PERMANYER www.permanyer.com
ORIGINAL ARTICLE Rev Inves Clin. 2015;67:304-12
Thalidomide and Dexamethasone
Induction Therapy Until Best Response
in Recently Diagnosed Patients
with Multiple Myeloma:
Results From a Pilot Study
Lauro Fabián Amador-Medina
1, Dennis Lacayo-Leñero
2, Erick Crespo-Solís
2, Álvaro Aguayo
2and Déborah Martínez-Baños
2*
1Hospital Regional Alta Especialidad Bajío, León, Gto. México; 2Department of Hematology and Oncology. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
Corresponding author:
*Déborah Martínez-Baños Multiple Myeloma Clinic
Department of Hematology and Oncology
Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán
Vasco de Quiroga, 15
Col. Belisario Domínguez Sección XVI, Del. Tlalpan C.P. 14080, México, D.F., México
E-mail: [email protected] Received for publication: 10-07-2015 Accepted for publication: 24-09-2015
ABSTRACT
Background: Novel therapies for multiple myeloma are not affordable for all healthcare systems. Objectives: The objectives of
this study were to evaluate the response rates, overall survival, event-free survival, and toxicity of thalidomide and dexamethasone administered until best response in recently diagnosed patients with multiple myeloma. Methods: All recently diagnosed
multiple myeloma patients meeting the inclusion criteria received the same treatment with thalidomide and dexamethasone.
Results: We studied 28 patients. Overall response rate was 75%. Complete response, partial response, and very good partial
response were 25.0, 32.1, and 17.9%, respectively. The most frequent adverse event related to therapy was neuropathy. Median overall survival was 66 months, and median event-free survival was 39 months (range, 27.6-50.4). Variables that negatively affected overall survival on multivariate analysis included the presence of extramedullary disease, t(14;16), and chromosome 13 deletion. Conclusions: Induction therapy with thalidomide and dexamethasone until obtaining the best
response in patients with recently diagnosed multiple myeloma was a useful and safe strategy. It represents an alternative for patients with limited access to costly drugs. (REV INVES CLIN. 2015;67:304-12)
Key words: Multiple myeloma. Treatment. Thalidomide. Dexamethasone.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
INTRODUCTION
Multiple myeloma (MM) is the prototype of a spectrum of diseases known as plasma cell dyscrasias. It is a neoplastic disease of unknown etiology, characterized by the abnormal proliferation of plasma cells that produce excessive quantities of a specific immuno-globulin isotype.
In the United States, 14,000 new cases of MM are diagnosed every year1, representing 1% of all cancers
and 10-15% of hematological neoplasias2.
Early studies implicated angiogenesis inhibition as a therapeutic target in MM3-7. Recent studies have
re-vealed that cereblon (CRBN) is the molecular target of the immunomodulatory drugs. Cereblon is a sub-strate receptor of the cullin ring E3 ubiquitin ligase complex (CRL4CRBN). Thalidomide binds to CRBN to
inhibit the function of this complex, which is the reg-ulation of DNA repair, replication, and transcription. Cereblon is the primary target of thalidomide tera-togenicity. T-cell co-stimulation by immunomodulato-ry drugs is cereblon-dependent since they promote the interaction of the transcription factors Aiolos and Ikaros binding to CRL4CRBN with enhanced
ubiquitina-tion, which results in proteosomal degradation of T lymphocytes.
The first study reporting treatment efficacy of tha-lidomide in relapsing MM patients was by Singhal, et al. Most patients had relapsed after autologous stem cell transplantation. Their response (defined as a > 50% decrease in M protein) was documented in 32% of patients. Thalidomide dosage varied between 200 and 800 mg/day8.
Subsequently, other reports emerged on the use of thalidomide as a single agent in refractory MM with response rates between 24 and 65%9-14.
There are many studies that proved the combination therapy with thalidomide and dexamethasone as an effective treatment in refractory MM. The overall re-sponse rate with this treatment is 41-55%15-17, and
63-72% in untreated MM18,19.
In the past decade, MM therapy has radically changed due to the development of treatment regimes that include immunomodulating agents (thalidomide,
lenalidomide) and proteasome inhibitors (bortezomib). These treatment regimens have increased response rates and overall survival (OS). Unfortunately, lenalid-omide and bortezomib are expensive and not afford-able drugs for every healthcare system, particularly those of developing countries.
The primary objective of this study was to evaluate the response rates, and the secondary objectives were to evaluate OS and event-free survival (EFS), in patients treated with thalidomide and dexamethasone as induction therapy, and to evaluate the toxicity of this regimen according to the NCI Common Terminol-ogy Criteria for Adverse Events, Version 3.0.
