www.elsevier.com.mx
medicina
universitaria
* Corresponding author: Department of Gynecology and Obstetrics, “Dr. José Eleuterio González” University Hospital. Madero y Gonzalitos Avenue, Mitras Centro, Monterrey, N. L., México. E-mail address: [email protected] (J. L. Iglesias-Benavides).
OrIGINAL ArtICLE
Maternal mortality and severe obstetric morbidity in a tertiary
care hospital
J. L. Iglesias-Benavides
*, M. S. Vidales-Hernández, W. E. Treviño-Ledezma, S. N.
Delgado-Muñiz, A. Guzmán-López, O. L. Guzmán-Aguillón
Department of Gynecology and Obstetrics, “Dr. José Eleuterio González” University Hospital, Universidad Autónoma de Nuevo León, Monterrey, N. L., Mexico
received: October 2013; Accepted: October 2013
KEYWORDS Maternal death; Severe obstetric morbidity; Incidence; Mexico.
Abstract
Introduction: Maternal mortality (MM) is a relection of the quality of care given to pregnant women. However, it does not relect many illnesses and medical complications of women at risk
of death, who do not die. Severe obstetric morbidity (SOM) refers to women who are “pregnant or recently postpartum, very ill, who would have died if not for the good health care received”.
Objective: to review the incidence of MM and SOM at the Obstetric Service of the University Hospital, Universidad Autónoma de Nuevo León (UANL) in the years 2007-2011.
Material and methods: Observational, cross-sectional, retrospective study, at the Obstetric Ser-vice of the University Hospital, UANL.
Results: We attended 19,985 births; there were 37 maternal deaths: 14 due to hypertensive disorders (37.8%), 3 due to hemorrhage (8.1%), 13 (35.1%) due to medical complications, 1 (2.7%) due to an anesthetic problem, and 6 due to sepsis (16.2%). twenty-three (62.1%) mater-nal deaths were catalogued as direct and 14 (37.8%) as indirect. Of 407 cases of SOM, 310 (76.1%) were due to hypertensive disorders, 58 (14.2%) to obstetric hemorrhage, 26 (6.3%) to medical complications, 1 (0.2%) to anesthetic complication, and 12 (2.9%) to sepsis. the MM rate was 1.85 per 1,000 live births; the incidence of MOS was 81.4 per year, with 1 death per every 11 cases.
Conclusions: the MM and the SOM provide more reliable data on the prevalence of serious
com-plications in obstetrics. This allows us to take preventive measures, offer better medical care,
and improve the allocation of resources.
Introduction
Maternal mortality (MM) is an occurrence which relects the quality of the healthcare system. The World Health Organi -zation defines maternal death as “the death of a woman while pregnant or within 42 days of termination of pregnan-cy, from any cause related to or aggravated by the preg-nancy or its management but not from accidental or in- cidental causes”. Direct maternal death is the result of a complication of the pregnancy, delivery or management of the 2 while an indirect maternal death (IMD) is a pregnancy-related death in a patient with a preexisting or newly deve-loped health problem unrelated to pregnancy. the standard
indicator is the MM rate which is deined as the relationship
between the numbers of maternal deaths for every 1,000 births.1
Severe obstetric morbidity (SOM) refers to “a pregnant or postpartum patient, very ill, who if not treated appropria-tely, would result in death”.2 It is safe to assume that the same disease processes which cause SOM are closely related to the ones which cause MM. It is possible to study the cir-cumstances surrounding women with SOM, therefore we are able to implement a better surveillance on maternal care.3
In medical literature, different inclusion criteria are used in the selection of SOM cases such as acute organ system dysfunction,4 severe obstetric complications between the 28th week of gestation and 42 days of puerperium,5 admis-sions to the intensive care unit,6,7 patients receiving a blood transfusion,8 and anesthetic accidents.9
the MM rate and other indexes have been created as a result of the study of such data. these indexes provide a be-tter understanding of the medical problems surrounding pregnant women. Mortality rate represents the number of deaths in accordance to the number of SOM cases, morbidi-ty rate expresses the relationship between SOM cases for every maternal death, and SOM incidence indicates the number of very ill women who are attended per year.10-13 the objective of this study was to review the main causes and incidence of maternal death, as well as SOM at the “Dr. José Eleuterio González” University Hospital of the Univer-sidad Autónoma de Nuevo León (UANL), between 2007 and 2011. Another objective was the analysis of medical and so-cial factors related to the care and attention of obstetric complications and maternal deaths.
