CorSalud 2019 Ene-Mar;11(1):46-53
RNPS 2235-145 © 2009-2019 Cardiocentro Ernesto Che Guevara, Villa Clara, Cuba. Artículo con Licencia de Creative Commons – CC BY-NC-ND 4.0 46
Sociedad Cubana de Cardiología
____________________________
Artículo Original
Cierre quirúrgico de comunicación interauricular en pacientes
mayores de 40 años de edad: Efecto sobre la función
cardíaca y resultados clínicos generales
Prof. Dr. Azman Ates
y Prof. Dr. Bilgehan Erkut
Servicio de Cirugía Cardiovascular, Medical Faculty of Ataturk University. Erzurum, Turkey.
Full English text of this article is also available
INFORMACIÓN DEL ARTÍCULO
Recibido: 21 de diciembre de 2018 Aceptado: 1 de febrero de 2019
Conflictos de intereses
Los autores declaran que no existen conflictos de intereses
Abreviaturas
CIA: comunicación interauricular
FA: fibrilación auricular
HTP: hipertensión pulmonar
PAP: presión arterial pulmonar
Qp/Qs: índice entre el flujo pulmonar y el sistémico
Bilgehan Erkut, Prof, MD. Atatürk University Medical Faculty. Department of Cardiovascular Surgery, Erzurum, Turkey. E-mail address:
bilgehanerkut@yahoo.com
RESUMEN
Introducción: La comunicación interauricular (CIA) es una de las cardiopatías
congénitas más frecuentes en los pacientes adultos.
Objetivo: Se evaluaron los resultados iniciales y a medio plazo del tratamiento
quirúrgico de la CIA tipo ostium secundum en pacientes mayores de 40 años de edad en relación con la función cardíaca y los resultados clínicos.
Método:Se estudiaron 32 pacientes,mayoresde40añosdeedad,aquienesseles
realizó corrección quirúrgica de una CIA tipo ostium secundum. Se compararon los parámetros ecocardiográficos, de función cardíaca y el estado clínico de todos los pacientes antes y después de la operación para evaluar la eficacia del trata-miento quirúrgico.
Resultados: Los pacientes fueron seguidos durante un promedio de 2,2 años
(rango 3 meses – 3,1 años). No hubo mortalidad en el postoperatorio. En el segui-miento temprano, no hubo ningún evento tromboembólico cerebrovascular y mejoraron las capacidades funcionales de los pacientes. No ocurrieron nuevas fibrilaciones auriculares. Los diámetros de la aurícula y el ventrículo derechos, y las presiones de la arteria pulmonar se redujeron significativamente, mientras que no se encontró variación en la fracción de eyección. La necesidad de tratamiento diurético se redujo después del tratamiento quirúrgico. No se detectó ningún cor-tocircuito intracardíaco residual durante el seguimiento.
Conclusiones:El cierre quirúrgico de la CIA en pacientes adultos mayores de 40
años puede mejorar la función cardíaca medida por ecocardiografía y reducir los síntomas clínicos. Incluso, si no se utiliza ningún tratamiento en estos pacientes, los síntomas son escasos y rara vez se encuentran alteraciones en los parámetros hemodinámicos con peligro para la vida. Sin embargo, la reparación quirúrgica debe realizarse lo antes posible, especialmente cuando se detecta en pacientes adultos.
Palabras clave:Comunicación interauricular, Cirugía, Adulto, Evaluación de
resul-tado (Atención de Salud)
Surgical closure of atrial septal defect in patients aged 40 years
and older: Effect on cardiac function and general clinical
outcomes
ABSTRACT
Introduction: Atrial septal defect (ASD) is one of the most common congenital
heart diseases in adult patients.
secundum atrial septal defects in patients with ≥ 40 years in terms of cardiac func-tions and clinical outcomes.
Method: Thirty-two patients who had undergone surgical correction for secundum
atrial septal defect at the age of 40 years an older were examined. Echocardio-graphic parameters, cardiac functions and clinical status of all patients were com-pared before and after the operation to evaluate the efficacy of surgical treatment.
