http://journals.iztacala.unam.mx/index.php/amta/
CASE
REPORT
Normalizing
the
eating
pattern
with
virtual
reality
for
bulimia
nervosa:
a
case
report
María
Roncero
a,∗,
Conxa
Perpi˜
ná
b,caUniversityofZaragoza,Zaragoza,Spain
bUniversityofValencia,Valencia,Spain
cCIBERFisiopatologíaObesidadyNutrición(CIBERobn),InstitutoSaludCarlosIII,Spain
Received21June2015;accepted30October2015 Availableonline1December2015
KEYWORDS
Eatingdisorders; Bulimiapurgative subtype;
Virtualreality; Casestudy
Abstract Theaimofthepresentstudywastoanalyzetheeffectsofavirtualreality(VR) com-ponentasatherapeutictooltonormalizeeatingpatterns,aspartofthecognitive-behavioral treatmentofabulimianervosa(BN)patient.Resultsindicatedthatthepatientmade signifi-cantprogresswithhereatinghabits;bingesandvomitswereeliminatedcompletely.Moreover, whentheVRstartedthepatientavoidedfood,especiallymeat(5over5),anditwasreduction ofthisavoidanceinthelastssessions(2 and3over5). Itwas alsoobserved areductionin theavoidanceandthefearofeating(from10and9to6and5respectively)andincreasedthe impulsecontrol(from2to7).ThepatientfeltthattheVRexperienceseemedrealandsimilar toreality(meanscoreof8.3over10).Before andafter thesevenVRsessions,therewasa decreaseinthedriveforthinness,bulimia,ineffectiveness,andBITEsymptomsandseverity, andinthegeneralpsychopathology.Moreover,thepatientimprovedhermotivationtochange. ResultssuggestthatVRisarelevantandeffectivecomplementtotraditionaltreatmentinaBN patient.Furtherstudiesshouldcontinuethislineofresearchbyusinglargersamplesizeswith differentdiagnosesandsubtypesandcontrolgroups.
AllRights Reserved©2015Universidad NacionalAutónomadeMéxico,FacultaddeEstudios SuperioresIztacala.Thisisanopenaccess itemdistributedundertheCreativeCommonsCC LicenseBY-NC-ND4.0.
∗Correspondingauthor.
E-mailaddress:[email protected](M.Roncero).
PeerReviewundertheresponsibilityofUniversidadNacionalAutónomadeMéxico.
http://dx.doi.org/10.1016/j.rmta.2015.11.001
PALABRASCLAVE
Trastornosdela conducta alimentaria; Bulimianerviosa subtipopurgativo; Realidadvirtual; Estudiodecaso
Normalizacióndelaingestaconrealidadvirtualenlabulimianerviosa:uncaso clínico
Resumen Elobjetivodelpresenteestudiofueanalizarelefectodeuncomponentederealidad virtual(RV)comounaherramientadeterapiaparalanormalizacióndelaingesta,comoparte deuntratamientocognitivoconductualparalabulimianerviosa(BN).Despuésdeunmódulo de 7sesionesdeRV, la paciente tuvoun progresosignificativoen sushábitos alimentarios. Los atraconesy vómitosseeliminaroncompletamente.Además,al iniciodelassesiones,la pacienteevitabalacomida,especialmentelacarne(5sobre5),observándoseunareducción delaevitaciónenlasúltimassesiones(2y3sobre5).Tambiénseredujeronlaevitaciónyel miedoacomer(de10y9a6y5,respectivamente)yaumentóelcontroldelimpulso(de2 a7).Lapacientesintiócomoreallaexperienciavirtualyfueevaluadacomosimilaraloque experimentaenlavidareal(puntuaciónmediade8,3sobre10).Despuésdelas7sesionesde RV,hubounareducciónenelimpulsoporadelgazar,bulimia,ineficacia,enlossíntomasyla gravedaddelBITE,yenlapsicopatologíageneral.Además,lamotivaciónalcambiomejoróen la paciente.Losresultados indicanquelaRVesuncomplementorelevanteyefectivoenel tratamientotradicional enunapacienteconBN.Serequierenfuturosestudiosenestalínea muestrasmásampliascondiferentesdiagnósticosysubtiposygrupocontrol.
DerechosReservados©2015UniversidadNacionalAutónomadeMéxico,FacultaddeEstudios SuperioresIztacala. Esteesunartículodeaccesoabiertodistribuidobajolostérminosdela LicenciaCreativeCommonsCCBY-NC-ND4.0.
Introduction
Inthepast20 years,therehasbeenincreasinginterestin theuseofvirtualreality(VR),acomputationaltechnology, inthementalhealtharea.Virtualenvironmentshavebeen created for clinical use to expose patients to their fears (Bush,2008).Thistechnologyallowsclinicianstocreatea safeenvironment that canbe customized andadapted to each patient underthe strict supervisionof the therapist (Wiederholdetal.,2002).VRissupposedtobeapriorstep toinvivo exposure(Riva,2009),butitis lesslikelytobe rejectedbythepatient(Olatunji,Cisler,&Deacon,2010).
