www.elsevier.es/rmuanl
REVIEW
ARTICLE
The
Zika
virus
disease:
An
overview
K.A.
Galán-Huerta
a,
A.M.
Rivas-Estilla
a,
E.A.
Martinez-Landeros
b,
D.
Arellanos-Soto
a,b,
J.
Ramos-Jiménez
b,∗aDepartmentofBiochemistryandMolecularMedicine,SchoolofMedicine,‘‘Dr.JoséEleuterioGonzález’’UniversityHospital,
UniversidadAutónomadeNuevoLeón,Monterrey,N.L.,Mexico
bInfectiousDiseasesService,DepartmentofInternalMedicine,SchoolofMedicine,‘‘Dr.JoséEleuterioGonzález’’University
Hospital,UniversidadAutónomadeNuevoLeón,Monterrey,N.L.,Mexico
Received7May2016;accepted10May2016 Availableonline4July2016
KEYWORDS
Zikavirus; Fever; Outbreak; Americas;
Aedesaegypti
Abstract Thezikavirus,anotherre-emergingFlavivirustransmittedtohumansbymosquitoes, isresponsibleforthemostrecentfeveroutbreakintheAmericasandthePacific,startingin 2015.TheimmunologicallynaïvepopulationintheAmericasfavorsthespreadofepidemics.The zikafeverischaracterizedbyfebrileillness,malaise,conjunctivitisandamaculopapularrash. SimilartootherarbovirosesrecentlyspreadintheAmericas,thereisnospecificoreffective antiviraltherapyandvaccinesarestillintrials.Theonlyeffectivepreventivemeasuresconsist ofindividualprotectionagainstmosquitobitesandvectorcontrol.Thisfebrileillnessincreases theepidemiologicalandpublichealthchallengeexistinginAmerica,wherethepopulationis alreadyfightingagainstdengueandchikungunyafever.Diseasepreventionisimportantdueto theeconomicburdenitentails.Thefactofsexualandtransfusionvirustransmissionisagreat
challengetoovercome.Doctorsneedtodistinguishbetweendengue,chikungunyaandother
diseasestogiveasuccessfultreatmentandpreventthediseasespreading.
©2016PublishedbyMassonDoymaM´exicoS.A.onbehalfofUniversidadAut´onomadeNuevo Le´on.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons. org/licenses/by-nc-nd/4.0/).
∗Correspondingauthorat:ServiciodeInfectología,Facultadde MedicinayHospitalUniversitario ‘‘Dr.José EleuterioGonzález’’, UniversidadAutónoma de Nuevo León,Ave. Francisco I. Madero andAve.Gonzalitoss/n,Col.MitrasCentro,64460Monterrey,N.L., Mexico.
E-mailaddress:[email protected](J.Ramos-Jiménez).
Introduction
Among many public health alerts, the global spread of arbovirusesisofconcernandalarm.TheZikavirusis trans-mittedtopeoplethroughthebiteofaninfectedmosquito from the Aedes genus, mainly Aedes aegypti in tropical and subtropical regions and Aedes albopictus in temper-ateclimates.Thesearethesamemosquitoesthattransmit dengue,Chikungunyaandyellowfever.Thediseaseisnamed Zika virus disease (ZVD) insteadof Zika fever because of the frequent subfebril and afebrile manifestations. Last,
http://dx.doi.org/10.1016/j.rmu.2016.05.003
butnotleast important,theZika virus isthethird recent globalinfectiousdiseaseoutbreak,followingcloselybehind H1N1 flu and the Ebola virus, which has had detrimental implicationsforpregnantwomenandtheirunbornchildren.
Epidemiology
Thefirstisolation wasmadeinApril 1947 fromthe serum of a pyrexial rhesus monkey in the canopy of Zika for-est,Uganda,1followedbyanisolationfromAedesafricanus
mosquitoesin January 1948,in the sameforest. The first human cases were detected in Uganda and the United RepublicofTanzaniain1952,whereneutralizingantibodies totheZikavirusweredetectedinsera.2,3Acoupleofyears
later,in1954,theviruswasisolatedfromagirlinEastern Nigeria.4
Fromthe1960stothe1980s,thezikaviruswasdetected inmosquitoesandsentinelrhesusmonkeysincountriesof equatorial Africa. Sporadic human cases were identified, mostlybyserologicalmethods,butsuchcaseswererareand thediseasewasregardedasbenign.
In1969,theZikavirusexpandeditsgeographical distri-butioninequatorialAsia,whereitisthefirstlargeoutbreak in humans on the Pacific island of Yap, in the Federated StatesofMicronesia.Anestimated73%ofYapresidentsover threeyears of age were infected with the Zika virus. No deaths,hospitalizations,orneurologicalcomplicationswere reported.
From 2012 to 2014, the Zika virus caused outbreaks in French Polynesia, Easter Island, Cook Islands and New Caledonia. Meanwhile, the virus continued circulating in Cambodia,Malaysia,Thailand,Nigeria,SenegalandUganda. ByMarch2015,anillnesscharacterizedbyaskinrashwas detectedinnorthern Brazil.Nevertheless,itwasnotuntil MaywhentheZika virusinfectionwasconfirmed.By July, Brazil reportedlaboratory-confirmed Zika cases in twelve states.InOctober2015,ColombiareportedPCR-confirmed patients with locally acquired Zika infections and poste-riorly 156 confirmed cases in thirteenmunicipalities. The ZikaviruswaslimitedtoBrazilandColombiauntil Novem-ber2015,whenitspreadtoSuriname,Guatemala,Mexico, ElSalvador,ParaguayandVenezuela.InDecember,Panama reporteditsfirstconfirmed cases,aswell asHaiti,Puerto Rico,Martinique,HondurasandFrenchGuiana.5
InJanuary2016,BoliviaandSaintMartindetectedtheir first indigenous cases, as well as Barbados, U.S. Virgin Islands, Dominican Republic, Nicaragua and Jamaica.6 As
ofApril 28, 2016, thenewcountries withconfirmedlocal transmissionsare:Curacao,CostaRica,RepublicofTrinidad andTobago,Aruba,Bonaire,SintMaarten,SaintVincentand the Grenadines, Dominica, Cuba, Saint Lucia and Belize. Thismakesatotalof35countries/territorieswithongoing autochthonous Zika virus transmission and 7982 accumu-latedconfirmedcases.7
In Mexico, the first imported case was identified in November 17, 2015, when a traveler came back from Colombia toQuerétaro. Later in that month, in the 47th EpidemiologicalWeek,thefirsttwocaseswerereportedin Monterrey,NuevoLeón,andinHuixtla,Chiapas.Noneofthe patientshadtraveled recently.8New casesweredetected
untilthe52ndEpidemiologicalWeekinJalisco,Chiapasand
NuevoLeón.9ThefirstEpidemiologicalWeekof2016lacked
confirmedcases.However,Chiapashasbeenreportingnew casessincethe2ndEpidemiologicalWeek.10UptoApril29,
2016,therehave been185confirmedautochthonouscases in Mexico reported fromthe states of Chiapas, Guerrero, Jalisco,Michoacán,Nayarit,NuevoLeón,Oaxaca,Sinaloa, Tabasco,VeracruzandYucatán.11
Eventhoughthereisnoautochthonousongoing transmis-sion in the United States,the presence of Ae. albopictus
inagreatproportionofthecontinentalUSposesariskfor autochthonousZikavirustransmission.12Thegeographic
dis-tributionoftheautochthonoustransmissionoftheZikavirus canbeobservedinFig.1.
