www.elsevier.es/rmuanl
EXPERT’S
CORNER:
A
PERSONAL
APPROACH
How
I
diagnose
and
treat
lupus
D.Á.
Galarza-Delgado
∗,
A.C.
Arana-Guajardo
ServiciodeReumatología,DepartamentodeMedicinaInternadelHospitalUniversitario,‘‘Dr.JoséEleuterioGonzález’’,dela UniversidadAutónomadeNuevoLeón,Monterrey,NL,Mexico
Received15October2014;accepted4November2014 Availableonline6February2015
Introduction
Systemic Lupus Erythematosus (SLE) is a multisystemic autoimmunedisease ofunknown originwitha waxingand waningcourseandasignificantmorbi-mortality.The objec-tive of this paper is to provide an SLE overview, aswell as recommendations regarding diagnosis and therapeutic concepts. In the first stage of the disease, the combina-tionofgenetic,genderandenvironmentalfactorsculminate inthe formationof autoantibodies yearsbeforetheonset of symptoms is observed. In the second phase,there are clinicalmanifestationsandassociationswithcomorbidities. ManagementofpatientswithSLEshouldbepredictive, pre-ventive,personalized,andparticipatoryinordertoachieve remission and prevent relapses. We can divide SLE into threecategories according totheseverityof the disease: mild,moderate,andsevere.Corticosteroidsarethe main-stayoftherapy,buttheuseofanotheragentismandatoryin ordertoreducesideeffects.Someofthebiologicalagents
∗Correspondingauthorat:ServiciodeReumatologíadel
Depar-tamentodeMedicinaInternadelHospitalUniversitario,‘‘Dr.José EleuterioGonzález’’,delaUANL,Av.MaderoyAv.Gonzalitoss/n, col.MitrasCentro,CP64460Monterrey,NL,Mexico.
Tel.:+528183337798.
E-mailaddress:[email protected] (D.Á.Galarza-Delgado).
usedinimmunosuppressivetherapyinSLEtreatmentinclude methotrexate,antimalarials, azathioprine,mycophenolate mofetil,cyclophosphamide,belimumabandrituximab.
Background
DiagnosingSystemicLupusErythematosus(SLE)hasbeena challengeover the years.The firstreports of the disease only considered skin manifestations. Later, William Osler recognizedthe systemicinvolvement of the disease.1 SLE
isamultisystemicautoimmunediseaseofunknownorigin.2
SLEhasanincidenceof1---10per100,000person-yearsand aprevalenceof20---70per100,000inhabitants.3SLE
preva-lenceinHispanicsis138.7---244.5per100,000people.4For
every9---10womenwithSLE,1malewillbeaffected.2SLE
hasa waxingandwaning coursewithsignificant morbidity thatcanbefatal---ifnottreatedearly---insomepatients. AdiagnosisofSLEshouldbeconsideredwhenapatienthas characteristicfeaturesofSLEassociatedwithautoantibody formation5; thus, the presence of anti-nuclear antibodies
(ANA)isconsiderednecessaryforanSLEdiagnosis.Patients withoutANAwillhavelessthana3%probabilityof develop-ingthedisease.
Theobjectivesofthispaperaretoprovideanoverview basedontheliteratureandonthepersonalexperienceof 30yearsoftreatingpatientswithSLE,providegeneraland specific recommendations regarding the diagnosis of this challenging disease, and share therapeutic concepts that
http://dx.doi.org/10.1016/j.rmu.2014.11.001
60 D.Á.Galarza-Delgado,A.C.Arana-Guajardo
Susceptibility: Genetic Gender Environmental
Autoantibodies
Latent lupus
Incomplete lupus
Preclinical phase Clinical phase
Trigger
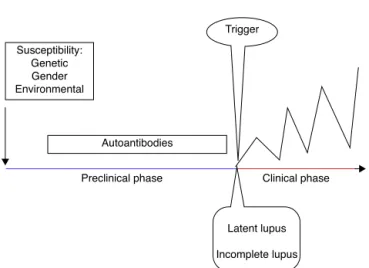
Figure1 Proposedcurrentstagesfordevelopingclinical man-ifestationsofSystemicLupusErythematosus.
arefundamentalforthecomprehensivemanagementofthe disease.