Results: The patients were followed for an average of 2,2 years (range 3 months –
3,1 years). There was no mortality in the postoperative period. In the early follow-up, there was no cerebrovascular thromboembolic event, functional capacities of the patients improved. No new atrial fibrillation occurred. Right atrial and ventricle diameters, and pulmonary artery pressures were significantly reduced, while ejection fractions did not change. The need for diuretic therapy was reduced after surgical treatment. No residual intracardiac shunt was detected during follow-up. Conclusions: Surgical closure of atrial septal defects in adult patients over the age of 40 can improve cardiac function by echocardiography and reduce clinical com-plaints. Even if no intervention is made in such patients, the current complaints are scarce and life-threatening problems are rarely seen in hemodynamic parame-ters. However, surgical repair should be performed as soon as possible, especially when detected in adult patients.
Keywords: Atrial septal defect, Surgery, Adult, Outcome assessment (Health Care)
INTRODUCIÓN
La comunicación interauricular (CIA) es una de las cardiopatía congénitas más comunes en pacientes adultos. Si bien está presente en aproximadamente el 10% de los recién nacidos, la CIA es responsable del 40% de las cardiopatías congénitas en la vida
adulta1.
El cierre quirúrgico de la CIA tipo ostium secun-dum puede realizarse de forma segura, con muy baja morbilidad y mortalidad, aunque todavía existe controversia respecto a las indicaciones quirúrgicas
y sus opciones terapéuticas en pacientes adultos2,3.
Además, con el tratamiento quirúrgico definitivo se previenen complicaciones potencialmente mortales como: insuficiencia cardíaca, hipertensión pulmo-nar, complicaciones tromboembólicas y arritmias, que pueden aparecer más tardíamente en la
evo-lución natural de la enfermedad4,5. Los síntomas y
las alteraciones hemodinámicas parecen ser míni-mos en este tipo de pacientes, pero la reparación quirúrgica debe realizarse lo antes posible después
del diagnóstico2,3.
En esta investigación se analizan los efectos a corto y mediano plazo, así como los resultados, del tratamiento quirúrgico de la CIA en pacientes mayo-res de 40 años.
MÉTODO
Se incluyeron 32 pacientes mayores de 40 años, a
quienes se les diagnosticó CIA en el Departamento de Cirugía Cardiovascular de la Facultad de Medi-cina de la Universidad de Atatürk del Erzurum Re-gional Training and Research Hospital, entre agosto de 2009 y noviembre de 2018.
Un 37,5% de los casos (12 pacientes) ingresados para cirugía tenían más de 50 años de edad y 4 (12,5%) eran mayores de 60. Veintiuno de ellos (65,7%) son hombres y 11, mujeres (34,3%). El pri-mer diagnóstico se realizó mediante ecocardiografía en todos los pacientes y como todos tenían más de 40 años de edad, se les realizó coronariografía y cateterismo cardíaco derecho. No se encontraron lesiones significativas en las arterias coronarias de ninguno de los pacientes. La relación del flujo san-guíneo pulmonar y sistémico (Qp/Qs) se determinó mediante oximetría. Los pacientes del estudio tenían un cortocircuito interauricular predominante de izquierda a derecha, con un índice Qp/Qs de, al menos, 1,5:1. En estos casos, el Qp/Qs medio estuvo entre 1,5-2,0; 2,0-3,0 y ≥3,0 en 9 (28,1%), 19 (59,4%) y 4 (12,5%) pacientes, respectivamente.
No se incluyeron en este estudio a pacientes con otras enfermedades cardíacas o comorbilidades gra-ves, cirugía cardíaca previa, otra malformación car-díaca congénita, enfermedad valvular reumática, arteriopatía coronaria, regurgitación mitral o aórtica y disfunción ventricular izquierda. Los pacientes fueron evaluados clínica y ecocardiográficamente durante un período medio de seguimiento de 2,2 años.