Molecular
virology
The Zika virusis a memberofthe Flavivirus genusof the
Flaviviridaefamily.Thisvirusisrelatedtootherpathogenic vectorborneFlavivirus,wherewecanfindtheDenguevirus, theWestNileVirusandtheSaintLouisencephalitisvirus.It isasingle-stranded,positive-sense,RNAviruswithagenome approximately 11kb in length.13 The single open reading
frame (ORF) encoding a polyprotein is framed by 5′ and
3′ untranslatedregions.The encodingpolyproteinis
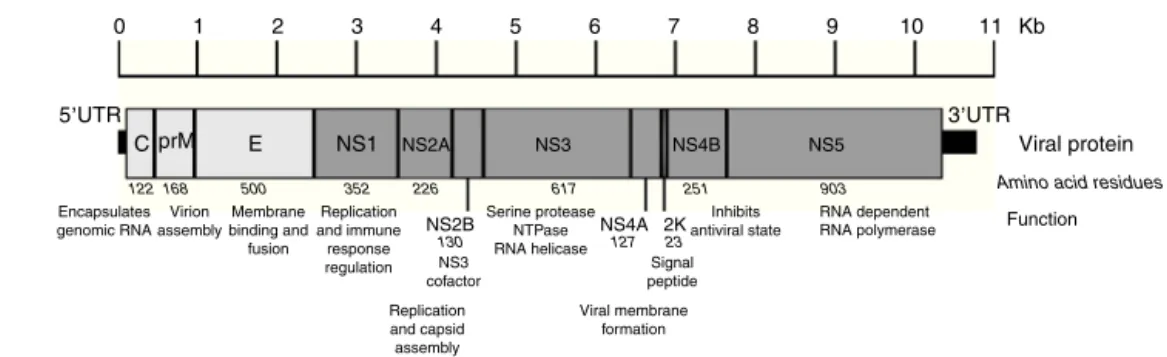
trans-latedandprocessedbyviralandcellularproteases,co-and post-translationally,intothreestructural(capsid,precursor membraneormembrane,andenvelope)andseven nonstruc-tural(NS1,NS2a,NS2b,NS3,NS4a,NS4b,andNS5)proteins (Fig.2).TheNS1,NS3andNS5proteinsarelargeandhighly conserved,meanwhiletheNS2A,NS2B,NS4AandNS4B pro-teinsaresmallandhydrophobic.14
Afteramosquitobite, theZika viruscan infect human dermal fibroblasts, epidermal keratinocytes and imma-ture dendritic cells. AXL, a phosphatydylserine receptor, has been described as a ZIKV entry receptor and is also relatedwithcellularautophagy,enhancingZIKVreplication inpermissivecells. DC-SIGN,Tyro3andTIM-Ialsoseemto mediateZIKVentry.15 InformationconcerningZIKV
replica-tionisscarce; thereforewe present thecommonfeatures of theFlaviviridae familylife cycle. Afterthe viral parti-cleinteractswiththe hostreceptors, itis internalized by clathrin-mediated endocytosis. The low pH of the endo-some induces fusion of the virion envelope with cellular membranes. Following uncoatingof the nucleocapsid,the RNA genome is released intothe cytoplasm. The genome servesthreediscreteroleswithinitslifecycle:asthe mes-senger RNA (mRNA) for translation of allviral proteins, a templateduringRNAreplication,andthegeneticmaterial packagedwithinnewvirusparticles.RNAreplicationoccurs entirelyinthecytoplasmincloseassociationwith intracel-lularmembranes.Progenyvirionsassemblebybuddinginto an intracellular membrane compartment, most likely the endoplasmicreticulum (ER),then transitthroughthehost secretorypathwayandarereleasedatthecellsurface.16
PhylogeneticanalysisamongthegenusFlavivirusplaces ZIKVatcladeX,withtheSpondwenivirus,inthe mosquito-borne cluster.17 Recent phylogenetic analysis divides ZIKV
Cuba
Dominican Republic Puerto Rico
Trinidad and Tobago
Venezuela Guyana
Rio Grande Do Norte
Paraíba
Pernam-buco
Alagoas
Bahia Espirito
Santo Minas Gerais
Goiás
Rio de Janerio Mato Grosso Do Sul
Paraná
Rio Grande Do Sul
Paraguay Bolivia
Mato Grosso Amazonas
Countries / regions with autochthonous ZIKV transmission
GBS cases
Microcephaly cases
Microcephaly and GBS cases
Dominican Republic
Saint Martin/ Sint Maarten
Guadeloupe Dominica Martinique
Saint Lucia 0 520
Kilometers 1040 15602080
N
Saint Vincent and the Grenadines
Barbados Aruba
Curacao Bonaire Puerto Rico
U.S. Virgin Islands
Ecuador Panama Costa Rica Nicaragua Honduras El Salvador
Guatemala Mexico
Jamaica. Belize Haiti
Rondônia
Colombia
Suriname Piauí Ceará Amapá
Pará Maranhao
French Guiana
Figure1 CountriesandregionsintheAmericaswithautochthonousZikavirustransmissionandcomplications.Themap illus-tratesthecountriesandregionswhereautochthonousZikavirustransmissionistakingplace. Italsoshows thecountrieswhere Guillain---Barrésyndromecaseswerereported,aswellasconfirmedmicrocephalycases.MexicoandBrazilaredividedbystates. TheBrazilianstatenamesareinitalics.LatinandNonCaribbeanarenotlabeledduetothemapresolution.Informationupdated April28,2016.ZIKV:Zikavirus;GBS:Guillain---Barrésyndrome.