SLE
stages
SLEstagesincludeapreclinicalandaclinicalphase,aswell asitsrelatedcomorbidities.
Clinicalmanifestationsonlydevelopinpredisposed indi-viduals and are secondary to a loss of tolerance with a subsequent immune dysregulation6 (Fig. 1). The
develop-ment of autoimmunity is determined by genetic, gender, andenvironmentalfactors.Advancesingenetictechniques haveidentifiedmorethan30geneticassociationswithSLE including variants of HLA and Fc␥ receptor genes, IRF5,
STAT4,PTPN22,TNFAIP3,BLK,BANK1,TNFSF4andITGAM.7
Moreover, the genetic contribution to the development of SLE has been observed in twins, with a concordance between monozygotic twins of 24---56% vs 2---5% in dizy-gotic twins.8 Female preponderance in the pathogenesis
of SLE has been demonstratedin transgenic mice. Smith-Bouvieretal.observedthatmicewiththeXXchromosome weremoresusceptibletodevelopinglupuswhencompared toXY mice.9 Environmental factorscan contribute tothe
developmentofSLEbytheinhibitionofDNAmethylation.10
Thesefactorsincludedrugs(e.g.procainamide),diet, smok-ing,UVlightexposureandinfections(Epstein---Barrvirus).11
Finally,thereisapathogenicautoantibodyproductioninSLE patients,reflectinglossoftolerance.6
Different authors have described the development of autoantibodies before the clinical onset of the disease in the past. Arbuckle et al. described the presence of at least one SLE autoantibody before the diagnosis (up to 9.4 years earlier; mean, 3.3 years) in asymptomatic patients.Antinuclear,antiphospholipid,anti-Roandanti-La antibodiesprecededtheotherautoantibodiesinthiscohort of patients.12 Subsequently, McClain et al. described the
clinicalsignificanceofthepresenceofantiphospholipid anti-bodiespriortoanSLEdiagnosis,aswellasthepresenceof theseautoantibodiesinpatientswithamoresevereclinical outcome.13
Inordertoclassifypatientsintheearlystagesofthe dis-ease,differentauthorshaveproposeddefinitionsaccording
Table1 GeneralrecommendationsforSLE*patients.
Balanceddietandexercise
Avoidsubstancesanddrugsthatmightinducelupus Nosmoking
Vaccinationschedule
Assessmentofcardiovascularriskfactors Screeningofcancer
Evaluationofreproductivehealth Assessmentofcognitivefunction
* Systemiclupuserythematosus.
tothesymptomsandthepresenceofclassificationcriteria. First, theterm undifferentiatedconnectivetissue disease (UCTD)is usedinindividuals withadisease manifestation suggestive but not diagnosticof a specific connective tis-suedisease.UCTDaccountsfor10---20%ofreferredpatients, 10---15%willfulfilltheclassificationcriteriaforSLE5years later.14 Factors that predict evolution to SLE are young
age,alopecia,serositis,discoidlupus,apositiveanti-human globulin(Coombs)testandanti-Smoranti-DNAantibodies.15
Ganczarczyketal.describedtheterm‘‘latentlupus’’to definepatientswithfeaturesconsistentwithSLEwhichmay ormaynotbeapartoftheAmericanCollegeof Rheumato-logy(ACR)classificationcriteria,butstillare≤4.16
Incompletelupusreferstopatients withless thanfour ACRclassificationcriteriaforSLE.Swaaketal.ina multicen-tricstudy,observedthatonlythreeof122incompletelupus patientsdevelopedSLEduring3yearsoffollow-up,and sug-gestedthat incompleteSLEforms asubgroup withagood prognosis.17 Later,Greeretal.confirmedthisobservation.