Regarding the treatment of eating disorders (ED), the most widely-accepted form of psychotherapy, mainly for bulimia nervosa and binge eating disorder, is cognitive-behavioraltherapy(CBT;NIMH,2014).InCBT,patientsare trainedtochange their patternsofthinkingand behaving toprepare them toface their fears.However,in spite of theprogressbeingmade,theseverity,thetendencytoward chronicity, andthecomplications observed inthese disor-ders show that we still donot have any treatments that are completely capable of dealing with their complexity (Wilson,2010;Villarejoetal.,2012).Oneofthemany diffi-cultiesfor patientsliesinstabilizing theireatingpatterns in order to achieve weight regulation and start the cog-nitiveworkabout theimplicationsoffood-relatedbeliefs. TherapeutictoolssuchasVRcomponentsmaybeeffective inoptimizingthesetherapeuticstrategies(Hart,Abraham, Franklin,&Russell,2011).
VR has mainly been applied in the evaluation and treatment of body image disturbances (Cesa et al., 2013; Gutiérrez-Maldonado, Ferrer-García, Caqueo-Urízar, & Moreno,2010;Marco,Perpi˜ná, & Botella,2013;Perpi˜ná etal.,1999;Perpi˜ná,Marco,Botella,&Ba˜nos,2004;Riva, Bacchetta, Baruffi, Rinaldi, & Molinari, 1999; Riva et al., 2000;Riva,2011),withsatisfactoryresultsnotonly inthe
case of body image, but also on psychopathology-related indices.However, recently some studies have shown that exposure to virtual food produces the same sensations as exposure to real food in non-immersive and immer-sive environments (Ferrer-García, Gutiérrez-Maldonado, Caqueo-Urízar,& Moreno, 2009; Ferrer-Garcia, Gutierrez-Maldonado, Treasure, Vilalta-Abella, 2015; Ferrer-Garcia etal., 2014; Gorini, Griez, Petrova,& Riva, 2010).Thus, thenextstepintheuseofVRforthetreatmentofEDwas totest virtual environments(VE) as atherapeutic tool in anotheressentialaspect of thetreatment of ED patients: normalizingeatingpatterns.Avalidatednon-immersive Vir-tualEnvironmentwithavirtualkitchen(Perpi˜náetal.,2013) hasbeen usedin twoclinical cases withpositive results. Inbothcases,onepatientwithanorexianervosa-restrictive typeandanotherwithanorexianervosa-purgativetype,this VEwasusedtoprovidegradedexposuretofearedfoodsas anadd-ontotheirrespectivetreatments(MaudsleyModel of treatment for adults with anorexianervosa and cogni-tive behavioral treatment, respectively). Results showed that both patients normalized their eating patterns and introducedavoidedfoodsintotheirrealdailyintakes.Inthe patientwithanorexianervosa-restrictivetype,theanxiety levelandfearsrelatedtofoodwerereduced,aswerebinges andvomitingintheanorexianervosa-purgativetype. More-over,theirEDsymptomswerereduced,andtheirbodymass indexincreasedsignificantly(Cardi,Krug,Perpi˜ná, Mataix-Cols,Roncero, &Treasure,2011; Perpi˜ná, Ferrero,Carrió, &Roncero,2012).
theeffectsofaVRcomponentasatherapeutictoolto nor-malizeeatingpatterns, aspartofthecognitive-behavioral treatmentforaBNpatient.
Case
illustration
Patientidentification
Bwasa17-year-oldwomanwithabodymassindexof22.2. She was single and living with her parents and an older brother and older sister. B was enrolled in the last year ofhigh school. She wantedtostart universitystudies the followingyear.Shehadamediumsocio-economiclevel.
Reasonfortheconsultation
Baskedfortreatment,butwaspushedbyhermother.She wasnotsureshehadaproblem,butshecomplainedabout herfrequentintrusivethoughtsaboutfood,andshewanted toeliminatethebinges andvomiting.She recognizedthat hereatinghabitswerenothealthy.Shewashaving3-4binges followed byvomiting per week, and she described strong feelingsof guilt,shame anddisgust.She alsohadasense oflosingcontrol.Shewasnotsatisfiedwithherweight,and shewantedtoloseatleast8kginordertoreachaweightof 55kg.Thiswasherobjectivebecauseatthatweight(when she was16 yearsold) she feltnice and proud of herself, ‘‘peopleusetotellmehowniceIlooked’’.Bhadlowinsight aboutthedisorder.