Material and methods
In this retrospective, transversal, analytic study, iles of pa
-tients classiied as maternal death, and those who met the
criteria for SOM between January 2007 and December 2011 were reviewed.
According to the literature, we considered as SOM preg-nant women with severe preeclampsia, eclampsia and HELLP syndrome (a life-threatening pregnancy complication usually considered to be a variant of preeclampsia, named after its characteristics: hemolysis, elevated liver enzymes, and low platelet count); women who had hemorrhage befo-re, during or after delivery higher than 500 ml and who
required a blood transfusion; severe medical diseases com -plicating pregnancy (cardiomyopathy, nephropathy, AIDS, thrombocytopenic purpura, etc.); women admitted to the
intensive care unit who underwent an obstetric
hysterec-tomy, laparotomy or pelvic packing, as well as anesthetic
accidents and puerperal sepsis cases.4-9
In order to obtain a better data analysis of MM and SOM, we divided the patients into 5 groups: hypertensive disor-ders, obstetric hemorrhage, medical conditions, anesthetic accidents, and sepsis.
the studied variables were: discharge diagnosis, number of surgeries practiced, blood transfusions, age, schooling, marital status, prenatal care (5 visits or more), gestational age, days of overnight stay, admittance to the Neonatal In-tensive Care Unit (NICU -UCIN in its Spanish acronym) and newborn conditions (NB). We calculated the MM rate (num-ber of maternal deaths over the num(num-ber of live births and stillbirths per 1,000),10 the mortality rate (maternal deaths over the number of SOM cases times 100)11,12 morbidity rate (number of SOM cases divided by the number of maternal deaths) and SOM incidence (number of SOM cases over the sum of periods of time).13,14 We performed descriptive
sta-tistics of frequency.
Results
During the 5-year reviewed, 19,985 births took place and
37 maternal deaths were registered (0.18%). the causes of death were as follows: 14 corresponded to hypertensive disorders (37.8%), 3 to hemorrhage (8.1%), 13 to medi- cal complications (35.1%), 1 to an anesthetic problem (2.7%), and 6 to sepsis (16.2%) (table 1). In 23 of the cases
(62.1%), maternal death was classiied as direct and in 14
(37.8%) as indirect. Maternal death rate was 1.85 per 1,000 born alive and dead. We gathered 407 SOM cases: 310 (76.1%) hypertensive disorders, 58 (14.2%) with an obstetric hemorrhage, medical complications in 26 (6.3%), 1 case (0.2%) with anesthetic complications, and 12 (2.9%) with sepsis (table 2). Mortality rate was 9.09% and morbi-dity rate resulted in 1 death for every 11 SOM cases (table 3).SOM incidence was 81.4 cases per year. After measu-ring mortality and morbidity rates within each of the SOM pathology groups, we found that for hypertensive disor-ders, morbidity rate resulted in 1 death for every 22.1 cases and mortality was 4.5%; in the hemorrhage cases, morbidity rate resulted in 1 death for every 19.3 and mor-tality was 5.1%; regarding medical complications and sep-sis, morbidity rate resulted in 1 death for every 2 and mortality was 50%; for anesthetic complications, morbidi-ty rate was a single case which resulted in death with a mortality rate of 100% (table 4).