Source:WorldHealthOrganization,52PanAmericanHealthOrganization,7andSecretariasdeSaúdedosEstadoseDistritoFederal.46
TheAsianlineageisresponsibleforthecurrentoutbreakin America.19
Transmission
Vectortransmission
The Zika virus is mostly transmitted to people through the bite of an infected mosquito from the Aedes genus,
includingAedesaegyptiintropicalandsubtropicalregions andAedesalbopictusintemperateregions.Givennumerous virusisolationsfrommosquitoes,theyareclearlythe natu-ralreservoirs.Vertebratehostsaremostlikelyamplifyingor dead-endhosts,sincenovertebrateinnaturehaseverbeen conclusivelydeterminedtoserveasatruereservoirforany arbovirus.20
SomeoftheprevalentvectorsidentifiedinAfricainclude
0
5,UTR 3,UTR
Viral protein
Amino acid residues
122 168 500 352 226 617
23 Signal peptide NS3
cofactor
Viral membrane formation Replication
and capsid assembly Replication and immune response regulation Membrane binding and fusion Virion assembly Encapsulates genomic RNA
127 130
251 903
RNA dependent Inhibits
antiviral state Serine protease
NTPase RNA helicase
RNA polymerase Function
C prM E NS1 NS2A NS3 NS4B
NS4A
NS2B 2K
NS5
1 2 3 4 5 6 7 8 9 10 11 Kb
Figure2 Zikavirusgenomeorganization.Thefigureshowsthestructuralandnonstructuralproteinsthewaytheyareorganized throughoutthegenomeaswellastheuntranslatedregionsin5′and3′.Thename,sizeinaminoacidsandfunctionisshowedfor
eachprotein.ThefigureisdrawntoscalebasedonthereferenceZIKVgenomewithGenBankaccessnumber:NC012532.1.13The informationregardingviralproteinfunctionwasobtainedfromtheUniProtdatabaseusingdenguevirusduetothelackofpublished data.TheaccessionnumberusedwasP17763.77NS:nonstructuralprotein;C:capsid;E:envelope;prM:precursormembrane;UTR: untranslatedregion;Kb:kilobases.
onsamplinglocation.Interestingly,theinvolvementofAe. aegyptihasbeensmallinAfrica.21 Ontheotherhand,Ae.
aegyptihasbeenthesinglemostimportantvectorin South-eastAsiaandthePacific.IntheoutbreakonYapIslandinthe Pacific,Ae.hensilliwasimplicatedasapossiblevector.22
Ae. albopictusis alsosusceptibletoinfectionandable totransmitZIKV.23 ThehighestconcernisthatAe.
albopic-tushasbeenfoundintemperateclimateswhereAe.aegypti
isabsent,allowingvirustransmissioninthoseregions.This includes 37 of 48 contiguous states of the United States of America, Albania, Bulgaria, Croatia, Southern France, Greece,Italy,Malta,Montenegro,Slovenia,EasternSpain, andSouthernSwitzerland.24,25
Non-vectortransmission
Eventhough themain transmissionroute ofthe Zikavirus isbythebiteofaninfectedmosquito,casesofnon-vector transmissionhavebeenreported.
During the French Polynesian outbreak, 3% of 1505 blood donors, asymptomatic at the time of blood dona-tion,werefoundpositiveforZIKVbyPCR.26,27Inthisrecent
outbreak, two possible cases of transfusion---transmission have been described in Campinas, Brazil and are being investigated.28Forthesereasons,theFoodandDrug
Admin-istration (FDA) has made recommendations to prevent transfusion---transmission.Someoftheserecommendations are:defer donors at risk for ZIKVinfections for 4weeks, use of an FDA-approved pathogen reduction device, and testlocalblooddonationswithanFDA-licensedblooddonor screeningtestforZIKVwhenavailable.29However,arecent
publicationaffirmedthatscreeningpotentialblooddonors basedonsymptomsorserologicaltestingofdonatedblood would dolittle to protectthe blood supply,reducing the risk of an infected donationby at most 30%. The authors advisethathighincidenceareasshouldconsiderPCRtesting toidentifysafecomponentsforuseinpregnantwomen.30
In addition,the Zika virus can besexually transmitted fromamantohissexpartner(s).DuringFebruary2016,the CDC received reports of 14 instancesof suspectedsexual transmissionoftheZikavirus.Amongthese,two laboratory-confirmedcases andfourprobable casesof theZika virus
disease have been identified among women whose only known riskfactor wassexualcontact withasymptomatic malepartnerwithrecenttraveltoanareawithongoingZika virus transmission.31 To date, allreportedcases of sexual
transmissionoftheZikavirushavebeenfromsymptomatic malepartners. Sexualtransmission of theZika virus from infected women to their sex partners and from persons whoareasymptomaticallyinfectedhasnotbeenreported.31
Therehavebeentworeportsofreplication-competentZika virus isolatedfromsemen atleast 2 weeksafteronset of illness,whenbloodplasmaspecimenswerenegativeby RT-PCR.32,33ViralARNhasbeendetectedinsemenbyRT-PCRas
longas62daysafterillnessonset,butthedurationof persis-tenceofinfectiousZikavirusinsemenremainsunknown.34
ThereisnowareportthatindicatesthattheZikaviruscanbe transmittedthroughanalsex,aswellasvaginalsex.35
There-fore,theCentersforDiseaseControlandPreventionissued interimguidanceforthepreventionofsexualtransmission of the Zika virus. Couples in which a woman is pregnant should use condoms or abstain from sexfor the duration of thepregnancy.Likewise,couples inwhich amanhada confirmedZikavirusinfectionorclinicalillnessshould con-sider using condomsor abstaining fromsexfor at least 6 monthsafteronsetofillness.Ifthecouplelivesinanarea withactiveZikavirus transmission,theuseofcondomsor abstaining from sexwhile active transmissionpersistsare recommended.36Evidenceimpliestrans-placental
transmis-sion and perinatal transmissionduring delivery, with Zika virusRNAbeingfoundinamnioticfluidandinpairedblood samplestakenfromnewborninfantsandmothers.37,38There
isnoevidencetosupporttransmissionbybreastfeedingor viacontactwithsaliva,urine,orrespiratorydroplets.
Clinical
features
The first clinical characterizations described Zika virus infectionsasmildandself-limiting.
Afteran experimentallyinduced Zikavirus infection in ahumanvolunteer,itresembledtheconditionobservedin thegirlinEasternNigeriareportedbyMacNamaraclosely.4
Table1 Differentialdiagnosticofmostcommonarbovirusinfectionsinacutepresentations.
Signsandsymptoms ZIKV(%) CHIKV(%) DENV(%) YFV(%) WNV(%)
Fever 65 89 90.6 72 95
Headache 45 47 57.7 54 65
Myalgia 48 60 54.6 36 35
Arthralgia 65 96.1 37.5 ND 35
Arthritis Rare 31.8 3.8 ND ND
Retroocularpain 39 Rare 41.4 ND ND
Non-purulentconjunctivitis 55 Rare 7.7 ND ND
Lymphadenopathy 45 8.9 Rare ND ND
Rash 90 40.1 7 ND 5
Signsofbleeding Rare 6.4 8.3 36 ND
Neurologicsigns Rare 12.1 6 ND 35
Nausea/vomit 10 47 32 30 45
Edema 19 Rare 14.4 ND ND
Jaundice ND ND Rare 34 ND
Source:Duffy,22Pialoux,72Borgherini,73Allonso,74Romano,75andRiabi.76
ZIKV:Zikavirus;CHIKV:chikungunyavirus;DENV:denguevirus;YFV:yellowfevervirus;WNV:WestNilevirus;ND:nodata.