She did not present any physical alterations, except a slight Russell’s sign on her right hand, and there was no swellingoftheparotidglands.Herbloodcountand biochem-icalanalyseswerenormal.Atacognitivelevel,Bcomplained that her thoughts about food did not allow her to con-centrate on other things, but her academic performance was not impaired. The patient presented depression and anxiety symptoms. She spent the day at school and the eveningstudyingathome.Bwasverymotivated toobtain highgrades.Shewantedtoearnamedicaldegreeandwas encouragedbyhermother,whowasanurse.
Historyoftheproblem
Bhasonebrother---6yearsolder,andasister---3yearsolder. Herbrother,sisterandmotherwerealloverweight.When shewas14,shebegantoworryaboutbecomingoverweight likethem. At15 yearsold,Bstarted tofollow restrictive diets,andshelost6kgin6months.Herfamilywouldtell her that she had to eat more because she wasvery thin andlookeddisgusting,butshethoughttheywereenviousof her.Soonshestartedbinging,followedbyvomiting,oncea week,andthebingesandvomitinghadincreasedinnumber to3-4 perweek in theprevious 6months,approximately. Thepatient’smothersoughthelpatthelocalMentalHealth CareUnit.
Assessmentanddiagnosis
Thepatientwasdiagnosedbyherclinicianintheoutpatient mental-healthcenterusingtheStructuredClinicalInterview forDSM-IV-TR.Inasecondsession,Bwasaskedtocomplete
asetofself-reports,listedbelow,atbaselineandafterthe 7 sessions of VR. This study received the approval of the Ethics Committees of the University of Valencia and theoutpatientmental-healthcenter.Beforecompletingthe protocol,thepatientsignedaninformedconsentform.
Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996).Thisself-report evaluates thepresenceand severity of depressive symptoms. It consists of 21 items ratedona4-pointLikertscale(from0to3).Psychometric propertiesoftheSpanishversionareadequate(Cronbach’s alphaof0.89;Sanz,Perdigón,&Vázquez,2003).
BeckAnxietyInventory (BAI; Beck & Steer, 1993).This self-reportevaluatestheseverityofanxietysomatic symp-tomswith21items,usinga4-pointLikertscale(from0to3). Forthepresentstudy,theSpanishversionofComeche,Diaz andVallejo(1995)wasused,whichhasshown satisfactory psychometricproperties(Cronbach’salphaof0.88).
EatingDisordersInventory-II(EDI-II;Garner,1991; Span-ishversion:Corral,González,Pere˜na, & Seisdedos,1998). This inventory consists of 91 items grouped in 11 sub-scalesthatevaluateattitudes,behaviors,andmoregeneral aspects associated with ED: Drive for thinness, bulimia, bodydissatisfaction,ineffectiveness, perfectionism, inter-personaldistrust,interoceptiveawareness,maturityfears, asceticism, impulse regulation and social insecurity. The psychometricpropertiesinSpanishpopulationare satisfac-tory(Cronbach’salpharangefrom0.83to0.92,exceptfor maturityfears=0.65).
Attitudes Toward Change in eating disorders (ACTA; Beato-Fernández&Rodriguez-Cano,2003).Thisself-report evaluates ED patients’attitudes toward change, following the Prochascaand DiClementetrans-theoretical model. It consistsof59items,ratedfrom1‘‘never’’to5‘‘always’’, and grouped in 6 sub-scales: pre-contemplation, contem-plation,decision, action,maintenanceandrelapse.Inthe present study, the last two factors were not included becausetheywerenotrelevanttothepatient’ssituation. The psychometric properties in the original study with a Spanishpopulationaresatisfactory(Cronbach’salpharange from0.74to0.90).
BulimicInvestigatoryTest,Edinburgh(BITE;Henderson& Freeman,1987;Spanishversion:Rivas,Bersabé,&Jiménez, 2004). This 33-item self-report was designed to evaluate bulimicandbinge-eatingsymptoms.Theinstrumenthastwo sub-scales:aseverityscale thatevaluatesthepresenceof symptoms,andaseverityscale thatmeasurestheseverity ofbinges andpurgesbasedonthefrequency.The Spanish validation hasshown satisfactory psychometric properties (Cronbach’salphaforsymptoms:0.96and0.62forseverity). Regardingthemeasurestocontroltheoutcomeofthe vir-tualrealitycomponent,thepatientfilledoutthefollowing questionnaires:
Ad-hoc intra-session questionnaire. During the virtual experience, the patientwas asked, using a Likert format (0:notatall---10:absolutely),abouttheexperienceof vir-tualeatingbeforeandaftereating:emotions(well-being, fear,nervousness,guilt,anddiscomfort),howappetizingit was,hercontrolovertheurgetoeatit,andthedesireto avoidthefood.
extentshehadavoidedfood,andthedegreeofinterference thedisordercausedinherdailyactivities.
At thetimeoftheassessment,BmettheDSM-IV(APA, 2000)criteriafor BulimiaNervosa(BN)purgative subtype. BasedontheDSM-5(2013),shewouldhavemetthecriteria forBNwithmild-moderateseverity.