Sixty patients underwent hysterectomy (14.7%) and 56 i
-les were reviewed. Background of a previous C-section oc -curred in 34 cases (60.7%). the diagnosis corresponded to placenta accrete in 30 cases (53.5%), uterine atony in 12 (21.4%), cornual and cervical ectopic pregnancy in 3 (5.35%), uterine myomatosis in 3 (5.35%), uterine perfora-tion in 3 (5.35%), and 3 (5.35%) cases with sepsis. In 2 patients a carcinoma in situ diagnosiswas established. In
Admittance to the NICU occurred in 132 cases (32%) as fo-llows: 80 due to hypertensive disorders (19.6%), 20 due to hemorrhage (4.9%), 24 due to a medical condition (5.8%) and 8 due to sepsis (1.96). Hospital stay ranged from 5 to 90 days, with an average of 10 days.
Maternal age was analyzed in 368 cases and ranged from 14
to 42 years, with an average of 25.3. The most frequent age
group was under 20 years with 128 cases (34.7%), followed by 21 to 25 years with 81 (22%). As for marital status, the distri-bution of the 327 cases was as follows: 195 single or in com-mon-law marriage (59.6%) and 132 married (40.3%). Schooling for the 327 cases was: 56 with elementary school completed
(17.1%), 193 with junior high school completed (59.02%), and 78 with high school or higher education completed (23.8%)
(Table 5). Distribution by gestational age in weeks at the mo -ment of admission was, out of the 327 SOM patients: of 43
cases with 25-30 weeks of age; 93 cases between 31-35 wee
-ks (28.44%); 181 between 36-40 wee-ks (55.35%), and 10 cases with 41 weeks or more (3.05%). Prenatal care in 327 iles was
considered positive in 233 cases (71.2%) and negative in 94 (28.7%). Obstetric care in 354 reviewed cases was of 3 uteri-ne curettage (0.84%), 38 deliveries (10.73%) and 313 C-sec-tions (88.41%).
Table 1 Causes of maternal deaths from 2007 to 2011.
Maternal death causes 2007 2008 2009 2010 2011 total %
Hypertensive disorders 2 2 4 0 6 14 37.8
Obstetric hemorrhage 2 0 1 0 0 3 8.1
Medical condition 3 1 5 3 1 13 35.1
Anesthetic complication 0 1 0 0 0 1 2.7
Sepsis 2 1 3 0 0 6 16.2
total 9 5 13 3 7 37 99.9
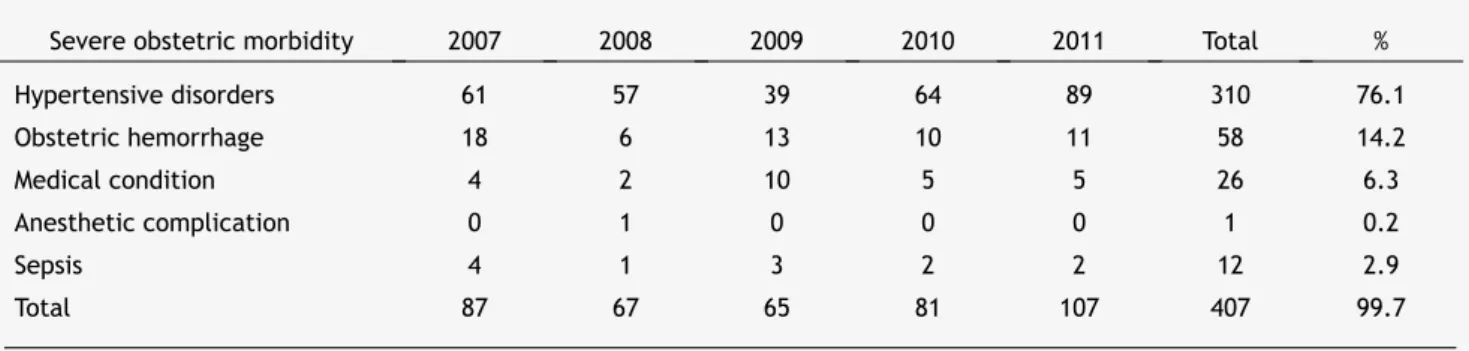
Table 2 Number of cases of severe obstetric morbidity from 2007 to 2011.
