www.elsevier.es/rmuanl
ORIGINAL
ARTICLE
Prevalence
of
sensorineural
hearing
loss
in
children
and
adolescents
with
diabetes
mellitus
J.L.
Trevi˜
no-González
a,∗,
D.I.
Campuzano-Bustamante
a,
O.
Flores-Caloca
b,
R.
Santos-Lartigue
a,
M.J.
Villegas-González
Jr.
aaDepartmentofOtolaryngologyandHeadandNeckSurgeryofthe‘‘Dr.JoséEleuterioGonzález’’UniversityHospitalofthe AutonomousUniversityofNuevoLeón,Mexico
bDepartmentofEndocrino-Pediatricsofthe‘‘Dr.JoséEleuterioGonzález’’UniversityHospitaloftheAutonomousUniversityof NuevoLeón,Mexico
Received23June2015;accepted23June2015 Availableonline17August2015
KEYWORDS Diabetesmellitus typeI;
Insulin-dependent diabetes;
Sensorineuralhearing loss;
Deafness; Children
Abstract
Objective: Toestablish the prevalenceofsensorineural hearing loss(SNHL), aswell asthe predisposing riskfactors, inchildren and adolescentswith type 1diabetes mellitus(T1DM) attendingtheServiceofEndocrino-PediatricsandOtolaryngologyDepartmentofthe‘‘Dr.José EleuterioGonzález’’UniversityHospitalandtheMaterno-InfantilHospital,fromJanuary2011 toDecember2012.
Materialandmethods: Atotalof84childrenwithT1DM,withagesbetween6and18yearsold, werestudied.Valuesofglycatedhemoglobin(HbA1c)wereassessedandTonalaudiometryand Speechaudiometrytestswereperformed.
Results:Atotalof84patientswithadiagnosisofT1DMwerestudied,outofwhich12(14.3%) presentedSNHL.Fiftypercentofpatientswith hearinglosswereintheagerangeof10---13 yearsold.Regardingtimeofevolutionwiththedisease(T1DM),33%ofpatientswithmorethan 5yearswithT1DMpresentedSNHL,andnearly88.9% ofthepatients withlessthan5years withT1DMpresentednormalhearing(p=0.011).Moreover,65.47%ofthepatientspresented complicationsduetopoorglycemiccontrolatsomepointintheevolutionoftheirdisease.All (100%)diabetic patientswithSNHLand91%ofthepatientswithoutSNHLhadHbA1cvalues greaterthan6%.Inpatientswithhearingimpairments,83.3%sufferedmildand16.4%suffered moderatehearingloss.Mostpresentedbilateral hearingloss,withtherighteardominating. Acutefrequencies,mainly8000kHz,werethemostaffected.
∗Correspondingauthorat:ServiciodeOtorrinolaringologíadelHospitalUniversitario‘‘Dr.JoséEleuterioGonzález’’delaUniversidad AutónomadeNuevoLeón,Ave.MaderoyGonzalitoss/nColoniaMitrasCentro,C.P.64460,Monterrey,N.L.,Mexico.Tel.:+528183334299; fax:+528183332917.
E-mailaddress:[email protected](J.L.Trevi˜no-González). http://dx.doi.org/10.1016/j.rmu.2015.06.004
:Conclusion:SNHLprevalenceamongourdiabeticpopulationwas14.3%,whichindicatesthata sixthofourdiabetictype1populationwilldevelopSNHL.Accordingtotheresultsobtained, SNHLismorefrequentamongpatientswhohavehadT1DMformorethan5years.Nevertheless, morestudiesarerequiredtoconfirmthatthereisarelationbetweentimespentwiththedisease andSNHL.