picture of the infection described by a worker that was infected collectingmosquitoesinthe Zikaforestwasthat of amild febrileillness of shortdurationaccompaniedby ageneralizedmaculopapularrash.40 InJava,Indonesia,all
patients had high fevers upon examination. Six of seven patients had stomach ache, five had malaise, five expe-rienced dizzinessandfour wereanorexic. Less frequently reportedsymptomsandsignswerediarrhea,constipation, hypotension and chills. Interestingly, arthralgia, myalgia, vomiting,conjunctivitis,hematuria,lymphadenopathyand legpainwerepresentinoneofthepatients.Furthermore, noneofthepatientshadarash.41 Atastudymadein
Thai-landwithcasesfrom2012to2014,theclinicalpresentation wasmildandnonspecific.Allsubjectspresentedfeveranda maculopapularrash.Othersymptomsincludedsorethroat, arthralgia, myalgia, rhinorrhea, and headache. Only two patientscomplainedof conjunctivitis,whichwasless than theratepreviouslyreportedinZIKVcasesoutsideAfrica.42
The incubation period of the Zika virus disease is not clear, but is estimated to be 4---7 days.30 The symptoms
are similar to other arbovirus infections such as dengue, and includefever, maculopapularrash, pruritus, conjunc-tival hyperemia, myalgia, arthralgia, malaise, headache, retro-orbitalpainanddigestivedisorders.Thesesymptoms are usually mild and last for 2---7 days.22,43 In addition,
commonpresentationsaccompanyingthefebrileillnessare frequentlyconfusedwithdenguevirusinfection,whichmay resultinunderreportingofZikavirus infection.InTable1, we present the frequent signs andsymptoms of themost commonarboviroses.Thiscanbeofgreathelptoclinicians regardingdifferentialdiagnosis.
Complications
WhenZikavirusinfectionswerefirstnoted,therewereno reportsofcomplications,butinrecentZIKVoutbreaksthe incidenceofneurologicaldisordershasincreased.Evidence that neurological disorders, including microcephaly and Guillain---Barrésyndrome,arelinkedtoZikavirusinfection
remainscircumstantial,butagrowingbodyofclinicaland epidemiologicaldatapointstowardacausalrolefortheZika virus.
Microcephaly
There are 6 countries, territories and areas reporting microcephalycases potentially associated withZika virus infection.These areBrazil,CaboVerde,Colombia,French Polynesia,Martinique,andPanama(Fig.1).44
AccordingtotheMinistryofHealthofBrazil,from Octo-ber22,2015throughApril23,2016,therehavebeenreports of7228suspected casesofmicrocephalyor other nervous systemmalformationsamongnewbornsacrossthecountry. Thiscontrastswiththeperiodfrom2001to2014,whenan averageof163microcephalycaseswasrecordednationwide peryear.45 Up toApril 23, 2016, BrazilHealth authorities
have reviewed 3518 cases, 49% of the total. They iden-tified1198 confirmed casesof microcephaly and/or other centralnervoussystem(CNS)malformationswithevidence suggestive of congenital infection, and discarded 2320.46
The 1198 confirmed microcephaly cases occurred in 435 municipalitieslocatedin22BrazilianFederalUnits:Alagoas, Bahia, Ceará,Maranhão, Paraíba,Pernambuco, Piauí, Rio GrandeDoNorte,Sergipe,EspíritoSanto,MinasGerais,Rio deJaneiro,Amapá,Amazonas,Pará,Rondônia,Distrito Fed-eral,Goiás,Mato Grosso,MatoGrossoDoSul,Paraná,and RioGrandeDo Sul.46 There havebeen 251deaths
(includ-ingmiscarriagesorstillbirths)reportedamongmicrocephaly and/orCNSmalformationcases.Fifty-fourofthesedeaths were confirmed as having microcephaly and/or CNS mal-formation, 167 remain under investigation and 30 were discarded.46 There is evidence that in additionto
micro-cephaly,theremaybealink betweenZika virusinfection andhydropsfetalisandfetaldemise.47
identified19cases,includingeightwithmajorbrainlesions andsevere microcephaly, six withsevere cerebral lesions withoutmicrocephalyandfivewithbrainstem dysfunction without visible malformations. Of the five-microcephaly casesthatweretestedvirologically,viralARNwasdetected by RT-PCR and infectious ZIKV isolates were obtained in four.Wheninterviewed,themothersoffourcasesreported clinical infection in the first trimester of pregnancy. The remainingmothercouldnotbereached.48
Acase seriesof pregnantU.S. womenthat traveled to Zikaaffectedareasreportedthatinfectionduringpregnancy wasassociated witha rangeof outcomes, includingearly pregnancylosses,congenitalmicrocephaly,andapparently healthyinfants.Inaddition,viralRNAwasdetectedinfetal remains of early pregnancy loss, amniocentesis fluid,and placenta.49
On March 30th, Colombia reported 50 live births with microcephalybetween January4th,2016and March20th, 2016. Of the 50 cases registered, 16 were discarded for microcephalywithsuspectedassociationwiththeZikavirus. Oftheremaining34cases,twowereruledoutfornot meet-ingthenationalcriteriaforassociationwithmicrocephalyby Zikavirus.Theremainingcases(32)areunderinvestigation. Sofar, eightof these32 casesof microcephalypresented positiveZikavirusresultsbyRT-PCR.44
ArecentstudyfromPernambuco,Brazil,establishedthat 30of31studiedmicrocephalycaseshadZika-specificIgMin theirCSF.SinceIgMdoesnotcrosseithertheplacentabarrier ortheblood---brain barrier,thepresenceofIgMin theCSF indicatesthattheneonatehadtheinfectionintheCNS.This isstrongevidencethatmicrocephalywasaconsequenceof Zikavirusinfection.50
A group of researchers evaluated the available data regarding ZIKV and microcephaly using criteria that have beenproposedfor theassessmentofpotentialteratogens. Theyconcludedthatthereisacausalrelationshipbetween prenatal Zika virus infection and microcephaly and other seriousbrainanomalies.51
The link between ZIKV infection and microcephaly becomes stronger with every new case report published. However,casereports,unlikecohortstudies,donot estab-lisha causativelink between the virus andmicrocephaly. Moreresearchisneededtoclearlyestablishtherelationship betweenZIKVinfectionandmicrocephaly.
Guillain---Barré
syndrome
According to the WHO, during 2015 and 2016, thirteen countriesand territories have reportedan increased inci-denceofGuillain---Barrésyndrome(GBS)and/orlaboratory confirmationofaZikavirusinfectionamongGBScases.52
Countries where there is increased incidence of GBS cases, with at least one GBS case with confirmed Zika virus infectionare:Brazil,Colombia, DominicanRepublic, El Salvador, French Polynesia, Honduras, Suriname, and Venezuela. In contrast, the countries reporting GBS with laboratoryconfirmedZikavirusinfectionswithoutincrease of GBS incidence are: French Guiana, Haiti, Martinique, Panamaand Puerto Rico.52 Countries or territories where
GBScaseswerereportedcanbeseeninFig.1.
