DagogluN,etal.Surgicaltreatmentand prognosisofprimitiveneuroectodermaltumorsofthethorax.J ThoracOncol.2009;4:185---92.
6.SchuckA,AhrensS,PaulussenMK,etal.Localtherapyin local-ized Ewing tumors: results of 1058 patients treated in the CESS81CESS86,andEICESS92trials.IntJRadiatOncolBiol. 2003;55:168---77.
7.Desai S, Jambhekar N. Pathology of Ewing’s sarcoma/PNET: current opinion and emerging concepts. Indian J Orthop. 2010;44:363---8.
30caseswithimmunohistochemicalandelectron-microscopic support treated at the Institute Gustave Roussy. Cancer. 1992;69:1012---20.
9.GaudeG,PatilP,MalurP,AnnurshetruS.Casereport.
Primi-tiveneuro-ectodermaltumorofthelung.JThoracDis.2011;10,
http://dx.doi.org/10.3978/j.issn.2072-1439.2011.07.02. 10.FinkM,SalisburyJ,GishenP.Askintumor:threecasehistories
andareviewoftheliterature.EurJRadiol.1992;14:178---80.
11.ParikhM,Samujh R,Kanojia RP,MishraAK, SodhiKS,BalA. Peripheralprimitiveneuroectodermaltumorofthechestwall inchildhood:clinico--- pathologicalsignificance.Management andliteraturereview.ChangGungMedJ.2011;34:213---7.
12.GamberiG, Cocchi S,Benini S, etal. Moleculardiagnosis in Ewingfamilytumors:theRizzoliexperience---222consecutive casesinfouryears.JMolDiagn.2011;13:313---24.
13.SirivellaS, GielchinskyI.Treatmentoutcomesin23thoracic primitive neuroectodermal tumours: a retrospective study. InteractCardiovascThoracSurg.2013;17:273---9.
14.VeronesiG,SpaggiariL,DePasT,etal.Preoperative chemother-apy is essential for conservative surgery of Askin tumors. J ThoracCardiovascSurg.2003;125:428---9.