©2015UniversidadAutónomadeNuevoLeón.PublishedbyMassonDoymaMéxicoS.A.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
The World Health Organization (WHO) defines diabetes mellitus (DM) as a multiple-etiology metabolic disorder, characterizedbychronichyperglycemiaandothermetabolic abnormalities, which resultin absolute or relativeinsulin deficiency.Itisthemostfrequentendocrine-metabolic dis-orderin children and adolescents, and has remained the maintypeofdiabetesinchildren.1---4
Type1diabetesmellitus(T1DM)isadiseasewithan eti-ologyof intervening environmental factorswhich interact withagenetic-predispositioncomponent;itisconsidereda chronicautoimmune diseasewhich causesthe destruction ofthepancreaticcellswhichproduceinsulin.5
Theaverageageoftheonsetofthediseaseisbetween7 and 15 yearsof age; however, it may occur at any age.6
Values of the HbA1c>6% higher than the normal range (5---6%)havebeenconsideredariskofdevelopingmicro-and macroangiopaticcomplications.Theaffectionoftheblood vesselswhichsupplytheinnerearandthevascularstriahave beenreportedbydifferentauthorsasaphysiopathological causeofSNHLinT1DMpatients.3,7Treatmentwithinsulin,
maintainingonaverage HbA1cof 7.2%, reducesthe onset andprogressionofmicroangiopaticcomplications,atrophy, anddemyelinationofthespiralganglionbyupto76%.8,9,13
Sensorineuralhearingloss(SNHL)isalossofhearingat anyfrequency morethan 25dB, withconductiveand sen-sorineuralgapslowerthat20dB,andaffectingthepatient’s abilitytocommunicate,hisorhereducation,jobprospects andsocialrelationships,andalsocausesstigmatization.11,12
ThereportedprevalenceofSNHLisupto33%inchildren withT1DMversus 0.3---0.5% in healthychildren. In Mexico thereisalackofsufficientepidemiologicinformationwhich definesthehearingconditionprevailinginourpopulation.12
Materials
and
methods
Aprospectivelongitudinal,analytic,comparativestudywas conducted on a total of 87 patients of both sexes, ages 6---18,withaT1DMdiagnosis,fromtheServiceof Endocrino-PediatricsandOtolaryngologyDepartmentofthe‘‘Dr.José EleuterioGonzález’’University Hospital and the Materno-InfantilHospital,fromJanuary2011toDecember2012.
We included patients whoagreed toparticipatein the protocolthroughasignedinformedconsent,signedbytheir parentsand/orguardiansand/orthepatient.Weexcluded patientswithnoiseexposure,afamilyhistoryofdeafness, use of ototoxic medications, otitis media, a history of
previousearsurgery(exceptventilationtubeinsertion)and DMtype2.
All subjects in this study were given a questionnaire, whichincludedfamily,prenatal,natalandpersonal patho-logical and non-pathological history. Patients underwent basic otorhinolaryngological exploration, tone audiometry andoralaudiometryusinganaudiometerAUDIOTEST259b, manufactured for Interacustics, Type 2 Tone Audiometer, TypeB-E-Tspeechaudiometerinasoundproofcabin Acous-tics Systems,ModelRE-142, Serial#21413a, madein USA. ThestudywasapprovedbytheEthicsandResearch Commit-teeoftheSchoolofMedicineoftheUniversidadAutónoma deNuevoLeón(UANLbyitsSpanishacronym)withthe reg-istrationkeyOT12-002.
The information obtained was gathered in a database usingExcel,performingstatisticalanalysisusingSPSS20.0. We obtained the traditional statistics in the quantitative and qualitative variables, looking to establish differences betweenbothgroupsthroughhypothesistestsformeansand proportions,toestablishtheabsenceorpresenceof associa-tionandcorrelationusingchisquare,PearsonorSpearman, withaconfidenceandreliabilityof95%.
Results
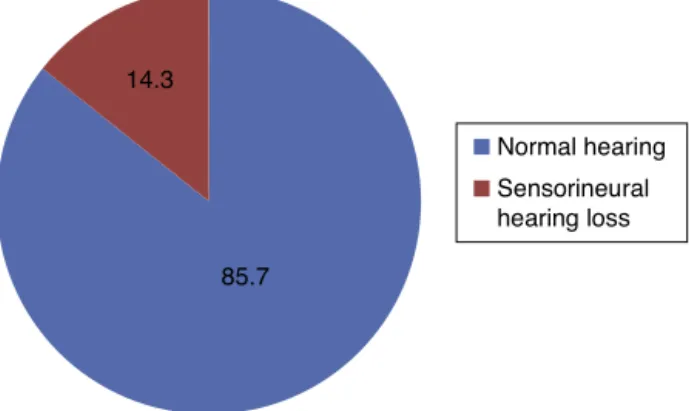
Outofthe87recruitedpatientswithaT1DMdiagnosis,we excludedapatientwithahistoryofchronicotitismediaof theright ear,onewithotitismediawithbilateraleffusion andapatientwithafinaldiagnosisofT2DM.Theremaining 84patientsweredividedinto3groups basedonage:6---9, 10---13,and14---18yearsold.Weobservedthat72patients withaT1DMdiagnosisshowednormalhearingwhile12T1DM patientsshowedsensorineuralhearingloss(Fig.1).