PATIENTS AND METHODS
Study design
The study was approved by the local Ethics Commit-tee (local Ethics CommitCommit-tee protocol number: 1604). It was conducted in accordance with the guidelines stipulated in the Declaration of Helsinki. All enrolled patients signed an informed consent form. All re-cently diagnosed MM patients meeting the inclu-sion criteria received the same treatment: thalido-mide: initial dose 50 mg orally at night; the dose was increased weekly by 50 mg until 200 mg was reached depending on drug tolerance. Dexametha-sone: 40 mg orally on days 1-4, 9-12, and 17-20. As-pirin 100 mg orally every 24 hours since treatment initiation, omeprazole 20 mg orally every 24 hours, sennosides 17.2-34.4 mg in case of constipation. Each cycle was repeated every four weeks until the best response was obtained, or if there was unac-ceptable toxicity, disease progression, or the patient’s wish to withdraw the consent for treatment. We de-fined best response as: a decrease in monoclonal paraprotein to < 25% (compared with the immedi-ately previous monoclonal spike) after two treat-ment cycles. In the case of disappearance of the monoclonal component on protein electrophoresis, the status of the monoclonal band by protein immu-nofixation was assessed after two treatment cycles. The response criteria used were the International Myeloma Working Group Uniform Response Crite-ria (IMWG): complete response (CR), partial response (PR), very good partial response (VGPR), stable dis-ease, and progressive disease20.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
The use of zoledronic acid or pamidronate as part of supportive therapy was allowed. Dose modification according to toxicity is shown in table 1. The relative dose intensity (RDI) for thalidomide and dexametha-sone was calculated as a function of total dose in-tended per cycle, divided by the actual dose received at a given cycle. The index of RDI was calculated per cycle.
Eligibility criteria
Inclusion criteria for this study were: recently diag-nosed symptomatic patients with MM according to the IMWG20 and previously untreated; measurable disease
defined as serum monoclonal protein ≥ 1.0 g/dl and/ or urinary monoclonal protein ≥ 200 mg/24 hours, or free light chain ≥ 10 mg/dl and abnormal ratio; and a signed Informed Consent. Exclusion criteria were: pa-tients with non-secreting MM (absence of quantifi-able monoclonal protein), history of previous malig-nant disease (except in situ cervical or breast cancer, basal cell or skin squamous cell carcinoma) unless the patient had been disease-free for ≥ 5 years; pregnant or lactating women; grade ≥ 2 peripheral neuropathy; females in reproductive age who could not use, or who refused, birth control with two methods; and males re-fusing to use barrier birth control methods.
Statistical analysis
Continuous variables were described as medians and ranges, categorical variables were described as fre-quencies and proportions. To estimate proportion
differences between groups, Fisher’s exact test was used. Survival analysis was determined by Kaplan-Meier curves. Survival-related prognostic factors were analyzed with the Cox proportional hazards regres-sion model. Overall survival was calculated from the time of treatment initiation until death or the last date in which we could ascertain that the patient was alive. Event-free survival was calculated from the time of treatment initiation to the date of progression, re-lapse, or death due to any cause. Analyses were per-formed using SPSS, v.20.0.
RESULTS
Patients
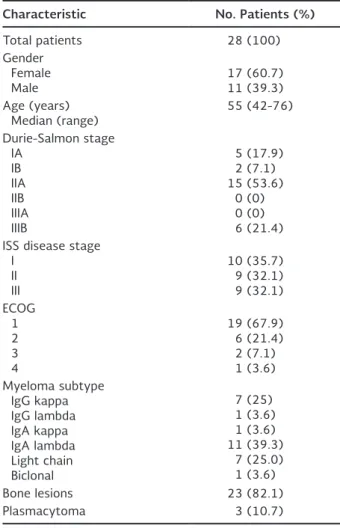
We included 28 patients between February 2006 and October 2011. Median follow-up was 31 months (range, 2-75). Patient demographic characteristics at diagnosis are shown in table 2. Six patients (21.4%) were considered of high-risk by karyotype (chromo-some 13 or 17 deletion) or FISH (deletion of 17p13.1, t(4;14),t(14;16)), and only one had t(11;14).
Response to therapy
The median number of chemotherapy cycles required to reach the best response was 6.5 (range, 2-12). Re-sponses to treatment are shown in table 3. Overall responses (CR + PR + VGPR) were 75%: seven patients experienced CR (25%), nine PR (32.1%), and five VGPR (17.9%).