Theyfollowed38incompletelupuspatientsover19months andonlytwodevelopedSLE.18Anadditionaltermis
preclin-icallupus,whichdefinesindividualswithincreasedgenetic riskforthedevelopmentofSLEbutnoclinicalsymptoms.19
Afterthepreclinicalstage,theclinicalstageoccurswith the onset of symptoms. The GLADEL (Grupo Latinoameri-canodeEstudiodeLupus)cohort,amultinationalinception prospectivecohortinLatinAmericancenters,describedthe symptomsin1214patientswithSLE.Theyfoundthat arthral-gia and/or arthritis, fever, photosensitivity, alopecia and malarrashwerethemostcommonsymptomsatonset.20
SLE
treatment
SLEmanagementrepresentsthe‘‘P4’’,anewparadigmof modern medicine.P4Medicine stands for Predictive, Pre-ventive,PersonalizedandParticipatoryMedicine.
SLE is a syndrome with high variability in the disease course as well as in the severity of the manifestations; thereforeeachSLEpatientshouldbetreatedonan individ-ualized basisinordertoimplementapropertreatment.21
Thegoalofthetreatmentistoachieveremission,prevent flares and use of drugs with the minimum dose required topreventlong-termsideeffects.The treatmentincludes lifestyle modification,patienteducation, physical activity andmedicalor(insomecases)surgicalintervention.
avoid Echinacea, melatonin, garlic, and alfalfa sprouts, whichhavebeendescribedtoprecipitatetheircondition.22
It is also important to inform patients to avoid disease reactivationdrugssuchasprocainamide,hydralazine, sul-fonamides,anti-TNFa, ibuprofen or estrogen.23,24 Smoking
alsoappearstoinfluence theonsetandcourseof the dis-ease among patients with SLE.25,26 The effect of drugs
likemethotrexate(MTX)andhydroxychloroquine(HCQ)may diminishwithsmoking.
ThevaccinationscheduleinSLEpatientsincludesayearly influenzavaccineandapneumococcalvaccineevery5years. Hepatitis Band Tetanus toxoid vaccinations also seem to besafe,andnotassociatedwithflares.27 Thequadrivalent
human papillomavirus vaccine is also safe and not asso-ciated with increased lupus activity.28 It is important to
considerthatinactivatedlivevaccinesarecontraindicated in patientstaking immunosuppressive drugs and/or gluco-corticoidsatadose>20mg/day.27
Most SLE patients are diagnosed in the reproductive years,thusreproductivehealthis animportantissue.Itis recommendedforSLEpatientstohave aninactivedisease forasixmonthperiodpriortoconception.Therearethree main types of contraceptives: barrier methods, intrauter-inedevicesandthehormonalmethod.Hormonalmethods include combinedor progestin-only. The use of combined methodsisassociatedwithanincreasedriskofSLE,29
how-ever,progesteronemethodshaveproventobesafeforSLE patients.30
In addition tothe control of the disease, SLE patients shouldhaveasystematicassessmentofcomorbidities.SLE patients develop prematureatherosclerosis and their risk of heart attack and stroke is 10 times higher than that of age-matched controls.31 Atherosclerosis is the result
of the complex interplay between dysfunctional immune regulation,inflammation,traditionalriskfactors,aberrant endothelialcellfunctionandrepair,andthetherapeuticsfor treatingtheunderlyingautoimmunedisease.32SLEpatients
alsohaveanincreasedriskofdifferenttypesofcancersuch asnon-Hodgkinlymphoma,lungcancer,andcervical dyspla-sia.Lupusdiseaseactivity,smokingandimmunosuppressive drug exposure are some of the causes of the increase in cancerrisk.33Therefore,SLEpatientsshouldhave
colonos-copies,Papsmear,andmammogramschedules.