85.7 14.3
Normal hearing
Sensorineural hearing loss
8.30% 50.00% 41.20% 26.40% 36.00% 37.50%
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 6 to 9 years
10 to 13 years 14 to 18 years
T1DM + normal hearing T1DM + SNH
T1DM = siabetes sellitus type 1; SNH = sensorineural hearing loss
Figure2 Comparisonofbothgroupsbyagerange.
The6---9groupincluded20patients(9girlsand11boys) withdiabeteswithanevolutiontimeoflessthan5years;10 (50%)subjectspresentedahistoryofpreviouscomplications likeketoacidosis,hyperglycemia or hypoglycemia,2 (10%) patients had HbA1c<6 and 18 HbA1c>6, and 1 (5%) sub-jectpresentedmildSNHLfor8000kHzthresholds.The10---13 groupincludedatotalof30patients(13girlsand17boys); 29(34.5%)hadhaddiabetesmellitusforlessthan5yearsand 1(1.21%)forover5years,18(21.4%)patientspresenteda historyofketoacidosis,hypo-orhyperglycemia,29(34.52%) presentedHbA1c>6and1(1.19%)HbA1c<6;mildSNHLwas displayedin 3 (3.57%) subjectsand 1 (1.19%)patient dis-playedmoderateSNHL,andall4patientswerein hearing thresholds of 8000kHz. The 14---18 group consisted of 34 patients (40.47%)(20 girls and14 boys),22(64.70%) with anevolution timeof lessthan5yearsand12(35.29%)for more than5 years;complications like ketoacidosis, hypo-or hyperglycemia werereportedby 27of them;3 (8.82%) subjectsshowedanHbA1c<6and31(91.17%)anHbA1c>6; SNHLoccurredwithinthisgroupin7individuals(mildin 6 andmoderatein 1).Inallpatients, SNHLwasobservedin thresholdsof8000kHz(SeeTable1).
Inourstudy,wewereabletoobserveapercentage preva-lence of SNHL of 14.3% (12 out of 84 patients). Also, 64 patients (76.19%) withT1DM were older than 10 yearsof age, asopposed toa small group of 20 patients (23.80%) betweentheagesof6and9(Fig.2).Therewereno differ-encesingender,eachrepresenting50%.Inregardtotimeof evolutionof T1DM,15.47% (13patients)withover 5years withT1DMpresented SNHL,and84.52% (71patients)with lessthan5yearswithT1DMpresentednormalhearing,this beingastatisticallysignificantvalue(p=0.011)(Fig.3).
66.70%
88.90%
33.30% 11.10%
0.00% 20.00% 40.00% 60.00% 80.00% 100.00% T1DM + SNH
T1DM + normal hearing
T1DM = diabetes mellitus type 1; SNH = sensorineural hearing loss More than 5 years with T1DM 5 years or less with T1DM
Figure3 ComparisonofbothgroupsbyT1DMevolutiontime. T
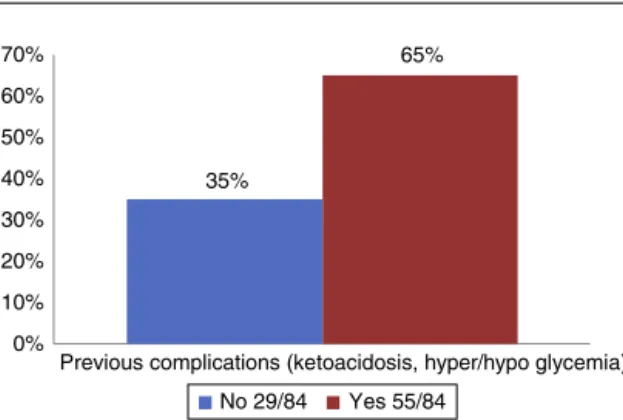
35%
65%
0% 10% 20% 30% 40% 50% 60% 70%
Previous complications (ketoacidosis, hyper/hypo glycemia)
N = 84 patients; hypoglycemia: glycemia < 60 mg/dL; hyperglycemia: glycemia 126-250 mg/dL; ketoacidosis: glycemia > 250 mg/dL + ketonemia and ketonuria.