Treatmentintervention
B received Fairburn’s Cognitive-Behavioral Therapy (CBT) for BN (seeFairburn,Marcus, & Wilson,1993 for detailed description)athercorrespondingnationalhealthoutpatient service. Duetoherlow insightandmotivationtochange, thedecision wasmade toincludeaVRmodulecontaining seven sessions, parallelto PhasesIand II of theCBT ses-sions.ThepurposeofthisfirststageofCBTistonormalize theeatingpattern,andthiswouldalsobethemain objec-tiveoftheVRsessions.IntheVRsessions,thepatientwould practicetheissuesintroducedintheCBTsessionsinorder toregaincontroloverfood,practicehealthyeatinghabits (enjoymeals,alwayseatinthesameplace,etc.),andplan mealsbycontrollingstimulitoavoidbinges.Then,inPhase II, the patient would gradually be exposed to forbidden food,practicealternative behaviors,andreplacenegative thoughtswithpositiveself-instructions.
AtotalofsevenVRsessionswereincludedin this ther-apymodule. The sessionsweredesignedfor patientswith BN,specificallytobeusedwithFairburn’sCBT.Theylasted approximately 60min each, and there was an intervalof one/two weeks between sessions. Sessions had specific objectivesandcontents,describedinTable1.
SoftwareandHardware
Thenon-immersivevirtualenvironmentconsistsofakitchen withtwoareas thatcontainallthenecessary elementsto
cook, drink and eat: countertop, cabinets, stove, fridge, table,andchair(seeFig.1).The foodsarelocatedinthe fridge, cabinets and shelves, and the patient can access themfreelyorblockthemifdesired.Theeatingstylecan besetatfastorslow.Thesizeofcertainfoods(chocolate, potatoes,pizza,etc.)canbeincreased(occupyingtheentire screen)ordecreased(untilvanishing).Alternativebehaviors canbeperformed,suchasmakingaphonecallorlistening tomusic.Inaddition,negativeandpositivethoughtscanbe addressed,andtrainingisgiveninpositiveself-instructions. Asreinforcement,thesoftwareallowsthetherapisttoshow positiveornegativeconsequencesofthedecisionor behav-iorthatthepatienthasjustdisplayed(imageofhappyvs. sadbodyorgans).
TheVEwasdisplayedona3-GHzPentiumVlaptopwith 1GBRAM,a256Mbgraphiccard,a19-in.monitoranda2D mouse.Thepatientwascomfortablyseatedinfrontofthe monitor-screen, located at a distance of 50cm, next to theclinician,andinadimlylitroom.
Results
Throughout the VR sessions, it could be observed that, before eating virtually, the desire to eat was quite high andstableovertheweeks;however,thefearandavoidance decreased,andtheimpulsecontrolincreased(seeTable2). Itisalsonoteworthythatafterthevirtualeating,theurge topurgeandeatandthenegativeconsequencesgradually decreased.Regarding theevaluationof thesenseof pres-ence,duringthesevensessions,thepatientfeltthattheVR experienceseemedrealandsimilartoreality.
Fig.2showstheweeklyinter-sessionevaluations.Inher dailylife,Bmadesignificantprogresswithhereatinghabits, experiencing a gradual decrease in binges, vomiting and foodavoidance.Therewasalso anoteworthy decreasein theinterferencecausedbythedisorder.Bwasveryaware
Table1 Descriptionofsessions.
Sessions Objectivesandactions
Session1 Presentandpracticehealthyeatinghabits:havingfivemealsaday,alwayseatinginthesameplace,
eliminatingdistractionswhileeating,payingattentiontowhatsheeats.Bwasaskedtoeatwhatshewanted, andshechoseachickenbreastwithfriedpotatoesandanapplefordessert.
Session2.Inthissession,wecontinuedto
Session2 Practicethehealthyeatinghabitsfromtheprevioussession,payingspecialattentiontoeatingslowly, andpointingouttheimportanceofplanningmealsandcontrollingstimuliinordertoavoidbingescaused byhungerandemotionaleating.
Session3 EncourageBtogainpowerandcontroloverherself-forbiddenfoods.Inthissession,Bwasaskedtoeata virtuallasagna.Positiveself-instructionsweretaughtandpracticedinordertoreplacenegativethoughts. Session4 Exposureto4squaresofavirtualchocolatebar.Inthissession,alternativebehaviorstothebinge-eating
werepracticedinordertocontrolimpulsiveeating.Shewastaughtaboutthehungermechanismsandthe advisabilityofwaiting5minbeforecontinuingtoeat.
Session5 Dealingwiththeforbiddenfoodsandtalkingabouttheimportanceofintroducingeachfoodintoherreallife inamoderateway.Arankingfromtheleasttothemostforbiddenfoodwasmade,usingallthepossibilities offeredbytheprogram(morethan20meals).