Thereislittleinformationinrespecttotheclinical char-acteristics of the Guillain---Barré syndrome cases caused by this virus. The most complete description is from a case-control study made in French Polynesia, where they diagnosed 42casesof Guillain---Barrésyndrome. Forty-one (98%)patientshadanti-ZikavirusIgMorIgG,andall(100%) hadneutralizingantibodiesagainsttheZikavirus.53
Mostpatientshadelectrophysiologicalfindings compati-blewiththeacutemotoraxonalneuropathy(AMAN)typeof thesyndrome,andhadrapidevolutionofthedisease.53The
clinical outcomeof thesepatientswiththeZikavirus and Guillain---Barré syndrome wasgenerally favorable, despite a rapid onset and short plateau phase, as may be seen in other patient groups suffering from the AMAN type of Guillain---Barrésyndrome.Eventhoughitisverylikelythat these patients had been recently infected with the Zika virus, itispossible thatthediseasewasduetodengueor mightpossiblyhavebeenunrelatedtoFlavivirusinfection.53
Arecent case report showedthat a housekeeper from Rio deJaneiro thatpresented clinical features consistent with paraparetic Guillain---Barré syndrome, had a positive PCR testfor ZIKVinserum,cerebrospinalfluid,salivaand urine.It isnoteworthythat thepatient’sserumand cere-brospinalfluidwerenegativefordengueandchikungunyaby real-timePCR.54Thisstudyhelpstoconfirmtheassociation
betweenZIKVandGBS.
Substantialnew research has strengthened the associ-ation between the Zika infection and the occurrence of neurological disorders.55 However, more investigation is
needed to better understand this relationship. Confound-ingfactorsincludethecontemporarycirculationofdengue andchikungunyaintheAmericas,whicharetransmittedby thesamespeciesofmosquito.
Clinical
and
laboratory
diagnosis
of
Zika
Even though the Zika virus was discovered decades ago, therearenolicensedorbroadlydistributeddiagnostictests. AccordingtotheWHO,asuspectedcaseofZikavirusdisease isdefinedasapatientwitharashandtwoormoreofthe following signs or symptoms: fever, usually<38.5◦C,
con-junctivitis (non-purulent/hyperemic), arthralgia, myalgia, and/orperi-articularedema.AarobablecaseofZikavirus diseaseisapatientwhomeetsthecriteriaofasuspected caseandhasZikaIgMantibodies,withnoevidenceof infec-tionwithotherflaviviruses.AconfirmedcaseofZikavirus diseaseisapatientwhomeetsthecriteriaforasuspected case and has laboratory confirmation of recent Zika virus infection.Thisconfirmationcanbethefollowing:viralRNA (serum,urine,saliva,tissueorwholeblood),positiveZika IgMantibodiesandplaquereductionneutralization(PRNT90)
for Zikavirus titers ≥20 andfour(or more)times greater thanthetitersforotherflaviviruses,withtheexclusionof other Flaviviruses.Inautopsyspecimens,detectionof the viralgenomeshouldbebymoleculartechniques,orantigen detectionbyimmunohistochemistry.56
Suspected Zika virus disease
Acute phase 1-5 days
NS1/RT-PCR DENV
Positive
DENV confirmed
Negative
consider ZIKV
IgM CHIKV
IgM ZIKV
ZIKV+ DENV–
presumptive ZIKV
ZIKV– DENV+
presumptive DENV RT-PCR
CHIKV
Positive
CHIKV confirmed Negative
ZIKV+ DENV+
flavivirus infection
ZIKV– DENV– negative IgM
DENV
Positive presumptive
DENV Negative
Consider ZIKV
Positive
presumptive CHIKV
RT-PCR ZIKV
Positive
ZIKV confirmed
Negative
consider CHIKV Days after
onset of symptoms Convalescent phase
≥ 6 days
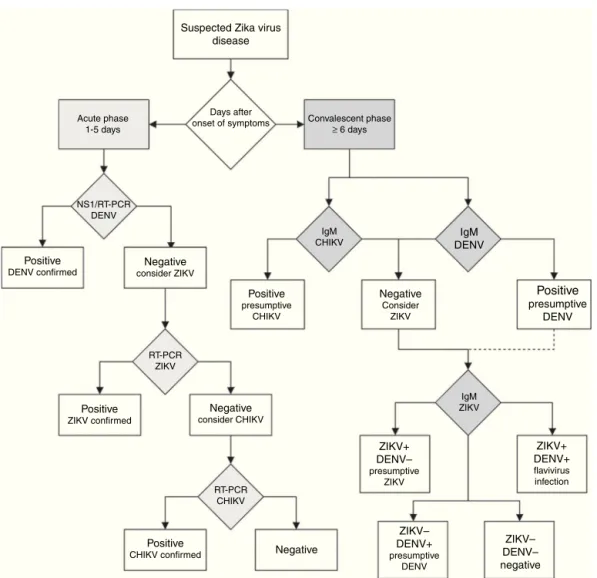
Figure3 DiagnosticalgorithmfordetectingZikavirusandrelatedarbovirus.Thisalgorithmisadaptedfromtheoneproposed bythePanAmericanHealthOrganization.65Duetocross-reactivityinsecondaryFlavivirusinfections,ELISAforIgMagainstDengue virusissuggested.NS1:non-structuralprotein1;RT-PCR:real-timepolymerasechainreaction;DENV:denguevirus;ZIKV:Zikavirus; CHIKV:chikungunyavirus;IgM:immunoglobulinM.
laboratory capacities are limited, the arbovirus diagnosis is often performed by serologic testing by IgM ELISA or rapidtests.Ifrapidtestsareusedfordengue,itis recom-mendedtouseacombinedNS1antigenandIgMantibodytest toincrease the sensitivityand specificityof denguefever diagnosis.58 IfseveralpatientsarenegativetoaDENVNS1
testwithinthefirstweek ofa‘‘dengue-likedisease,’’the Zikavirusdiseaseorotherarbovirusesshouldbesuspected. Incountrieswithadvancedlaboratorycapacities,aRT-PCR assayshouldbethefirst-linetest.Patientswithintheacute phaseofinfection withadengueor chikungunya-like syn-drome, or fever and rash, withnegativeDENV andCHIKV RT-PCRassaysshouldbetestedwithaspecificZIKVRT-PCR assay.57ThealgorithmforZikavirusdetectioninFig.3can
beausefulguideforclinicians.