Severe obstetric morbidity 2007 2008 2009 2010 2011 total %
Hypertensive disorders 61 57 39 64 89 310 76.1
Obstetric hemorrhage 18 6 13 10 11 58 14.2
Medical condition 4 2 10 5 5 26 6.3
Anesthetic complication 0 1 0 0 0 1 0.2
Sepsis 4 1 3 2 2 12 2.9
total 87 67 65 81 107 407 99.7
Table 3 relation between number of births, morbidity, severe obstetric morbidity (SOM), maternal deaths and associated data of the period 2007-2011.
Year Births SOM Maternal deaths
Mortality rate (1,000
newborns) Morbidity rate Mortality index (%)
2007 3,890 87 9 2.31 9.6 10.3
2008 3,915 67 5 1.27 13.4 7.4
2009 3,718 65 13 3.49 5 20
2010 4,074 81 3 0.73 27 3.7
2011 4,388 107 7 1.59 14.5 6.8
Discussion
Maternal mortality is the result of a series of events which
reveal a lack of action to improve the conditions and the
exclusion conditions which many women in Mexico live in. Behind every maternal death there is a series of severe so-cioeconomic problems such as a high child morbidity/mor-tality rate, malnutrition, orphanage, schooling drop-outs,
and a premature start for children in the workforce.15 MM is
a relection of the quality of care given to pregnant women. However, this parameter does not show the frequency of
many of the pathologies of women who were close to dying
but survived. The undeniable benefits of this knowledge allow us to know what is really happening in the obstetric
units, while MM provides us with limited information. Around 1% of pregnant women suffer some sort of event
which puts their lives at risk and there is an estimate of 120
events for every direct MM, most of which are related to Table 4 relation between severe obstetric morbidity, maternal deaths, mortality rate and morbidity rate for each group.
Severe obstetric morbidity N Maternal deaths (n) Morbidity rate Mortality rate (%)
Hypertensive disorders 310 14 22.1 4.5
Obstetric hemorrhage 58 3 19.3 5.1
Medical condition 26 13 2 50
Anesthetic complications 1 1 1 100
Sepsis 12 6 2 50
total 407 37 11 9.09
Table 5 Maternal age, marital status and level of education frequencies in severe obstetric morbidity patients between 2007 and 2011.
Maternal age 2007 2008 2009 2010 2011 total (%)
< 15 4 0 2 4 6 16 4.3
16-20 16 27 14 33 38 128 34.7
21-25 22 11 11 14 23 81 22
26-30 12 5 9 8 11 45 12.2
31-35 17 14 10 10 13 64 17.3
36-40 7 4 4 6 7 28 7.6
> 40 2 1 1 1 1 6 1.6
total 68 62 51 76 99 368 99.7
Marital status
Married 29 28 16 28 31 132 40.3
Single/ common-law
marriage
43 28 30 34 60 195 59.6
total 72 56 46 62 91 327 99.9
Level of education
Elementary 12 10 10 10 14 56 17.1
Junior high
school 45 34 20 40 54 193 59.02
High school or higher
15 12 16 12 23 78 23.8
hypertension and hemorrhage. Severe maternal morbidity is
quantiiable and can be the best way of measuring the im -provements in health care.15,16
In Mexico, 90% of maternal deaths occur in hospitals or medical units. this is why the hospital MM rate is so high, compared to the general population.17 In Nuevo Leon for this period of time, the average MM rate was 9.9 per 100,000 born alive. When we compare our MM rate of 1.85 per 1,000 births with that from other hospitals, it is below the 2.46 and 2.48% reported by the Hospital Materno Perinatal del Estado de México during 2007 and 200818 and by Peru (11.25 per 1,000 births).19 A common problem in concentration hos-pitals is the admittance of severe maternal complications, which are referred very tardily. In our MM group we found that 25 patients (67.5%), were referred in a bad condition. the relation is as follows: of the hypertensive disorders, 12 out of the 14 fatal cases (85.7%) were referred to our hospi-tal with brain hemorrhage; the 3 fahospi-tal cases resulting from hemorrhage were treated in other hospitals and then sent here; of the 6 fatal cases due to sepsis, 5 (83.3%) were treated in other hospitals and then sent here; of the 13 fatal cases from medical complications, 5 (19.2%) were admitted to our department being very ill.