Cognitive dysfunction prevalence in SLE ranges from 12% to 87%. Petri et al. compared cognitive functioning inrecentlydiagnosedSLE patientsversusnormalcontrols. Using Automated Neuropsychological Assessment Metrics (ANAM), SLE patients performed significantly worse than normalcontrols.Therefore,acognitiveassessmentis nec-essaryinallSLEpatientsfromtheonsetofthedisease.
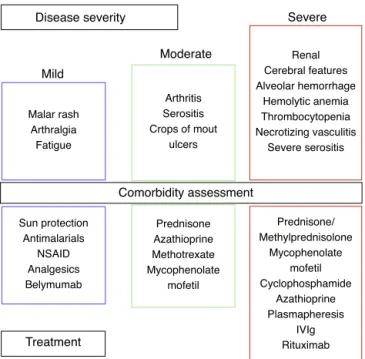
WecandivideSLEintothreecategoriesbasedondisease severity:mild,moderate,andsevere(Fig.2).
Corticosteroids (CS) are the mainstay of treatment for SLE in any category, with proven efficacy.34 The
dose varies according to the severity of symptoms. A low dose is 0.1---0.2mg/kg/day, an intermediate dose is 0.3---0.5mg/kg/day,andahighdoseis0.6---2mg/kg/day.The useofthisdrugisassociatedwithanincreaseinserumlipids, bloodpressure,weightandglucose,inadditiontocataracts andosteoporoticfractures.Theadverse sideeffectsofCS depend on both the current and the cumulative dosage. Thamer etal. demonstratedthe hazardratio for accrued
Disease severity
Mild
Malar rash Arthralgia
Fatigue
Sun protection Antimalarials
NSAID Analgesics Belymumab
Prednisone Azathioprine Methotrexate Mycophenolate
mofetil
Prednisone/ Methylprednisolone
Mycophenolate mofetil Cyclophosphamide
Azathioprine Plasmapheresis
IVIg Rituximab Arthritis
Serositis Crops of mout
ulcers
Renal Cerebral features Alveolar hemorrhage
Hemolytic anemia Thrombocytopenia Necrotizing vasculitis
Severe serositis
Moderate
Comorbidity assessment
Treatment
Severe
Figure 2 Stepwise approach in the treatment of SLE. NSAID,Nonsteroidalantiinflammatorydrugs;IVIg,intravenous immunoglobulin;SLE,systemiclupuserythematosus.
organdamagetobe1.5,1.64and2.51withprednisonedoses of 6mg/day, 12mg/day and >18mg/day, respectively.35 It
is important to note that SLE diagnosis is not equivalent tothe useof methylprednisolone,andthatin manycases the deleterious effects of CS may outweigh the benefits. Therefore,thegoalistheuseofCSaccordingtotheclinical manifestationsandslowtaperingto1---2mg/day.Inorderto reduceCSdosesandsideeffects,theuseofanotheragent ismandatory.34
MildSLEincludesmucocutaneouslesions,arthralgiasand fatigue.Sun protectionconsists of avoiding whenthe sun is at its highest (10am to 4pm) and patients should use agentswithasunprotectionfactorofat least50,applied 20---30minpriortoexposure,andreappliedevery4h.Topical therapiesdependonwhetheritisalocalizedorwidespread skindisease.Therapiesincludesteroidsand/or calcineurin inhibitors.36Systemictherapiesincludeantimalarialagents,
MTX,azathioprine,mycophenolatemofetil(MMF),dapsone, and cyclophosphamide (CYC), and are used in refrac-tory diseases or in poor responses to treatment.34,36 For
cutaneovascularmanifestations(Raynaudsyndrome,livedo reticularis,etc.) theuse ofcold-preventivemeasures and calcium channel blockers can be beneficial. Nonsteroidal antiinflammatorydrugs (NSAID)canbeusedinheadaches, myalgias, arthralgias, and serositis. NSAID use must be monitored;sideeffectscouldberenal,gastrointestinalor cardiovascular.In myexperience,I have seen severe sec-ondarysideeffectssuchasasepticmeningitis.Ibuprofenis thedrugmostfrequentlyinvolvedinasepticmeningitis,but sulindacandnaproxenhavealsobeendescribed.37
62 D.Á.Galarza-Delgado,A.C.Arana-Guajardo