Session6 Practicethepreviouslylearnedself-controlstrategiesinadifficultsituation:Bwastoldthatshewasinan interpersonalsituation(anargumentwithherfriend)thatoftenledhertohaveanepisodeofbingeeating. Session7 Reviewandpracticeallthelessonsandsituationsfromtheprevioussessions,withspecialemphasisonthe
Figure1 Picturesofthevirtualenvironment.(A)Close-upofthetablewhileeatingfood.(B)Aradioandatelephonethatcan beusedasalternativebehaviors.
oftheVRinherday-to-daylife,whichwasdemonstratedby commentssuchas:‘‘EverytimeIeat,IseemyselfintheVR kitcheneatingslowlyandenjoyingeachbite’’;‘‘whenthe thoughtofbingingcomestomymind,Irememberyou(her therapist)intheVRtellingmetotakecontrolofthefood andmakethesizeofthechocolatebarsmallerandsmaller, sothatitlosesitspoweroverme’’.
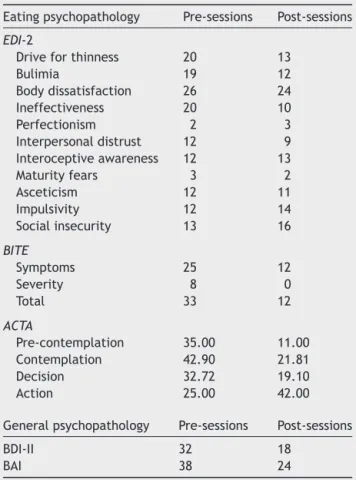
Thecomparisonofthepsychopathologymeasurestaken beforeand after the seven VRsessions showeda general improvement.Therewasanoteworthydecreaseinthedrive for thinness,bulimia, ineffectiveness,andBITE symptoms and severity. Regarding the motivation to change, B was mainlyinthecontemplationandrelapsestagesinthe pre-sessions, and in the action stage at the end of the VR sessions.Thegeneralpsychopathologyalsodecreased(see
Table3).
Discussion
Themainobjectiveofthisstudywastoanalyzetheeffect ofaVRcomponentasatherapeutictooltonormalizeeating
patterns,aspartofthecognitive-behavioraltreatmentfor a BNpatient.Results of thiscase study indicated thatVR had a positive effect on her eating habits. The patient showedareductioninbinges, purgesandfoodavoidance, andmoreimportantly,thedisorder’sinterferenceinherlife alsodecreased.
RegardingtheVRexperience,Bdemonstratedagradual improvementinhercontrolovertheurgetobingeandpurge after virtuallyeatingfood, eventhough the desiretoeat wasstableand high across sessions. Itis noteworthy that thesimilaritytoreallifeandthesenseofrealityfeltbythe patient wasveryhigh from the firstsession on.Her feel-ingofpresenceandtheattributionofrealitywereprobably duetotherelevanceandclinicalsignificanceofthevirtual environmentinherdisorder,makingtheenvironment emo-tionally significant for her. This effect hasbeen observed whencomparingtheVRexposureofclinicalandnon-clinical individuals to relevant virtual environments designed for their disorders (Perpi˜ná, Botella, & Ba˜nos, 2003; Perpi˜ná et al.,2013).In turn, this sense of reality helps patients togeneralizetheVRtreatmenttoreallife(Botellaetal.,
Table2 Datacollectedduringthevirtualsession.
S.1 S.2 S.3 S.4 S.5 S.6 S.7
Beforeeating(0-10)
Desiretoeat 10 9 9 8 8 8 7
Fear 9 10 8 9 7 7 5
Avoidance 10 8 8 7 5 0 6
Impulsecontrol 2 2 0 2 7 8 7
Aftereating(0-10)
Urgetopurge 10 9 7 8 6 2
Urgetoeat 9 9 3 8 5 0
Guilt 10 9 8 6 5 5
Discomfort 9 8 7 7 6 6
Realityoftheexperience(0-10)
Similar 8 8 9 9 8 8 8
Reality 9 8 8 8 9 8 9
S.: session.
0 1 2 3 4 5
S.1 S.2 S.3 S.4 S.5 S.6 S.7
N.º binges
N.º vomits
Food avoidance-meat (0-5) Food avoidance-chocolate (0-5)
Figure2 Dataregardingtheinter-VRsessionevaluations.
2004).Bstated thatthe VRsessionshelpedher tocreate a visual image of herself as successful in controlling the impulsetobingeandvomit.At theendof thesessions, B also introduced more healthy foods that she had avoided
Table3 Eatingandgeneralpsychopathologymeasures pre-andpost-VRsessions.