No 29/84 Yes 55/84
Figure4 Previouscomplicationsfromuncontrolledblood glu-coseinbothgroups.
83.30% 16.70%
0% 0%
0.00% 20.00% 40.00% 60.00% 80.00% 100.00% Light 20 to 40 DB
Moderate 41 to 60 DB Severe 61 to 80 DB Profound more than 80 DB
T1DM = diabetes mellitus type 1; SNH = sensorineural hearing loss T1DM + SNH
Figure5 Degreesofsensorineuralhearingloss.
Out of the 84 patients, 55 (64.47%) presented complicationsat somepoint during the evolutionof their disease due to glycemic irregularities;the most frequent complicationwasketoacidosisandtheleastprevalentwas hypoglycemia(Fig.4).
Inthepresentstudy,100%ofdiabeticpatientswithSNHL (12patients)and91%ofpatientswithnormalhearing pre-sentedHbA1cvaluesgreater than6%,showingan average value of 7.5% in the general population studied. Accord-ingtoagegroups,thegroupconsistingofchildrenbetween 6and 12yearspresented, onaverage, an HbA1cvalue of 7.24%,while thegroup consisting of children between 13 and19yearsofagepresented,onaverage,anHbA1cvalue of7.67%.
OfalltheSNHLpatients,83.30%(10patients)presented mild hearingloss and 16.70% (2 patients)moderate hear-ingloss(Fig.5).Mostpatients presentedbilateralhearing loss,predominatelyontherightear.The8000kHzthresholds werethemostaffected.(Table1)
Discussion
An SNHL prevalence of up to 33% in children with T1DM hasbeen considered,versus 0.3---0.5%in healthychildren. InMexico,thereisalackofepidemiologicinformationthat candefinethehearingconditionwhichprevailsamongour population.12
Theobservedprevalenceinourstudiedgroupwas14.3%, contrary to the rate reported in different publications.
However,we must keep inmind thatmost of the studied populationisAmericanorEuropean.Itisimportanttostress the fact that there are still many T1DM cases that have not been diagnosed,but withthe obtainedresults at this point,weareabletoinferthatuptoasixthofthediabetic populationinoursocietywilldevelopSNHL.
Regardingage,theobtainedinformationmatchestheone foundinthebibliography.Mostchildrenareinthementioned peak ranges, especially above 10 yearsof age, beginning withhormonechangesthatareanormalpartofpubertyand adolescence. Nevertheless, basedon the obtained results weareabletoseethatthepatient’sagedoesnotrepresent ariskfactorforthepresenceofSNHL.
According to the American Diabetes Association (ADA) andtheDiabetesmedicalattentionstandardsof2014,the goal for HbA1cin type1 diabetic patientsvaries depend-ingonage.Concerningvalues<8%inthe6---12years-of-age range,becauseitisnotpossibletohavemorestrictgoals due tothe risk of developing hypoglycemia, evenin this age rangewe candemandgoals of <7.5%inspecific cases wherepatientsdonotpresentseverehypoglycemia.Inthe 13---19 years-of-age range,valuesof <7.5% areconsidered andinspecificcaseseven<7%.Inchildrenunder6yearsof age,goals of <8%aretoostrict,soupto<8.5% is accept-able, becausethese children have a greater vulnerability for hypoglycemia, agreater sensitivitytoinsulin, andare unpredictableintheirintakeandphysicalactivity.10
TheaveragepopulationshowedHbA1cvaluesof7.5%and takingtheresultsbyagegroupintoaccount,weareableto saythatourpatients,under13yearsofagewithanHbA1c averageof7.24%,arewithinanadequateglycemiccontrol, becausetheyareinsidetheacceptedrangebytheADA2014 (6---12years=<8%);andpatientsolderthan13yearsofage withanaverageof7.67%showacontrolbarelyabovethat expectedfortheiragegroup(13---19years=<7.5%).