There are two strategies for the molecular detection ofZIKV.Oneis thedetectionofFlavivirusesusing consen-susprimersandposteriordetectionofspecificZIKVARN.59
The other strategy is to use specific ZIKV primers and probes.Severalprotocolshavebeendevelopedtotargetthe E-encodinggene,60themembrane-envelopejunction
(M/E-encoding gene),the partialenvelope (pE)-encoding gene,
andtheNS5-encodinggene.61,62 Furthermore,ZIKVRT-PCR
do not cover the genetic diversity and geographic distri-butionofallZIKVstrains.61 The reasonis thattheprimers
andprobeshavebeendesignedusingonlythefewfullZIKV genomesequencesavailable. On March17,2016, theFDA issuedan EmergencyUseAuthorization (EUA)toauthorize theemergencyuseoftheCDC’sTrioplexReal-timeRT-PCR Assayfor the qualitative detection and differentiation of RNAfromtheZikavirus,denguevirus,andchikungunyavirus inhumanseraorcerebrospinalfluid,andforthequalitative detectionofZikavirusRNAinurineandamnioticfluid.63On
April28,2016,FocusDiagnostics,Inc.’sZikaVirusRNA Qual-itativeReal-TimeRT-PCRtestwasauthorizedundertheEUA forthequalitativedetectionofRNA fromtheZikavirusin humanserumspecimens.Thisisthefirstcommercialtestto detecttheZikavirusthathasbeenauthorizedbytheFDA foremergencyuse.63
is expensive, and may require regulated laboratories becauseofthemanipulationofliveviruses.64Todate,there
is no validated commercial serology kit for ZIKV, but on February26,2016,theFDAissuedanEmergencyUse Autho-rizationfortheemergencyuseofCDCZikaImmunoglobulin MAntibody Capture Enzyme-Linked Immunosorbent Assay (Zika MAC-ELISA) for the presumptive detection of Zika virus-specific IgM in human sera or cerebrospinal fluid.63
Samplesforserologicormoleculartestingshouldhave spe-cialstorageconditions,rangingfromrefrigeration(2---8◦C)
tofreezing(−10to−20◦Cor−70◦C)dependingofthetime
andsiteoftesting.65
Treatment
Similar to other arboviral diseases, there is no specific antiviral drug treatment for ZIKV infection. Symptomatic treatment is recommended after excluding more serious conditionslikemalaria,dengue,andbacterialinfections.In acuteinfection,treatment issymptomaticandsupportive, consistingofrestandtheuseofacetaminophentorelieve fever(<4g/day).Theuseofibuprofen,naproxen,oranother non-steroidal anti-inflammatory agents (NSAID) to relieve thearthritic componentof the diseasecan beusedwhen dengueinfectionisdiscarded.Patientsshouldbeadvisedto drinkplentyoffluidstoreplenishfluidlostfromsweating, vomiting,andotherinsensiblelosses.66
There are specific guidelinesfor health care providers caring for infants and children with possible Zika virus infection at the official CDC website. These guidelines recommend clinical evaluation and laboratory testing for infants withpossible congenital Zika virus infection, with orwithoutmicrocephalyorintracranialcalcifications.67
The CDC has also put out guidelines for health care providerscaringfor women ofreproductive agewith pos-sibleZikavirusexposure. Womenwhohave hadZikavirus diseaseor exposurewithoutclinicalillness,shouldwaitat least8weeksaftersymptomonsettoattemptconception. MenwithZikavirus diseaseshouldwait at least6months aftersymptomonset,or8weeksafterexposuretothevirus withoutclinicalillness,toattemptconception.These guide-linesalsoprovideupdatedrecommendationsforthetesting ofpregnantwomenwithpossibleZikavirusexposure.68Itis
importanttonotethatthecurrent guidanceisbasedona limitedbodyofevidence.
Prevention
Pendingvaccinedevelopment,theonlyeffectivepreventive measuresconsistofindividualprotectionagainstmosquito bites andvector control.Control of both adult andlarval mosquitopopulations usesthe same model asfor dengue and has been relatively effective in many countries and settings.Mosquitocontrolisthebestavailablemethodfor preventingZIKVinfection.Breedingsitesmustberemoved, destroyed,frequentlyemptied,andcleanedortreatedwith insecticides.43
Forprotection,clothing whichminimizesskin exposure to the day-biting vectors is advised. Repellents can be applied to exposed skin or to clothing, in strict accor-dance with product label instructions. Repellents should
contain DEET (N, N-diethyl-3-methylbenzamide), IR3535 (3-[N-acetyl-N-butyl]-aminopropionic acid ethyl ester) or icaridin (1-piperidinecarboxylic acid, 2-(2-hydroxyethyl)-1-methylpropylester). Mosquito coils or other insecticide vaporizersmayalsoreduceindoorbiting.69
Aspreviouslymentioned,thecorrectandconsistentuse ofcondomsduringanysexualintercourseisencouragedto preventthesexualtransmissionoftheZikavirus.Another, althoughdifficult,optionissexabstentionwhileactivevirus transmissionpersists.36
Vaccines
UptoMarch,2016thereisnoavailablevaccineagainstthe Zikavirus.Thereareseveralproposalsforavaccine,using thesamemethodologyasotheranti-flavivirusesvaccines70;
nevertheless, the process is still long. There are ethical issues involving pregnant women and the ‘‘safe use’’ of vaccines,whicharestillabarrier.71
Future
directions
There are still many unanswered questions regarding the Zikavirusdisease.Clinicalandepidemiologicalstudiesmust beperformedtodescribeviraldynamicsandtheexpansion of the outbreak. More studies areneeded toconfirm the suspected association between ZIKVinfection with micro-cephaly and Guillain---Barré syndrome. Research must be donetoidentifyanantiviral,prophylactic,or immunother-apyvaccineaswellasdiagnosticELISAtesting.
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest inwritingthismanuscript.
References
1.Dick GW, Kitchen SF, Haddow AJ. Zika virus. I. Isolat-ions and serological specificity. Trans R Soc Trop Med Hyg. 1952;46:509---20.
2.DickGW.Zikavirus.II.Pathogenicityandphysicalproperties. TransRSocTropMedHyg.1952;46:521---34.
3.SmithburnKC.Neutralizingantibodiesagainstcertainrecently isolatedvirusesin theseraof humanbeingsresidingin East Africa.JImmunol.1952;69:223---34.
4.MacnamaraFN.Zika virus:a reportonthreecasesofhuman infectionduringanepidemicofjaundiceinNigeria.TransRSoc TropMedHyg.1954;48:139---45.
5.KindhauserMK,AllenT,FrankV,SanthanaR,DyeC.Zika:the ori-ginandspreadofamosquito-bornevirus.BulletinoftheWorld HealthOrganization;2016.
6.Pan American Health Organization. Countries and territories withautochthonous transmission in theAmericas --- EW4 of 2016;2016.
7.PanAmericanHealthOrganization.Cumulativesuspectedand confirmedcases reportedbycountriesand territories inthe Americas;2015---2016.Updatedasof28April2016.
9.DirecciónGeneraldeEpidemiología.VigilanciaEpidemiológica ---Semana52,2015.BoletínEpidemiológico.2015;32:1---64. 10.DirecciónGeneraldeEpidemiología.VigilanciaEpidemiológica
---Semana2,216.BoletínEpidemiológico.2016;33:1---64. 11.Dirección General de Epidemiología. Casos Confirmados de
InfecciónporVirusZika.Semanaepidemiológica16de2016; 2016.