the pattern of the main obstetric causes of morbidity and mortality has remained unchanged in the last decades;
however, the frequency of all the causes have risen. The 5
main causes worldwide are complications of abortion, pos-tpartum hemorrhage, high blood pressure, antepartum he-morrhage and pre-existing medical conditions.20,21 the 407 SOM cases represent 2.03% of total births, i.e., 1 SOM case for every 49 births. Obstetric morbidity and MM have a di-rect or close relationship. In our review, there were 37 ma-ternal deaths and the 3 main reasons were: Hypertensive disorders (37.8%), medical conditions (35.1%), and sepsis (16.2%). In the same period of time, SOM incidence was as follows: hypertensive disorders (76.1%, hemorrhage 14.2%, and medical conditions 6.3%). there was only one differen-ce in the hemorrhage cases: they occupied the second pladifferen-ce in obstetric morbidity, while they appear in 4th place as a cause of maternal death with only 3 cases (table 1).
When we applied the rates to all of the 5 groups of SOM cases, a greater relationship with the severity of the illness comparative with the number of cases (table 4) was seen. therefore, among hypertensive diseases there was 1 death for every 22 cases (4.5%) with hemorrhage, 1 for every 19.3 cases (5.1%) with medical complications and 1 death for every 2 cases of sepsis (50%); there was also only 1 anesthe-tic complication which resulted in death (100%). these results were positively correlated with the admittances to NICU: 19.6% from hypertensive disorders, 4.9% hemorrhage, 92.3% medical conditions, and 66.6% sepsis.
the age group with the highest number of SOM were tee-nagers with almost 35%; 60% were single or in common-law
marriage. Eighty-two percent had inished junior high school
or higher (table 5). Becoming pregnant at an early age
marks the beginning of long-term economic and social res -ponsibilities, as most of these mothers have low income and
limited work options, favoring a vicious cycle of poverty.
this situation worsens with the inter-generational
repeti-tion of teenage pregnancy, increasing the risk of
compli-cations.22,23Being single or living in common-law marriage favors social exclusion and reduces economic expectations
as well as medical care for women.24 In our study all of the patients were low income and did not have medical care services.
Obstetric care in 354 reviewed cases was of 3 uterine cu-rettages (0.84%), 38 deliveries (10.73%) and 313 C-sections (88.41%). Historically, performing C-sections is related with obstetric complications or associated with medical condi-tions.25
Conclusion
Assessment of MM in addition to SOM provides reliable data about the prevalence of severe obstetric complications;
thus, this relevant information allows taking speciic pre -ventive measures as well as improving medical care and the allocation of resources addressed at caring for women of childbearing-age.26
Conlicts of interest
The authors have no conlicts of interest to declare.
Funding
No inancial support was provided.
References
1. Clasiicación estadística internacional de enfermedades y pro
-blemas relacionados con la salud. Décima revisión. Publicación cientíica 554. Organización Mundial de la Salud 1992;2:29-64.
2. Say L, Pattinson rC, Gulmezoglu AM. WHO systematic review of maternal morbidity and mortality: the prevalence of severe acute maternal morbidity (near miss). reprod Health 2004;1:3– 7.
3. Pattinson RC, Buchmann E, Mantel G, et al. Can enquiries into
severe maternal morbidity act as a surrogate for maternal
death enquiries? Br J Obstet Gynaecol 2003;110:889–893.