Table 1. Dose modification according to National Cancer Institute Common Terminology Criteria for Adverse Events toxicity
Drug Dose modification
Thalidomide a) Peripheral neuropathy
Grade 1 toxicity: thalidomide reduction by 50%
Grade 2 toxicity: thalidomide discontinued until symptom resolution or decreased to grade 1 and then thalidomide resumed, reduced by 50%
Grade 3 or 4 toxicity: thalidomide suspended indefinitely
b) Any other grade 2 toxicity: thalidomide reduction by 50% (if administered dose was 50 mg, it was administered every other day)
c) Any other grade 3 toxicity: thalidomide was discontinued; if it improved to grade ≤ 2, then thalidomide reinitiated at 50% of the initial dose
Dexamethasone Grade ≥ 3 toxicities: dexamethasone discontinued until symptom resolution and then resumed with a dose reduction by one level
1st level reduction: 20 mg orally on days 1-4, 9-12, and 17-20
2nd level reduction: 20 mg orally on days 1-4 and 17-20
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
Toxicity
The most frequently observed adverse event was neu-ropathy, detected in 64.2% of patients; however, only two patients progressed to grade 3 (7.14%). Other adverse events developed in over 10% of cases, and included constipation, Cushing and edema, deep ve-nous thrombosis, and pneumonia. There were three deaths in the induction phase, one due to pneumonia and two in which the cause of death was unknown. Ta-ble 4 summarizes the most frequent adverse events.
Dexamethasone was reduced to level 1 in 15 patients (54%), and in 10 of them (36%) it was further reduced to level 2. The median of time to dose reduction level 1 was four months (range, 2-4), and to dose reduction level 2 was six months (range, 4-9). Twelve patients (43%) did not require any reduction.
Thalidomide was reduced in 12 patients (43%), and in six patients (21%) it was suspended indefinitely during the study. The median of time to the first re-duction was six months (range, 3-10), and to discon-tinuation was eight months (range, 4-11). Fourteen patients (50%) did not require any reduction.
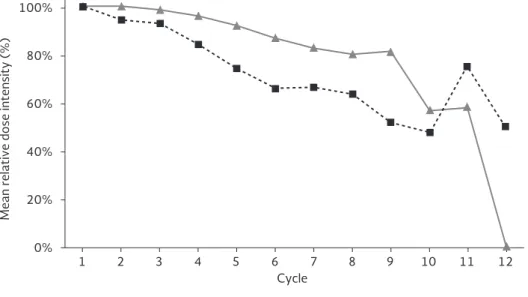
The RDI is shown in figure 1. Analysis of RDI per cycle shows that dexamethasone mean RDI was maintained above 74% until cycle 5, and thalidomide mean RDI was maintained above 74% until cycle 9.
Autologous transplant
Three patients (10.7%) received high-dose melphalan (200 mg/m2) and autologous transplant as
consoli-dation therapy. Their OS were 50, 66, and 29 months.
Overall survival and event-free survival
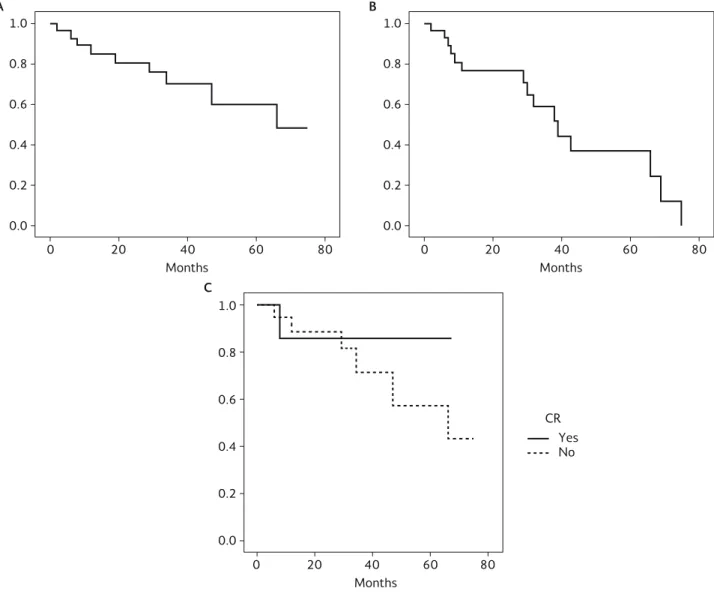
Median OS was 66 months (range, 34-not calculable) and median EFS was 39 months (range, 27.6-50.4). Figures 2 A and B show the OS and EFS Kaplan-Meier
Table 2. Patient’s demographic and clinical characteristics
Characteristic No. Patients (%)
Total patients 28 (100) Gender
Female
Male 17 (60.7)11 (39.3) Age (years)
Median (range) 55 (42-76) Durie-Salmon stage
IA IB IIA IIB IIIA IIIB
5 (17.9) 2 (7.1) 15 (53.6)
0 (0) 0 (0) 6 (21.4) ISS disease stage
I II III
10 (35.7) 9 (32.1) 9 (32.1) ECOG
1 2 3 4
19 (67.9) 6 (21.4) 2 (7.1) 1 (3.6) Myeloma subtype
IgG kappa IgG lambda IgA kappa IgA lambda Light chain Biclonal
7 (25) 1 (3.6) 1 (3.6) 11 (39.3)
7 (25.0) 1 (3.6) Bone lesions 23 (82.1)
Plasmacytoma 3 (10.7)
ISS: International Staging System; ECOG: Eastern Cooperative Oncology Group.