Eatingpsychopathology Pre-sessions Post-sessions
EDI-2
Driveforthinness 20 13
Bulimia 19 12
Bodydissatisfaction 26 24
Ineffectiveness 20 10
Perfectionism 2 3
Interpersonaldistrust 12 9 Interoceptiveawareness 12 13
Maturityfears 3 2
Asceticism 12 11
Impulsivity 12 14
Socialinsecurity 13 16
BITE
Symptoms 25 12
Severity 8 0
Total 33 12
ACTA
Pre-contemplation 35.00 11.00
Contemplation 42.90 21.81
Decision 32.72 19.10
Action 25.00 42.00
Generalpsychopathology Pre-sessions Post-sessions
BDI-II 32 18
BAI 38 24
EDI-2:EatingDisorderInventory;BITE:ACTA:AttitudesToward Changeineatingdisorders;BDI-II:BeckDepressionInventory-II; BAI:BeckAnxietyInventory.
for years into herreal diet, such asred meat.The most important achievement for her was that she managed to eata pieceof chocolate cake, which scared her because shewas notconfident that she couldcontrol the impulse toeat the entire cake. In fact, in the first VR session, B toldthetherapistthatshewouldnoteatthevirtual choco-latecake.However,asthesessionsprogressed,Bfeltmore confident, making it possible towork withher emotions, thoughtsandfearsinasecureenvironmentat theprecise momentofeatingahighlyfearedfood.Again,VRfunctioned asa previoussteptoreallife,asoccurredwhenusingVR inotherED diagnoses,suchasanorexianervosarestrictive andpurgativesubtypes(Cardietal.,2011;Perpi˜ná etal., 2012).As Pla-Sanjuaneloet al.(2015) stated,by simulat-ingreal-world environmentswhere binging occurs, virtual realityexposuretherapyachievesgreaterecologicalvalidity thaninvivoexposureconductedinthetherapist’soffice.
There was also a noticeable improvement in the ED symptomswhencomparing thepre- andpost-VR sessions, especiallyin the drive for thinness, bulimia,and ineffec-tiveness factors of the EDI-II, and in the severity of the BN measured by the BITE. One of the most remarkable results was the change in the motivational stage of the patientbefore and after the seven VRsessions. The pre-VRevaluationshowedthatBwasmainlyinaContemplation stage,i.e. she began toconsiderthat she hada problem butdidnothavethedeterminationtocorrectit.However, atthepost-VR evaluation,Bwasclearlypositionedinthe Action stage, where the patient experiences a change in threeareas:cognitive,withpositivethoughtsaboutchange; behavioral,withchangesinherhabits;andaffective,where thedisorder is perceived as unpleasant(Beato-Fernández &Rodriguez-Cano,2003).Thisresultdemonstrates--- once again---thepositiveeffectofVRonself-efficacyand motiva-tiontochange(Rivaetal.,1999).Thisisespeciallyrelevant inEDbecausepatients’ambivalencemakesthemreluctant toreceivetreatment,andtheattritionrateisveryhigh.
theuseofaVRcomponentinthegeneraltreatmentfor nor-malizing the ED eatingpattern. As mentioned above,the virtualfoodseemstohave thesameemotional impacton EDpatients.BecauseVRseemscapableofproducing anxi-etyandfood avoidanceandtheawakeningofthe urgeto eat,opportunities arise todesign components to prevent andmanage binging andemotional eatingin ED patients, notonlyforuseintreatments,butalsotoconstructefficient virtuallabsforstudyingeatingbehavior.
In sum,our resultssuggest that the VEwasa relevant andeffectivecomplementtotraditionalCBTtreatmentina BNpatient.However,withoutcontrolgroupsitisnot possi-bletoaffirmtowhatextentthebenefitsareduetotheVR componentortotheCBT.Moreover,wehavenodataabout thefollow-up.Furtherstudies shouldcontinuethisline of researchby usinglargersample sizes withdifferent diag-nosesandcontrolgroups, inordertocomparedifferences inthereactionstoandresultsoftheVRcomponentinthe clinicalsetting,andtheirgeneralizationtoreallife.
Ethical
disclosures
Protection of human and animal subjects.The authors declarethat the proceduresfollowed were in accordance withtheregulationsoftherelevantclinicalresearchethics committeeandwiththoseoftheCodeofEthicsoftheWorld MedicalAssociation(DeclarationofHelsinki).
Confidentialityofdata.Theauthorsdeclarethattheyhave followedthe protocols of theirwork center onthe publi-cation of patient data and that all the patients included inthestudyhavereceivedsufficientinformationandhave giventheirinformedconsentinwritingtoparticipateinthat study.
Righttoprivacyandinformedconsent.Theauthorshave obtainedthe written informed consentof the patients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Conflict
of
interest
Theauthorsdeclarenoconflictofinterest.
Acknowledgements
Supported by the Spanish Ministerio de Sanidad (FIS-PI051937), Conselleria de Sanidad (SMI 3/2008), and Conselleria d’Educació, Cultura i Esport, Generalitat Valenciana(PROMETEO/2013/066).CentrodeInvestigación BiomédicaenRedFisiopatologíadelaObesidadyNutrición, initiativeofISCIII.GobiernodeAragón(dpto.deindustriae innovación).FondoSocialEuropeo.