4. Mantel GD, Buchmann E, rees H, et al. Severe acute maternal morbidity: A pilot study for a near miss. Br J Obstet Gynaecol 1998;105:985-990.
5. Prual A, Bouvier-Colle MH, de Bernis L, et al. Severe maternal morbidity from direct obstetric causes in West Africa: Incidence and case fatality rates. Bull World Health Organ 2000;78:593-602.
6. Fitzpatrick C, Halligan A, McKenna P, et al. Near-miss maternal
mortality (Letter). Irish Med J 1992;85:37.
7. Baskett TF, Sternadel J. Maternal intensive care and near miss
mortality in obstetrics. Br J Obstet Gynaecol 1998;105:981-984. 8. de Bernis L, Dumont A, Bouillin D, et al. Maternal morbidity and
mortality in two different populations of Senegal: A prospective study (MOMA Survey). BJOG 2000;107:68-74.
9. Mantel GD, Buchmann E, rees H, et al. Severe acute maternal morbidity: A pilot study for a near miss. Br J Obstet Gynaecol 1998;105:985-990.
10. Cabero Ll, Cerqueira Ma J. Protocolos de medicina materno-fe
-tal (perinatología). 2da Ed. Barcelona: Ed. Ergon; 2000. p. 372.
11. Pattinson rC, Hall MH. Near misses: a useful adjunct to
mater-nal death enquiries. Br Med Bul 2003;67:231-243.
13. Fabre E, Carrera José M, Monleón J, et al. Cómo diseñar, reali
-zar y comunicar la investigación clínica en perinatología. Dep
-to. Obstetricia y Ginecología Instituto Universitario Dexeus.
Barcelona: Ed. Masson; 1998. p. 199-200.
14. Castañeda M. La mortalidad materna en México. Cuatro visio
-nes críticas. Xochimilco, México: Fundar-UAM; 2004. p. 18.
15. Waterstone M, Bewley S, Wolfe Ch. Incidence and predictors of severe morbidity: case control study. BMJ 2001;322:1089-1093. 16. Danel I, Berg C, Johnson Ch, et al. Magnitude of maternal
mor-bidity during labor and delivery: United States, 1993-1997. Am J Public Health 2003;93:631-634.
17. Instituto Nacional de Estadística y Geografía. Estadísticas de
defunciones, 2010. Base de datos. México: INEGI; 2011. 18. Briones JC, Díaz de León M, Meneses J. Estrategias para reducir
la mortalidad materna hospitalaria en el Estado de México. rev Asoc Mex Med Crit y ter Int 2009;23:16-24.
19. Díaz J, Salvador JL, Hidalgo F. Mortalidad materna. Experiencia de 4 años en el Hospital Nacional Cayetano Heredia. Ginecol
Obstet 2004;50:97-100.
20. Pattinson RC, MacDonald AP, Backer F, et al. Effect of audit on
critically ill pregnant women. Clin Govern Int J 2006;11:278-288.
21. Brace V, Penney G, Hall M. Quantifying severe maternal morbi-dity: a Scottish Population Study. BJOG 2004;111:481-484. 22. Karam CM, Bustamante MP, Camarena GA. Aspectos sociales de
la mortalidad materna. Estudio de caso en el Estado de México. Medicina Social 2007;2:205-211.
23. Alatorre RJ, Atkin CL. “El embarazo adolescente y la pobreza”, en Paloma Bonil y Vania Salles (eds.) Mujeres pobres: salud y
trabajo. México: Gimtrap; 1998. p. 13-30.
24. Lipman EL, Boyle MH. Social support and education groups for single mothers: a randomized controlled trial of a community-based program. CMAJ 2005;173:1451-1456.
25. Liu S, Liston RM, Joseph KS, et al. Maternal mortality and seve
-re morbidity associated with low risk planned cesa-rean delivery
versus planned vaginal delivery at term. CMAJ 2007;176:455-460.
26. Brace V, Penney G. Learning from adverse outcomes: A system
for identiication and assessment of severe maternal morbidity.