Table 3. Response to treatment
Response No. Patients (%)
Complete response 7 (25.0) Very good partial response 5 (17.9) Partial response 9 (32.1) Stable disease 1 (3.6) Progressive disease 4 (14.3)
Not evaluated 2 (7.1)
Table 4. Adverse events according to National Cancer Institute
Common Terminology Criteria for Adverse Events
Adverse event No. (%) Grade 3 or 4 No. (%)
Neuropathy 18 (64.2) 2 (7.14)
Cushing 5 (17.9) 0 (0)
Pneumonia 4 (14.2) 4 (14.2) Constipation 3 (10.7) 1 (3.6)
DVT 3 (10.7) 1 (3.6)
Cellulitis 2 (7.1) 0 (0) Cytopenias 1 (3.6) 0 (0) Bradycardia 1 (3.6) 1 (3.6) Somnolence 1 (3.6) 0 (0)
DVT: deep venous thrombosis.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
100%
80%
60%
40%
20%
0%
1 2 3 4 5 6 7 8 9 10 11 12 Cycle
Mean relative dose intensity (%)
Thalidomide Dexamethasone
curves. On univariate analysis, variables affecting OS were extramedullary disease, chromosome 13 dele-tion, t(14;16), and patients with high-risk cytoge-netics, as a group. The first three variables were still significant on multivariate analysis, HR: 41 (95% CI: 4.1-381.7), p = 0.001; HR: 9.2 (95% CI: 1.1-77.1), p = 0.039; HR: 32.97 (95% CI 1.2-868.8), p = 0.036, respectively. On univariate analysis of EFS, female gender and having been treated with bisphosphonates were variables that improved this outcome, but they did not remain significant on multivariate analysis. After five years, the OS of patients achieving CR was 86%, compared to 58% in the group that did not achieve CR. This difference was not statistically sig-nificant, probably due to the small number of patients. Figure 2 (c) shows the OS Kaplan-Meier curve in terms of CR.
DISCUSSION
This study arose from the need to search for a strategy that would increase the rate of responses and the outcomes of patients with MM in a scenar-io in which access to drugs such as bortezomib and lenalidomide as well as autologous bone marrow transplantation is limited due to high costs. The pur-pose of this study was to determine the impact of
thalidomide/dexamethasone administration until the best response was achieved in each patient, the qual-ity of these responses, OS, EFS, and toxicqual-ity.
In this report, the number of female patients was higher than that of male patients and the most com-mon isotype was IgA. According to the GLOBOCAN 2012 report, in Mexico, the percentage of MM female patients was 46%. However, in our database from 2007 to 2012, we diagnosed 73 patients with MM, of which 55% were female, and IgG isotype was the most common (48%) followed by IgA (30%). There-fore, we think that the higher frequency of IgA isotype found in our report was just a population bias.
A previously published series of patients treated with 4-6 cycles of thalidomide/dexamethasone that were not candidates for autologous transplant, yielded the following results: CR 5%, OS 21 months, and EFS 11 months21. Parameters defining CR and OS were
more stringent in our study. We must underscore that the median age in that study21 was 66 years (range,
36-78), higher than in our study.
Two phase III trials designed in parallel were conduct-ed to answer two separate questions concerning the efficacy of thalidomide/dexamethasone at short term (four months) developed by Eastern Cooperative
Figure 1. Relative dose intensity (dose intended/dose delivered/time) of thalidomide and dexamethasone. Thalidomide mean relative dose intensity was maintained above 74% until cycle 5, and thalidomide mean relative dose intensity was maintained above 74% until cycle 9.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80
Months A
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80
Months B
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80
Months C
CR Yes No
Oncology Group, and at long term (until progression) developed in the USA, Australia, Poland, and Spain. In the first study18, since therapy was limited to four
cycles, complete responses were achieved only in 4% of the patients. In the second study22, therapy was
administered until progression or undue toxicity. Me-dian age was 64 years (range, 39-86). The treat-ment schedule differed from the one given in the present study in the dexamethasone dose. They ad-ministered dexamethasone 40 mg orally on days 1-4, 9-12, and 17-20 during cycles 1 through 4, and 40 mg orally on days 1-4 beginning with cycle 5. Patients treated with thalidomide/dexamethasone reached
CR in 7.7% and VGPR plus CR in 44%. The OS at 30 months was 59%, and median PFS was 15 months. As expected due to the lower dexamethasone dose, pneumonia and peripheral neuropathy grades 3 or 4 were less frequent (Table 4); on the other hand, since thromboprophylaxis was not mandatory, deep vein thrombosis was more frequent and they report-ed pulmonary embolism as well (6.8% grade 3 or 4). In our study, the dexamethasone dose was not re-duced beyond a specific cycle, and it was rere-duced as required by toxicity. The higher rates of CR and VGPR in our study emphasize the role of high-dose dexa-methasone.