It is important to maintain HbA1c values as close to normal as possible, thus reducing by almost 80% the risk of presentingmicroangiopatic complications;however,we mustnotbeverystrictwithourpopulation,especiallywith childrenunder13yearsofage,becauseoftherisksof pre-senting severe or belatedhypoglycemia cases, and hence the importance of following the standards established by theADA2014.
RegardingtimeofevolutionwithT1DM,itwastheonly statistically significant risk factor (p=0.011) for a period greaterthan5yearsandthepresenceofhearingloss. How-ever, when we looked for the correlation between both factors, we did not find it. The present study showed a greater prevalence of hearing loss in patients with more than 5 yearsof evolutionof T1DM, without itbeing asso-ciatedorrelated.Thiscouldbeduetothelackofpotency in thestudied population whopresented T1DMandSNHL, requiringagreaternumberofpatientsandfurtherresearch. Nevertheless,itisimportantthat5yearsafteraT1DM diag-nosis,asthereisanalreadyestablishedprotocolinsearchof microangiopatic complicationslike retinopathy, we estab-lish the application of hearing studies which allow us to detecthearingproblemsinatimelymanner.
in these patients is similarto the one that patients with presbycusiswouldpresent,butatanearlieragecompared tothepopulationwithoutT1DM.
This research provided valuable data to lead the way for newresearches in thesetypes of patients, and estab-lishatimelyandprotocol-ledassessmentfortheirglycemic control as well as their hearing, thus avoiding hearing complicationswhichpatientswithaT1DMoflongduration present,likeSNHLandsuddenhearingloss.Also,later stud-iesarerecommendedwherealong-termfollow-upisgiven tothesepatientsinordertodeterminethecausationdegree ofthestudiedriskfactorsonthebasepathology.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Funding
Nofinancialsupportwasprovided.
References
1.Australian.Clinicalpracticeguidelines:type1diabetesin chil-drenandadolescents,Australia,vol.1;2005.p.26.
2.TakeshiK.Earlydiagnosis,earlytreatmentandthenew diag-nosticcriteriaofdiabetesmellitus. BrJNutr.2000;84Suppl. 2:S177---81.
3.LisowskaG,NamysłowskiG,MorawskiK,StrojekK.Early identi-ficationofhearingimpairmentinpatientswithtype1diabetes mellitus.OtolNeurotol.2001;22:316---20.
4.KuzuyaT,NakagawaS,SatohJ,etal.ReportoftheCommittee ontheclassificationanddiagnosticcriteriaofdiabetesmellitus. DiabetesResClinPract.2002;55:65---85.
5.SteeleC,HagopianWA,GitelmanS,etal.Insulinsecretionin type1diabetes.Diabetes.2004;53:426---33.
6.Mark AS, Stuart AW, William VT. Diabetic mellitus. Pediatric endocrinology, vol. 10, 3rd ed. Saunders Elsevier; 2008. p. 374---7.
7.Pi˜nónPAL,LuisREJ.ValordiagnósticodelaHemoglobina Glu-cosiladaenelestadoprediabético.HospitalUniversitarioCdte. FaustinaPérezHernández;2008.
8.LachinS,GenuthS,NathanDM,ZinmanB,RutledgeBN.Effectof glycemicexposureontheriskofmicrovascularcomplications inthediabetescontrolandcomplicationstrial-revisited. Dia-betes.2008;57:995---1001.
9.DCCT(TheDiabetesControlandComplicationsTrialResearch Group). The effect of intensive treatment of diabetes on thedevelopmentand progressionoflong-termcomplications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14).Massachusetts.
10.ADA---AmericanDiabetesAssociation.Standardsofmedicalcare indiabetes2014.DiabetesCare.2014;37Suppl.1.
11.ElaminA,FadlallahM,TuvemoT.Hearinglossinchildrenwith type1diabetes.IndianPediatr.2004;42:15---21.
12.Secretaria de Salud Guía de Práctica Clínica. Evidencias y recomendaciones. Hipoacusia Neurosensorial Bilateral e ImplanteCoclear.México,D.F.;2010.