12.MonaghanA,MorinC,SteinhoffD,etal.Ontheseasonal occur-renceandabundanceoftheZikavirusvectormosquitoAedes aegyptiinthecontiguousUnitedStates.PLOSCurrOutbreaks. 2016;8.
13.KunoG, ChangGJ.Full-lengthsequencingandgenomic char-acterizationofBagaza,Kedougou,andZikaviruses.ArchVirol. 2007;152:687---96.
14.ChambersTJ,HahnCS,GallerR, RiceCM.Flavivirusgenome organization,expression,andreplication.AnnuRevMicrobiol. 1990;44:649---88.
15.HamelR,DejarnacO,WichitS,etal.BiologyofZikavirus infec-tioninhumanskincells.JVirol.2015;89:8880---96.
16.Lindenbach BD, Murray CL, Heinz-Jürgen T, Rice CM. Fla-viviridae. In: KnipeDM, Howley PM,editors. Fieldsvirology. Philadelphia, PA: Lippincott Williams & Wilkins; 2013. p. 712---46.
17.KunoG,ChangGJ,TsuchiyaKR,KarabatsosN,CroppCB. Phy-logenyofthegenusFlavivirus.JVirol.1998;72:73---83. 18.FayeO,FreireCC,IamarinoA,etal.MolecularevolutionofZika
virusduringitsemergenceinthe20(th)century.PLoSNeglTrop Dis.2014;8:e2636.
19.EnfissiA,CodringtonJ,RoosbladJ,KazanjiM,RoussetD.Zika virusgenomefromtheAmericas.Lancet.2016;387:227---8. 20.KunoG,ChangGJ.Biologicaltransmissionofarboviruses:
reexa-minationofandnewinsightsintocomponents,mechanisms,and uniquetraitsaswellastheirevolutionarytrends.ClinMicrobiol Rev.2005;18:608---37.
21.BoormanJP,PorterfieldJS.Asimpletechniqueforinfectionof mosquitoeswithviruses;transmissionofZikavirus.TransRSoc TropMedHyg.1956;50:238---42.
22.DuffyMR,Chen TH, HancockWT, et al. Zika virus outbreak onYapIsland,FederatedStatesofMicronesia.NEnglJMed. 2009;360:2536---43.
23.WongPS,LiMZ,ChongCS,NgLC,TanCH.Aedes(Stegomyia) albopictus(Skuse):apotentialvectorofZikavirusinSingapore. PLoSNeglTropDis.2013;7:e2348.
24.CenterforDiseaseControlandPrevention.Vectorsurveillance andcontrol|Zikavirus|CDC;2016.http://www.cdc.gov/zika/ vector/index.html[accessed01.04.16].
25.European Centre for Disease Control and Prevention. Aedes albopictus; 2016. http://ecdc.europa.eu/en/healthtopics/ vectors/mosquitoes/Pages/aedes-albopictus.aspx [accessed 01.04.16].
26.AubryM,FinkeJ,TeissierA,etal.Seroprevalenceofarboviruses amongblooddonorsinFrenchPolynesia,2011---2013.IntJInfect Dis.2015;41:11---2.
27.MussoD,NhanT,RobinE,etal.PotentialforZikavirus transmis-sionthroughbloodtransfusiondemonstratedduringanoutbreak inFrench Polynesia, November 2013to February 2014. Euro Surveill.2014:19.
28.BoadleA.BrazilreportsZikainfectionfrombloodtransfusions. Reuters; 2016. http://www.reuters.com/article/us-health-zika-brazil-blood-idUSKCN0VD22N[accessed01.04.16]. 29.Food and Drug Administration. Recommendations for donor
screening,deferral,andproductmanagementtoreducetherisk oftransfusion---transmissionofZika virus.Rockville,MD:U.S. DepartmentofHealthandHumanServices;2016.
30.LesslerJT,OttCT,CarcelenAC,etal.Timestokeyeventsin thecourseofZikainfectionandtheirimplications:asystematic reviewandpooledanalysis.BullWorldHealthOrgan.2016.
31.HillsS,RussellK,HennesseyM,etal.TransmissionofZikavirus throughsexualcontactwithtravelerstoareasofongoing trans-missionincontinentalUnitedStates,2016. MorbMortalWkly Rep.2016;65:215---6.
32.MansuyJM,DutertreM,MengelleC,etal.Zikavirus:high infec-tiousviralloadinsemen,anewsexuallytransmittedpathogen? LancetInfectDis.2016;16:405.
33.MussoD,RocheC,RobinE,NhanT,TeissierA,Cao-LormeauVM. Potentialsexualtransmission ofZikavirus.Emerg InfectDis. 2015;21:359---61.
34.AtkinsonB,HearnP,AfroughB,LumleyS,CarterD,AaronsEJ. DetectionofZika virusinsemen.Emerg Infect Dis.2016;22: 940.
35.DeckardDT,ChungWM,BrooksJT,etal.Male-to-malesexual transmissionofZikavirus---Texas,January2016.MorbMortal WklyRep.2016;65:372---4.
36.OsterAM,RusselK,EllenSJ,etal.Update:interimguidancefor preventionofsexualtransmissionofZikavirus---UnitedStates, 2016.MorbMortalWklyRep.2016;65:323---5.
37.CalvetG,AguiarRS,MeloAS,etal.Detectionandsequencing ofZikavirusfromamnioticfluidoffetuseswithmicrocephaly inBrazil:acasestudy.LancetInfectDis.2016.
38.BesnardM,LastereS,TeissierA,Cao-LormeauV,MussoD. Evi-denceofperinataltransmissionofZikavirus,FrenchPolynesia, December2013andFebruary2014.EuroSurveill.2014;19. 39.BearcroftWG.Zikavirusinfectionexperimentallyinducedina
humanvolunteer.TransRSocTropMedHyg.1956;50:442---8. 40.SimpsonDI.Zikavirusinfectioninman.TransRSocTropMed
Hyg.1964;58:335---8.
41.Olson JG, KsiazekTG, Suhandiman,Triwibowo. Zika virus,a causeoffeverinCentralJava,Indonesia.TransRSocTropMed Hyg.1981;75:389---93.
42.BuathongR,HermannL,ThaisomboonsukB,etal.Detectionof ZikaVirusInfectioninThailand,2012---2014.AmJTropMedHyg. 2015;93:380---3.
43.World Health Organization. Zika virus --- fact sheet. World HealthOrganization;2016.http://www.who.int/mediacentre/ factsheets/zika/en/[accessed04.03.16].
44.World Health Organization. Zika situation report --- Zika virus,microcephalyandGuillain---Barré syndrome--- 31March 2016.WorldHealthOrganization;2016.http://www.who.int/ emergencies/zika-virus/situation-report/31-march-2016/en/ [accessed02.04.16].