Figure 2. Kaplan-Meier plots for overall survival (A), event-free survival (B), and overall survival by complete response (C). Five-year overall survival for patients that reached complete response was 86% (continuous line) compared to 58% of patients that did not (dotted line).
CR: complete response.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
If we compare the results of thalidomide/dexametha-sone administration until achieving the best response, with phase III results of the melphalan/prednisone/tha-lidomide (MPT) arm of a trial comparing MPT vs. mel-phalan/prednisone, the median age of patients in these studies was also higher than that of our group23-27.
Although MPT is a triple drug combination, the ste-roid used is prednisone, which is a less potent drug than dexamethasone in the treatment of MM. Com-plete remission rates varied between 7 and 16%, me-dian OS was 29-52%, and PFS was 13-28%.
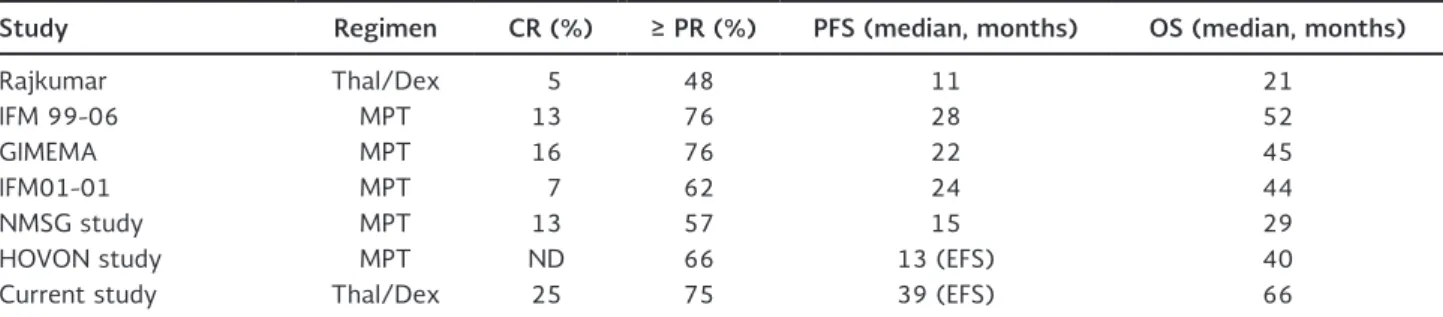
Although it is inappropriate to compare those report-ed OS with ours due to the great difference in pa-tients’ median ages, our CR rate practically doubled that obtained with MPT, and relapses occurred at least 11 months earlier than the ones of the patients treated with our strategy. Table 5 depicts response rates and outcomes of several studies.
The frequency of grade 3 and 4 infections referred in our study is similar to that in the MPT study, but more frequent than in the study by Rajkumar, et al.21.
Only one patient developed grade 3 deep venous thrombosis in our study. Unlike Rajkumar’s study21 in
which no patient received prophylactic anti-throm-botic therapy, it was mandatory that all patients in our cohort be treated with aspirin 100 mg/day, ex-cept in cases that were anti-coagulated for medical reasons. The frequency of thrombosis was also lower than that reported by the GIMEMA group (11%)24,
but in that study no anti-thrombotic prophylaxis was initially administered; once half of the patients had been recruited, a frequency of grade 3 or 4 thrombosis of
17% was observed; afterwards, prophylactic enoxapa-rin was administered duenoxapa-ring the first four chemother-apy cycles, resulting in a decrease of the number of these episodes to 3%. The GIMEMA24 and IFM 99-0626
studies reported grade 3 or 4 thrombosis in 12% of cases and neither used anti-thrombotic prophylaxis.
The frequency of grade 3 or 4 peripheral neuropathy was 7%, similar to that reported in two MPT series. The HOVON27 study reported a rate of peripheral
neuropathy of 23%, but that study administered tha-lidomide as maintenance therapy. Table 6 summariz-es the adverse events in different studisummariz-es.
As expected, extramedullary disease, chromosome 13 deletion, and t(14;16) were deleterious factors in OS. One patient’s karyotype showed a 19p13 de-letion; this chromosomal abnormality has been pre-viously described in MM28,29, but its prognostic
sig-nificance has not been determined. It has also been described in pre-B acute lymphoblastic leukemia. This gene encodes the immunoglobulin enhancer-binding factor E12/E47. This patient’s disease was character-ized by extramedullary plasmacytomas of the larynx and colon, and the 19p13 deletion was the only chro-mosomal abnormality detected.