responds to NSAID and CS. Belimumab is a fully human-ized IgG1 mAb that binds to soluble BLyS (B lymphocyte stimulator),inhibiting itsactivity.21 BLISS-52 andBLISS 76
demonstratedsignificantclinicalresponseswithBelimumab comparedtoplacebosinpatientswithmildandmoderate diseaseactivity(withoutnephritis/CNS).39,40
The severe SLE stage includes hemolytic anemia, thrombocytopenia,diffuse alveolar hemorrhage, necrotiz-ingvasculitis,neuropsychiatriclupusandrenalinvolvement. In this stage, CS is used in high doses and intravenous methylprednisolone pulses for severe cases. In hemolytic anemia and thrombocytopenia the treatment includes CS anddanazol,Rituximab,intravenousimmunoglobulin(IVIg), MMF,CYC,plasmapheresisand/or splenectomy for refrac-tory cases.41 The use of CYC and high doses of CS are
alsoemployedfordiffusealveolarhemorrhage,and plasma-pheresis for refractory cases.We made an observational, retrospectivestudythatincludedtwelveSLEpatientswith alveolar hemorrhage. We found that simultaneous treat-mentwithCS,CYC,plasmapheresisandIVIgwasassociated with a mortality of 17%, contrary to the rate previously describedofupto70---90%.42
According tothe recommendations, glucocorticoid and immunosuppressive therapy is indicated for severe neu-ropsychiatric manifestations (myelopathy, optic neuritis, etc.).AnticoagulationtherapyisindicatedfortheSNC man-ifestationsofantiphospholipidsyndrome.43Inourpractice,
wehavealsoobservedthatthecombinationof methylpred-nisolone,CYC,IVIgandRituximabwaseffectiveforpsychosis refractorytoconventionaltreatment.
Renal involvement is considered the most important prognostic factor. The Task Force Panel for screening, treatment, and management of Lupus Nephritis (LN) rec-ommendedthe treatment to be basedon the type of LN accordingtotheISN/RPScriteria.44Thetreatmentconsists
of the use of corticosteroids either solely or in combina-tionwithimmunosuppressiveagents.Therecommendations for LN treatment include an induction and a maintaining therapy. There are 2 regimens for Class III/IV LN, low-dose ‘‘Euro-Lupus’’ CYC and high-dose CYC followed by maintenancetreatmentwithMMForazathioprine.45 Inour
practice,webelievethatalow-doseCYCismorebeneficial topatientsdecreasing adverse effects,suchasinfections, gonadal toxicity and increased risk of cancer. We do not sharetheideathatmethylprednisolonepulseswillprovide agreaterbenefitthanprednisone.Andfinally,LNresponse shouldbeevaluated3---6monthsafterinitiatingtreatment. In conclusion, SLE is a challenging diseaseto diagnose andtreat. Advancesin research have allowedus toknow whichindividualsareatriskofdevelopingthedisease.Each patientshouldbetreatedonanindividualizedbasis accord-ingtotheirclinicalmanifestationsinordertoprovideproper treatment.
Funding
Nofinancialsupportwasprovided.
Conflict
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.WallaceDJ,HahnBH.Duboislupuserythematosus.7thed. Lip-pincottWilliams&Wilkins;2007.
2.O’NeillS,CerveraR.Systemiclupuserythematosus.BestPract ResClinRheumatol.2010;24:841---51.
3.Pons-EstelGJ,AlarcónGS,ScofieldL,etal.Understandingthe epidemiologyandprogressionofsystemiclupuserythematosus. SeminArthritisRheum.2010;39:257---68.
4.Atisha-FregosoY,Jakez-OcampoJ,LlorenteL.Systemiclupus erythematosusinHispanics.Autoimmunity.2011;44:555---61. 5.SmithPP,GordonC.Systemiclupuserythematosus:clinical
pre-sentations.AutoimmunRev.2010;10:43---5.