References
American Psychiatric Association(2000). Diagnostic and statisti-calmanualofmentaldisorders(4thed.rev.).Washington,DC: AmericanPsychiatricAssociation.
Beato-Fernández, L., & Rodriguez-Cano, T. (2003). Attitudes towardschange ineating disorders(ACTA). Developmentand
psychometric properties. Actas Espa˜nolas de Psiquiatría, 31, 111---119.
Beck,A.T.,&Steer,R.A.(1993).ManualfortheBeckDepression Inventory.SanAntonio,TX:ThePsychologicalCorporation. Beck,A.T.,Steer,R.A.,&Brown,G.K.(1996).ManualfortheBeck
DepressionInventory(2nded.).SanAntonio,TX:The Psycholog-icalCorporation.
Botella,C.,Quero,S.,Ba˜nos,R.,Perpi˜ná,C.,GarciaPalacios,A., &Riva,G.(2004).Virtualrealityandpsychotherapy.Studiesin HealthTechnologyandInformatics,99,37---54.
Bush, J. (2008). Viability of virtual reality exposure therapy as a treatment alternative. Computers in Human Behavior, 24, 1032---1040.
Cardi,V., Krug, I., Perpi˜ná, C.,Mataix-Cols, D., Roncero,M., & Treasure,J.(2011).Theuseofanonimmersivevirtualreality programmeinanorexianervosa:Asinglecase-report.European EatingDisordersReview,20,240---245.
Cesa,G.L.,Manzoni,G.M.,Bacchetta,M.,Castelnuovo,G.,Conti, S.,Gaggioli,A.,etal.(2013).Virtualrealityforenhancingthe cognitivebehavioraltreatmentofobesitywithbingeeating dis-order: Randomizedcontrolled studywithone-year follow-up. JournalofMedicalInternetResearch,15,e113.
Comeche,M.I.,Díaz,M.I.,& Vallejo,M.A.(1995). Cuestionar-ios, inventarios y escalas. Ansiedad,depresión yhabilidades sociales.Madrid:UNED,FundaciónUniversidad-Empresa. Corral, S., González, M., Pere˜na, J., & Seisdedos, N. (1998).
Adaptación espa˜nola del Inventario de trastornos de la con-ductaalimentaria.InD.M.Garner(Ed.),EDI-2:inventariode trastornos de la conducta alimentaria. Manual (pp. 69---80). Madrid:TEA.
Fairburn,C.,Marcus,M.,&Wilson,G.(1993).Cognitive-behavioral therapyforbingeeatingandbulimianervosa:Acomprehensive treatmentmanual.InFairburn,&Wilson(Eds.),Bingeeating: Nature, assessment, and treatment. New York:The Guillford Press.
Ferrer-García,M.,Gutiérrez-Maldonado,J.,Caqueo-Urízar,A.,& Moreno,E.(2009).Thevalidityofvirtualenvironmentsfor elic-itingemotionalresponsesinpatientswitheatingdisordersand incontrols.BehaviorModification,33,830---854.
Ferrer-Garcia,M.,Gutierrez-Maldonado,J.,Treasure,J.,& Vilalta-Abella,F.(2015).Cravingforfoodinvirtualrealityscenariosin non-clinicalsample:Analysisofitsrelationshipwithbodymass indexandeatingdisordersymptoms.EuropeanEatingDisorder Review,23,371---378.
Ferrer-Garcia, M., Gutiérrez-Maldonado, J., Pla, J., Riva, G., Andreu-Gracia,A.,Dakanalis,A.,etal.(2014).Developmentof a VRapplicationforbinge eatingtreatment:Identification of contextsandcuesrelatedtobingeingbehaviorinSpanish Ital-ianpatients.StudiesinHealthTechnologyandInformatics,199, 71---75.
Garner,D.M.(1991).EatingDisordersInventory-2.Odessa,FL: Psy-chologicalAssessmentResourcesInc.
Gorini,A.,Griez,E.,Petrova,A.,&Riva,G.(2010).Assessmentof theemotionalresponsesproducedbyexposuretorealfood, vir-tualfoodandphotographsoffoodinpatientsaffectedbyeating disorders.AnnalsofGeneralPsychiatry,9,1---30.
Gutiérrez-Maldonado,J.,Ferrer-García,M.,Caqueo-Urízar,A.,& Moreno,E.(2010).Bodyimageineatingdisorders:Theinfluence ofexposure to virtual-realityenvironments. Cyberpsychology, Behavior,andSocialNetworking,13,521---531.
Hart,S.,Abraham,S.,Franklin,R.,&Russell,J. (2011).Weight changes during inpatient refeeding of underweight eating disorder patients. European Eating Disorders Review, 19, 390---397.