Patients that achieved CR had an OS of 86% at five years. Achieving CR and maintaining it has a direct im-pact on OS; this has been previously shown in patients treated with total therapy 2 (TT2)30 that had an OS at
three years of almost 90% in the group that went into CR and maintained it, vs. 65% in the group that did not achieve CR. Another study showed that achieving CR is an independent factor in the long-term outcome,
Table 5. Summary of response and survival rates in other studies
Study Regimen CR (%) ≥ PR (%) PFS (median, months) OS (median, months)
Rajkumar Thal/Dex 5 48 11 21
IFM 99-06 MPT 13 76 28 52
GIMEMA MPT 16 76 22 45
IFM01-01 MPT 7 62 24 44
NMSG study MPT 13 57 15 29
HOVON study MPT ND 66 13 (EFS) 40
Current study Thal/Dex 25 75 39 (EFS) 66
CR: complete response; PR: partial response; PFS: progression-free survival OS: overall survival; EFS: event-free survival; IFM: Intergroupe Francophone du Myélome; GIMEMA: Gruppo Italiano Malattie Ematologiche dell’Adulto; NMSG: Nordic Myeloma Study Group;
HOVON: Hemato-Oncologie voor Volwassenen Nederland; Thal/Dex: thalidomide/dexamethasone; MPT: melphalan, prednisone, thalidomide; ND: not determined.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
regardless of age and International Staging System score31.
The use of high dexamethasone doses (480 mg/month) is considered unnecessary when using a treatment regimen that includes bortezomib or lenalidomide, and it may even be deleterious in terms of adverse events and mortality when compared with the use of low dexamethasone doses32. Lenalidomide and
tha-lidomide have similar structures and mechanisms of action. Both drugs direct cytotoxic effects on myelo-ma cells and are capable of inducing apoptosis or pro-grammed cell death33. Also, these agents are capable
of stimulating T-cell, interleukin-2 (IL-2), and interfer-on (IFN)-γ production. Lenalidomide has been shown
to be anywhere from 50 to 2,000 times more potent than thalidomide in the stimulation of T-cell pro-duction, and 50-100 times more potent in the stim-ulation of IL-2, and IFN-γ production. The
augmenta-tion of T-cell response leads to an increased producaugmenta-tion of IL-2, which in turn leads to alterations in the num-ber and function of natural killer (NK) cells, increas-ing the activity of NK-dependent cytotoxicity. In ad-dition, thalidomide and lenalidomide have been shown to inhibit the production of tumor necrosis factor (TNF)-α through two mechanisms: increasing the
degradation of TNF-α mRNA and increasing the ac-tivity of α-1-acid glycoproteins, which have intrinsic
anti-TNF-α activity34,35.Such inhibition leads to
de-creased myeloma cell growth and survival. Here, too, lenalidomide has been shown to be more potent than thalidomide. Some suggest that lenalidomide may be up to 50,000 times more potent in inhibiting TNF-α than thalidomide36.In addition, these agents
are capable of modulating the expression of cell surface adhesion molecules, interfering with growth signaling between myeloma cells and bone marrow stromal cells37.Lastly, these agents are capable of
reducing angiogenesis through the inhibition of the secretion of vascular endothelial growth factor (VEGF), a pro-angiogenic cytokine that is secreted by bone marrow stromal cells and myeloma cells38.Inhibition
of VEGF leads to alterations in the microvasculature of the bone marrow environment and inhibits myeloma cell growth and proliferation.
The role of low-dose dexamethasone in combination with thalidomide remains to be determined. Our regi-men-associated mortality was 10.7%, which is not neg-ligible; however, the CR and OR (25 and 75%, respec-tively) as well as an EFS of 39 months in the absence of newer and more potent drugs makes this regimen an attractive strategy. High-dose dexamethasone also increases the risk of thrombosis, but the frequency of grade 3-4 thrombosis was 4% when using aspirin as prophylactic therapy.
In the current study we reported better EFS and OS than other series treated with thalidomide/dexameth-asone, as well as higher CR rates. It is possible that our results reflect the effect of uninterrupted therapy versus limited number of cycles.
Induction therapy with thalidomide and dexametha-sone until achieving the best response in patients with recently diagnosed MM is a useful and safe strategy. It represents an affordable alternative for patients with limited access to more expensive drugs.