45.Pan American Health Organization. Zika epidemiological update --- 31 March 2016. Pan American Health Organiza-tion; 2016. http://www.paho.org/hq/index.php?option= comdocman&task=docview&Itemid=270&gid=34041&lang=en [accessed02.04.16].
46.Centro de Operac¸ões de Emergências em Saúde Pública SobreMicrocefalias.InformeEpidemiológicoNo23---Semana Epidemiológica (SE) 16/2016 (17/04 A 23/04/2016) --- Moni-toramentoDosCasosDeMicrocefaliaNoBrasil;2016.http:// combateaedes.saude.gov.br/images/sala-de-situacao/informe microcefaliaepidemiologico19.pdf[accessed02.05.16]. 47.SarnoM,SacramentoGA,KhouriR,etal.Zikavirusinfection
andstillbirths:acaseofhydropsfetalis,hydranencephalyand fetaldemise.PLoSNeglTropDis.2016;10:e0004517.
48.BesnardM,Eyrolle-GuignotD,Guillemette-ArturP,etal. Con-genitalcerebralmalformationsanddysfunctioninfetusesand newborns following the2013 to 2014 Zika virus epidemicin FrenchPolynesia.EuroSurveill.2016:21.
49.Meaney-Delman D, Hills S, Williams C, Galang R, Iyengar P. Zika virus infection among U.S. pregnanttravelers ---August 2015---February2016.MorbMortalWklyRep.2016;65:211---4. 50.CordeiroMT,Pena LJ, BritoCA,GilLH, MarquesET.Positive
51.RasmussenSA,JamiesonDJ,HoneinMA,PetersenLR.Zikavirus andbirthdefects---reviewingtheevidenceforcausality.NEngl JMed.2016;374:1981---7.
52.World Health Organization. Zika situation report --- Zika virus, microcephaly and Guillain---Barré syndrome --- 21 April 2016.WorldHealthOrganization;2016.http://www.who.int/ emergencies/zika-virus/situation-report/21-april-2016/en/ [accessed02.05.16].
53.Cao-LormeauV-M,BlakeA,MonsS,etal.Guillain---Barré syn-dromeoutbreakassociatedwithZikavirusinfectioninFrench Polynesia:acase---controlstudy.Lancet.2016;387:1531---9. 54.BrasilP,SequeiraPC,FreitasAD,etal.Guillain---Barresyndrome
associatedwithZikavirusinfection.Lancet.2016;387:1482. 55.BroutetN,KrauerF,RiesenM,etal.Zikavirusasacauseof
neurologicdisorders.NEnglJMed.2016;374:1506---9. 56.Pan American Health Organization. Case definitions; 2016.
http://www.paho.org/hq/index.php?option=comcontent& view=article&id=11117&Itemid=41532&lang=en [accessed 04.04.16].
57.Musso D,Gubler DJ. Zika virus. ClinMicrobiol Rev.2016;29: 487---524.
58.FrySR,MeyerM,SempleMG,etal.Thediagnosticsensitivity ofdenguerapidtestassaysissignificantlyenhanced byusing acombinedantigenandantibodytestingapproach.PLoSNegl TropDis.2011;5:e1199.
59.LanciottiRS.Molecularamplificationassaysforthedetection offlaviviruses.AdvVirusRes.2003;61:67---99.
60.Faye O, Dupressoir A, Weidmann M, Ndiaye M, Alpha Sall A. One-step RT-PCR for detection ofZika virus.JClinVirol. 2008;43:96---101.
61.FayeO,DialloD,DialloM,WeidmannM,SallAA.Quantitative real-timePCRdetectionofZikavirusandevaluationwith field-caughtmosquitoes.VirolJ.2013;10:311.
62.BalmMN,LeeCK,LeeHK,ChiuL,KoayES,TangJW.A diagnos-ticpolymerasechainreactionassayforZikavirus.JMedVirol. 2012;84:1501---5.
63.FoodandDrugAdministration.Zikavirusemergencyuse autho-rization. U.S. Food and Drug Administration; 2016. http:// www.fda.gov/MedicalDevices/Safety/EmergencySituations/ ucm161496.htm[accessed02.05.16].
64.World Health Organization. Guidelines for plaque reduction neutralizationtestingofhumanantibodiestodengueviruses. Geneva,Switzerland:WorldHealthOrganization;2007.
65.PanAmericanHealthOrganization.Zikavirussurveillanceinthe Americas:laboratorydetectionanddiagnosis.Washington,DC: PanAmericanHealthOrganization;2016.
66.Centers for Disease Control and Prevention. Zika virus ---clinical evaluation & disease. Centers for Disease Control andPrevention;2016.http://www.cdc.gov/zika/hc-providers/ clinicalevaluation.html[accessed04.03.16].
67.Fleming-DutraKE,NelsonJM,FischerM,etal.Update:interim guidelinesforhealthcareproviderscaringforinfantsand chil-drenwithpossibleZikavirusinfection---UnitedStates,February 2016.MorbMortalWklyRep.2016;65:182---7.
68.PetersenEE,PolenKN,Meaney-DelmanD,etal.Update:interim guidanceforhealthcareproviderscaringforwomenof repro-ductiveagewithpossibleZikavirusexposure---UnitedStates, 2016.MorbMortalWklyRep.2016;65:315---22.
69.Center for Disease Control and Prevention. Zika virus pre-vention. Centers for Disease Control and Prevention; 2016. http://www.cdc.gov/zika/prevention/index.html [accessed 04.03.16].
70.CohenJ.Infectiousdisease.TheraceforaZikavaccineison. Science.2016;351:543---4.
71.OmerSB,BeigiRH.PregnancyinthetimeofZika:addressing barriers for developing vaccines and other measures for pregnantwomen.JAMA.2016;315:1227---8.
72.Pialoux G, Gauzere BA, Jaureguiberry S, Strobel M. Chikungunya, an epidemic arbovirosis. Lancet Infect Dis. 2007;7:319---27.
73.BorgheriniG,PoubeauP,StaikowskyF,etal.Outbreakof chikun-gunyaonReunionIsland:earlyclinicalandlaboratoryfeatures in157adultpatients.ClinInfectDis.2007;44:1401---7. 74.Allonso D,Meneses MD, FernandesCA, FerreiraDF,
Mohana-BorgesR.Assessingpositivityand circulatinglevelsofNS1in samplesfroma2012dengueoutbreakinRiodeJaneiro,Brazil. PLOSONE.2014;9:e113634.
75.RomanoAP,CostaZG,RamosDG,etal.YellowFeveroutbreaks inunvaccinatedpopulations,Brazil,2008---2009.PLoSNeglTrop Dis.2014;8:e2740.
76.RiabiS,GaaloulI,MastouriM,HassineM,AouniM.Anoutbreak ofWestNileVirusinfectionintheregionofMonastir,Tunisia, 2003.PathogGlobHealth.2014;108:148---57.