6.ChoiJ,KimST,CraftJ.Thepathogenesisofsystemiclupus ery-thematosus---anupdate.CurrOpinImmunol.2012;24:651---7. 7.Deng Y, Tsao BP. Genetic susceptibility to systemic lupus
erythematosus in the genomic era. Nat Rev Rheumatol. 2010;6:683---92.
8.DeapenD,EscalanteA, WeinribL, et al. Arevised estimate oftwinconcordanceinsystemiclupuserythematosus.Arthritis Rheumatol.1992;35:311---8.
9.Smith-BouvierDL,DivekarAA,SadidharM,etal.Aroleforsex chromosomecomplementin the femalebias in autoimmune disease.JExpMed.2008;12:1099---108.
10.Tsokos GS. Systemic lupus erythematosus. N Engl J Med. 2011;365:2110---21.
11.Somers EC, Richardson BC. Environmental exposures, epige-neticchangesandtheriskoflupus.Lupus.2014;23:568---76. 12.ArbuckleMR,McClainMT, RubertoneMV,et al.Development
ofautoantibodiesbefore theclinicalonsetofsystemic lupus erythematosus.NEnglJMed.2003;16:1526---33.
13.McClainMT,ArbuckleMR,HeinlenLD,et al.Theprevalence, onset, and clinical significance of antiphospholipid antibod-iespriortodiagnosisofsystemiclupuserythematosus.Arthritis Rheumatol.2004;50:1226---32.
14.BertsiasGK,SalmonJE,BoumpasDT.Therapeuticopportunities insystemiclupuserythematosus:stateoftheartandprospects forthenewdecade.AnnRheumDis.2010;69:1603---11. 15.Calvo-Alen J, Alarcon GS, Burgard SL, et al. Systemic lupus
erythematosus:predictors of its occurrenceamong a cohort ofpatientswithearlyundifferentiatedconnective tissue dis-ease:multivariateanalysesandidentificationofriskfactors.J Rheumatol.1996;23:469---75.
16.Ganczarczyk L, Urowitz MB, Gladman DD. Latent lupus. J Rheumatol.1989;16:475---8.
17.SwaakAJ,vandeBrinkH,SmeenkRJ,etal.Incompletelupus erythematosus:resultsofamulticentrestudyunderthe supervi-sionoftheEULARStandingCommitteeonInternationalClinical Studies Including Therapeutic Trials (ESCISIT). Rheumatology (Oxford).2001;40:89---94.
18.Greer JM,PanushRS. Incomplete lupuserythematosus. Arch InternMed.1989;149:2473---6.
19.Deane KD, El-Gabalawy H. Pathogenesis and prevention of rheumatic disease:focus onpreclinical RAand SLE.NatRev Rheumatol.2014;10:212---28.
20.Pons-EstelBA,CatoggioLJ,CardielMH,etal.TheGLADEL multi-nationalLatinAmericanprospectiveinceptioncohortof1214 patientswith systemiclupus erythematosus: ethnicand dis-easeheterogeneityamong‘‘Hispanics’’.Medicine(Baltimore). 2004;83:1---17.
21.Sthoeger Z, Sharabi A, Mozes E. Novel approaches to the development of targeted therapeutic agents for systemic lupus erythematosus. J Autoimmun. 2014, http://dx.doi.org/10.1016/j.jaut.201406.002[Epubaheadof print].
23.SkaerTL. Medication-inducedsystemic lupus erythematosus. ClinTher.1992;14:496---506.
24.XiaoX,Chang C.Diagnosisandclassificationofdrug-induced autoimmunity(DIA).JAutoimmun.2014;48:66---72.
25.Ekblom-KullbergS, KautianienH, Alha P,et al. Smokingand the risk of systemic lupus erythematosus. Clin Rheumatol. 2013;32:1219---22.