Table 6. Summary of grade 3 or 4 adverse events in other studies according to National Cancer Institute Common Terminology Criteria for Adverse Events
Study Regimen Infection
(%) Thrombosis (%) Peripheral neuropathy (%)
Rajkumar Thal/Dex 5 10 6
IFM 99-06 MPT 13 12 6
GIMEMA MPT 10 12 8
IFM01-01 MPT ND 6 2
NMSG study MPT ND ND 6
HOVON study MPT 28 3 23
Current study Thal/Dex 14 4 7
IFM: Intergroupe Francophone du Myélome; GIMEMA: Gruppo Italiano Malattie Ematologiche dell’Adulto; NMSG: Nordic Myeloma Study Group; HOVON: Hemato-Oncologie voor Volwassenen Nederland; Thal/Dex: thalidomide/dexamethasone; MPT: melphalan, prednisone, thalidomide; ND: not defined.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N
ACKNOWLEDGMENTS
Déborah Martínez-Baños is a doctoral student from Pro-grama de Doctorado en Ciencias Biomédicas, Universidad Nacional Autónoma de México (UNAM), and received finan-tial support from CONACyT (SALUD-2007-C01-69695).
REFERENCES
1. Munshi NC, Tricot G, Barlogie B. Plasma cell neoplasms. In: De Vita VT, Hellman S, Rosenberg SA (eds). Cancer: Principles and Practice on Oncology. 6th ed. Philadelphia, PA. Lippincott Wil-liams and Wilkins; 2001. p 2465-99.
2. Wingo PA, Tong T, Bolden S. Cancer Statistics: 1995. CA Cancer J Clin. 1995;45:8-30.
3. Folkman J. Angiogenesis in cancer, vascular, rheumatoid and other diseases. Nat Med. 1995;1:27-31.
4. Vacca A, Ribatti D, Roncali L, Ranieri G, Silvestris F, Dammaco F. Bone marrow angiogenesis and progression in multiple myelo-ma. Br J Haematol. 1994;87:503-8.
5. Rajkumar SV, Leong T, Roche PC, et al. Prognostic value of bone marrow angiogenesis in multiple myeloma. Clin Cancer Res. 2000;6:3111-16.
6. D’Amato RJ, Loughnan MS, Flynn E, Folkman J. Thalidomide is an inhibitor of angiogenesis. Proc Natl Acad Sci USA. 1994;91: 4082-5.
7. Hideshima T, Chauhan D, Shima Y, et al. Thalidomide and its analogs overcome drug resistance of human multiple myeloma cells to conventional therapy. Blood. 2000;96:2943-50. 8. Singhal S, Mehta J, Desikan R, et al. Antitumor activity of
tha-lidomide in refractory multiple myeloma. N Engl J Med. 1999; 341:1565-71.
9. Weber DM, Gavino M, Delasalle K, Rankin K, Giralt S, Alexanian R. Thalidomide alone or with dexamethasone for multiple my-eloma. Blood. 1999;94(Suppl 1):604a [Abstract 2686). 10. Durie BGM, Stepan DE. Efficacy of low dose thalidomide (T)
in multiple myeloma. Blood. 1999;94(Suppl 1):316a [Ab-stract].
11. Juliusson G, Celsing F, Turesson I, Lenhoff S, Adriansson M, Malm C. Frequent good partial remissions from thalidomide including best response ever in patients with advanced refractory and relapsed myeloma. Br J Haematol. 2000;109:89-96.
12. Rajkumar SV, Fonseca R, Dispenzieri A, et al. A phase II trial of thalidomide in the treatment of relapsed multiple myeloma (MM) with laboratory correlative studies. Blood. 2000;96:168a; [Ab-stract 724].
13. Kneller A, Raanani P, Hardan I, et al. Therapy with thalidomide in refractory multiple myeloma patients –the revival of an old drug. Br J Haematol. 2000;108:391-3.
14. Tosi P, Ronconi S, Zamagni E, et al. Salvage therapy with tha-lidomide in multiple myeloma patients relapsing after autolo-gous peripheral blood stem cell transplantation. Haematologica. 2001;86:409-13.
15. Dimopoulos MA, Zervas K, Kouvatseas G, et al. Thalidomide and dexamethasone combination for refractory multiple myeloma. Ann Oncol. 2001;12:991-5.
16. Palumbo A, Giaccone L, Bertola A, et al. Low-dose Thalidomide plus dexamethasone is an effective salvage therapy for ad-vanced myeloma. Haematologica. 2001;86:399-403.
17. Weber DM, Gavino M, Delasalle K, Rankin K, Giralt S, Alexanian R. Thalidomide alone or with dexamethasone for multiple myelo-ma. Blood. 1999;94(Suppl 1):604a [Abstract 2686].
18. Rajkumar SV, Blood E, Vesole D, Fonseca R, Greipp P. Phase III clinical trial of thalidomide plus dexamethasone compared with dexamethasone alone in newly diagnosed multiple myeloma: a clinical trial coordinated by the Eastern Cooperative Oncology Group. J Clin Oncol. 2006;24:431-6.
19. Weber D, Rankin K, Gavino M, Delasalle K, Alexanian R. Tha-lidomide alone or with dexamethasone for previously untreated multiple myeloma. J Clin Oncol. 2003;21:16-19.