Henderson, M., & Freeman, C.P. (1987). Aself-rating scale for bulimia.The‘BITE’.BritishJournalofPsychiatry,150,18---24. Marco, J.H.,Perpi˜ná, C.,& Botella,C.(2013). Effectivenessof
treatmentofbodyimageineatingdisorders:Oneyearfollow-up. PsychiatryResearch,30,619---625.
National Institute of Mental Health (NIMH). (2014). Eating dis-orders. In Eating disorders: About more than food (No. 11-4901).Availableat:www.nimh.nih.gov/health/publications/ eating-disorders/eating-disorders.pdf
Olatunji,B.O.,Cisler,J.,&Deacon,B.J.(2010).Efficacyof cog-nitive behavioral therapy for anxiety disorders: A review of meta-analyticfindings.PsychiatricClinicsofNorthAmerica,33, 557---577.
Perpi˜ná,C.,Botella,C.,&Ba˜nos,R.M.(2003).Virtualrealityin eat-ingdisorders.EuropeanEatingDisordersReview,11,261---278. Perpi˜ná,C.,Ferrero,A.,Carrió,C.,&Roncero,M.(2012).
Normal-izationoftheeatingpatternsinapatientwithanorexianervosa, purgativesubtype,withthesupportofavirtualenvironment.A casestudy.AnnuaryofClinicalandHealthPsychology,8,23---30. Perpi˜ná, C.,Botella,C., Ba˜nos,R.,Marco,J. H.,Alca˜niz, M.,& Quero,S.(1999).Bodyimageandvirtualrealityineating dis-orders:Exposurebyvirtualrealityis moreeffective thanthe classicalbodyimagetreatment?CyberPsychology&Behaviour, 2,149---159.
Perpi˜ná, C., Marco, J. H., Botella, C., & Ba˜nos, R. M. (2004). Tratamientodelaimagencorporalenlostrastornos alimenta-riosmediantetratamientocognitivo-comportamentalapoyado conrealidadvirtual:resultadosala˜nodeseguimiento.Psicología conductual,12,519---537.
Perpi˜ná,C.,Roncero,M.,Fernández-Aranda,F.,Jiménez-Murcia,S., Forcano,L.,&Sánchez,I.(2013).Clinicalvalidationofavirtual environmentfornormalizingeatingpatternsineatingdisorders. ComprehensivePsychiatry,54,680---686.
Pla-Sanjuanelo, J., Ferrer-García, M., Gutiérrez-Maldonado, J., Riva,G.,Andreu-Gracia,A.,Dakanalis,A.,etal.(2015). Identi-fyingspecificcuesandcontextsrelatedtobingeingbehaviorfor thedevelopmentofeffectivevirtualenvironments.Appetite, 87,81---89.
Riva,G. (2009). Virtualreality: An experientialtool for clinical psychology. British Journal of Guidanceand Counselling, 37, 337---345.
Riva,G.(2011).Thekeytounlockingthevirtualbody:Virtual real-ityinthetreatmentofobesityandeatingdisorders.Journalof DiabetesScienceandTechnology,5,283---292.
Riva,G., Bacchetta, M., Baruffi, M., Rinaldi, S., & Molinari, E. (1999). Virtualreality basedexperientialcognitive treatment ofanorexianervosa.JournalofBehaviouralTherapyand Exper-imentalPsychiatry,30,221---230.
Riva, G., Bacchetta, M., Baruffi, M., Rinaldi, S., Vincelli, F., & Molinari,E.(2000).Virtualreality-basedexperientialcognitive treatmentofobesityand binge-eatingdisorders.Clinical Psy-chology&Psychotherapy,7,209---219.
Rivas,T.,Bersabé,R.,&Jiménez,M.(2004).Fiabilidadyvalidez deltestdeinvestigaciónbulímicadeedimburgo(BITE)enuna muestradeadolescentesespa˜noles.PsicologíaConductual,12, 447---461.
Sanz, J., Perdigón, A. L., & Vázquez, C. (2003). Adaptación Espa˜noladelInventario parala Depresiónde BeckII (BDI-II). Propiedadespsicométricasenpoblacióngeneral.ClínicaySalud, 14,249---280.
Villarejo, C., Fernández-Aranda, F., Jiménez-Murcia, S., Pe˜ nas-Lledó,E.,Granero,R.,Penelo,E.,etal.(2012).Lifetimeobesity inpatientswitheatingdisorders:Increasingprevalence,clinical andpersonalitycorrelates.EuropeanEatingDisordersReview, 20,250---254.
Wiederhold,B.K.,Jang,D.P.,Gevirtz, R.G.,Kim,S.I.,Kim,I. Y.,& Wiederhold,M.D.(2002). Thetreatmentoffearof fly-ing: Acontrolled studyof imaginaland virtualrealitygraded exposuretherapy[electronicversion].InformationTechnology inBiomedicine,IEEETransactions,6,218---223.