26.Bourré-TessierJ,PeschkenCA,BernatskyS,etal.Associationof smokingwithcutaneousmanifestationsinsystemiclupus ery-thematosus.ArthritisCareRes(Hoboken).2013;65:1275---80. 27.MoscaM,Tani C,AringerM,et al. EuropeanLeague Against
Rheumatism recommendations for monitoring patients with systemiclupuserythematosusinclinicalpracticeandin obser-vationalstudies.AnnRheumDis.2010;69:1269---74.
28.MokCC,HoLY,FongLS,et al.Immunogenicityandsafetyof aquadrivalenthumanpapillomavirusvaccineinpatientswith systemiclupuserythematosus:acase-controlstudy.AnnRheum Dis.2013;72:659---64.
29.BernierMO,MikaeloffY,HudsonM,etal.Combinedoral con-traceptiveuseandtheriskofsystemiclupuserythematosus. ArthritisRheum.2009;61:476---81.
30.AndreoliL,FrediM,NalliC,etal.Pregnancyimplicationsfor sys-temiclupuserythematosusandtheantiphospholipidsyndrome. JAutoimmun.2012;38:J197---208.
31.AskanaseA,ShumK,MitnickH.Systemiclupuserythematosus: anoverview.SocWorkHealthCare.2012;51:576---86.
32.SkaggsBJ,HahnBH,McMahonM.Acceleratedatherosclerosis inpatientswithSLE---mechanismsandmanagement.NatRev Rheumatol.2012;14:214---23.
33.BernatskyS,KaleM,Ramsey-GoldmanR,etal.Systemiclupus andmalignancies.CurrOpinRheumatol.2012;24:177---81. 34.Lateef A, Petri M. Unmet medical needs in systemic lupus
erythematosus. Arthritis Res Ther. 2012;14 Suppl. 4:S4, http://dx.doi.org/10.1186/ar3919[Epub18.12.12].
35.ThamerM,HernanMA,ZhangY,etal.Prednisone,lupusactivity, andpermanentorgandamage.JRheumatol.2009;36:560---4.
36.Okon LG, Werth VP. Cutaneous lupus erythematosus: diag-nosis and treatment. Best Pract Res Clin Rheumatol. 2013;27:391---404.
37.MorisG,Garcia-MoncoJC.Thechallengeofdrug-induced asep-ticmeningitis.ArchInternMed.1999;159:1185---94.
38.BallEM,BellAL.Lupusarthritis---dowehaveaclinicallyuseful classification?Rheumatology(Oxford).2012;51:771---9. 39.Navarra SV, Guzman RM, Gallacher AE, et al. Efficacy and
safetyofbelimumabinpatientswithactivesystemiclupus ery-thematosus:arandomised,placebo-controlled,phase3trial. Lancet.2011;377:721---31.
40.Furie R, Petri M, Zamani O, et al. A phase III, random-ized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients withsystemiclupuserythematosus.ArthritisRheum.2011;63: 3918---30.
41.Newman K, Owlia MB, El-Hemaidi I, et al. Management of immunecytopeniasinpatientswithsystemiclupus erythemato-sus---oldandnew.AutoimmunRev.2013;12:784---91.
42.Sauceda-DuránAY,Pérez-BarbosaL,Galarza-DelgadoDA,etal. Hemorragia Aleolar en pacientes con enfermedades autoin-munes.Revisióndeunaseriede15casos.Reumatologíaclínica. 2006;2:65.
43.BertsiasGK,IoannidisJP,AringerM,etal.EULAR recommen-dationsforthemanagementofsystemiclupuserythematosus withneuropsychiatricmanifestations:reportofataskforceof theEULARstandingcommitteeforclinicalaffairs.AnnRheum Dis.2010;69:2074---82.
44.WeeningJJ,D´AgatiVD,SchwartzMM,etal.Theclassificationof glomerulonephritisinsystemiclupuserythematosusrevisited. KidneyInt.2004;65:521---30.