20. Durie BG, Harousseau J-L, Miguel JS, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20: 1467-73.
21. Dingli D, Rajkumar SV, Nowakowski G, et al. Combination therapy with thalidomide and dexamethasone in patients with newly diag-nosed multiple myeloma not undergoing upfront autologous stem cell transplantation: a phase II trial. Haematologica. 2005;90:1650-4. 22. Rajkumar SV, Rosiñol L, Hussein M, et al. Multicenter, randomized,
double-blind, placebo-controlled study of thalidomide plus dexa-methasone compared with dexadexa-methasone as initial therapy for newly diagnosed multiple myeloma. J Clin Oncol. 2008; 26:2171-7. 23. Waage A, Gimsing P, Fayers P, et al. Melphalan and prednisone
plus thalidomide or placebo in elderly patients with multiple myeloma. Blood. 2010;116:1405-12.
24. Palumbo A, Bringhen S, Caravita T, et al. GIMEMA Oral melphalan and prednisone chemotherapy plus thalidomide compared with melphalan and prednisone alone in elderly patients with multiple myeloma: randomized controlled trial. Lancet. 2006;367:825-31. 25. Hulin C, Facon T, Rodon P, et al. Efficacy of melphalan and pred-nisone plus thalidomide in patients older than 75 years with newly diagnosed multiple myeloma: IFM 01/01 Trial. J Clin On-col. 2009;27:3664-70.
26. Facon T, Mary JY, Hulin C, et al. Melphalan and prednisone plus thalidomide versus melphalan and prednisone alone or reduced-intensity autologous stem cell transplantation in elderly pa-tients with multiple myeloma (IFM 99–06): a randomized trial. Lancet. 2007;370:1209-18.
27. Wijermans P, Schaafsma M, Termorshuizen F, et al. Phase III study of the value of thalidomide added to melphalan plus pred-nisone in elderly patients with newly diagnosed multiple my-eloma: The HOVON 49 Study. J Clin Oncol. 2010;28:3160-6. 28. Taniwaki M, Nishida K, Takashima T, et al. Nonrandom
chromo-somal rearrangements of 14q32.3 and 19p13.3 and preferen-tial deletion of 1p in 21 patients with multiple myeloma and plasma cell leukemia. Blood. 1994;84:2283-90.
29. Taniwaki M, Nishida K, Ueda Y, Takashima T. Non-random chro-mosomal rearrangements and their implications in clinical fea-tures and outcome of multiple myeloma and plasma cell leuke-mia. Leuk Lymphoma. 1996;21:25-30.
30. Hoering A, Crowley J, Shaughnessy JD, et al. Complete remission in multiple myeloma examined as time-dependent variable in terms of both onset and duration in Total Therapy protocols. Blood. 2009;114:1299-305.
31. Gay F, Larocca A, Wijermans P, et al. Complete response cor-relates with long-term progression-free and overall survival in elderly myeloma treated with novel agents: analysis of 1175 pa-tients. Blood. 2011;117:3025-31.
32. Rajkumar SV, Jacobus S, Callander NS, et al. Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomized controlled trial. Lancet On-col. 2010;11:29-37.
33. Anderson KC. Lenalidomide and thalidomide: mechanisms of ac-tion–similarities and differences. Semin Hematol. 2005;42:S3-8. 34. Hideshima T, Chauhan D, Shima Y, et al. Thalidomide and its
analogs overcome drug resistance of human multiple myeloma cells to conventional therapy. Blood. 2000;96:2943-50. 35. Niwayama S, Turk IS, Liu JO. Potent inhibition of tumor necrosis
factor-alpha production by tetrafluorothalidomide and tetra-fluorophthalimides. J Med Chem. 1996;39:3044-5.
36. Bartlett JB, Dredge K, Dalgleish AG. The evolution of thalido-mide and its IMiD derivatives as anticancer agents. Nat Rev Cancer. 2004;4:314-22.
37. Geitz H, Handt S, Zwingenberger K. Thalidomide selectively mod-ulates the density of cell surface molecules involved in the adhe-sion cascade. Immunopharmacology. 1996;31:213-21. 38. Gupta D, Treon SP, Shima Y, et al. Adherence of multiple
my-eloma cells to bone marrow stromal cells upregulates vascular endothelial growth factor secretion: therapeutic applications. Leukemia. 2001;15:1950-61.
.r
e
hsi
l
b
u
p
e
ht
f
o
n
ois
si
mr
e
p
ne
tti
r
w r
oir
p
e
ht
t
u
o
hti
w
g
ni
y
p
oc
ot
o
h
p r
o
de
c
u
d
or
pe
r
e
b
ya
m
n
oit
aci
l
b
u
p s
i
ht
f
o t
ra
p
o
N