Cierre quirúrgico de comunicación interauricular
CorSalud 2019 Ene-Mar;11(1):46-53 48
estudiados se definió en 3 categorías:
- HTP leve: presión arterial pulmonar (PAP) por
debajo de 50 mmHg (n=16, 50%)
- HTP moderada: PAP entre 50 y 75 mmHg (n=12,
37,5%)
- HTP grave: PAP superior a 75 mmHg (n=4, 12,5%)
Los datos referentes a la capacidad funcional (definida como clase I, II, III o IV, según la New York Heart Association [NYHA]), la necesidad de diuréti-cos y las alteraciones del ritmo cardíaco se com-pararon con los del período preoperatorio para evaluar la eficacia del tratamiento quirúrgico. Die-ciocho pacientes (56,3%) estaban en clase funional I y II, y 14 en las categorías III y IV (43,7%). También se evaluaron los diámetros de la aurícula y el ventrículo derechos, la PAP y la fracción de eyec-ción del ventrículo izquierdo, antes y después de la intervención quirúrgica.
Todas las operaciones se realizaron con circula-ción extracorpórea y temperatura corporal entre 32-36 °C. Se realizó esternotomía media a 27 pacientes (84,4%) y toracotomía derecha a 5 (15,6%), y se administró una solución cardioplégica cristaloide fría en la raíz aórtica para la protección miocárdica.
El tamaño del defecto septal se evaluó después de la atriotomía derecha y se comprobó el funcio-namiento de la válvula tricúspide. A los pacientes con insuficiencia tricuspídea grave se les realizó anuloplastia de De Vega, después del cierre de la
CIA con sutura o parche de pericardio o dacrón (Figura 1).
La evaluación postoperatoria temprana se realizó en el primer mes después de la cirugía. Posterior-mente, se realizó el seguimiento de todos los pa-cientes cada 3 meses hasta 3,1 años (media de 2,2 años) mediante un cuestionario o una entrevista telefónica, con el paciente o su médico de asistencia, o ambos. Se aconsejó a todos los pacientes que acu-dieran a las evaluaciones clínicas y ecocardiográ-ficas de seguimiento cada 6 u 8 meses, o tan pronto como fuera posible si aparecían nuevo síntoma o empeoraba su estado clínico.
Análisis estadístico
Para análisis estadístico se utilizó el programa SPSS 10.0 (SPSS, Chicago, IL, EEUU). Todos los resultados se expresan como media ± desviación estándar. La prueba de Kolmogorov-Smirnov se utilizó para el análisis de las variables. Se utilizaron pruebas t pa-readas para comparar los parámetros ecocardio-gráficos pre y posoperatorios de los pacientes, y las pruebas de McNemar para comparar el uso de diu-réticos, el estado del ritmo cardíaco y la capacidad funcional antes y después de la cirugía. Se consideró significativo el valor de p <0,05.
RESULTADOS
El análisis incluyó a 32 pacientes a quienes se les
Figura 1. Imágenes de dos pacientes a quienes se les realizó cierre quirúrgico de la CIA, con empleo de parche de
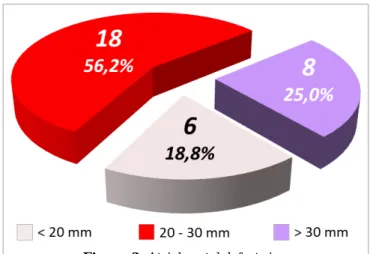
realizó corrección quirúrgica de una CIA ostium secundum; 11 mujeres (34,3%) y 21 hombres (65,7%), con una edad media de 46 ± 9 años (rango de 40 a 72 años). El diámetro de la CIA fue de 1,5 a 3,8 cm (me-dia de 2,1 ± 0,8 cm), su distribución se muestra en la figura 2.
La CIA se cerró con sutura directa en 5 pacientes (9,8%), en los demás se prefirió el uso de parche de pericardio (19 pacientes) o de dacrón (8 pacientes). Para el cierre directo se empleó la técnica de sutura continua con prolene 4/0 o 5/0.
Todos los pacientes sobrevivieron y su capaci-dad funcional mostró una mejoría significativa des-pués de la operación; pues, mientras que el número de pacientes en clase funcional I y II aumentó, se redujo el de aquellos con clase funcional III y IV (Tabla). Veintidós pacientes (68,8%) habían recibi-do tratamiento diurético antes de la operación, y solo 9 (28,1%) lo usaron posteriormente, lo que de-muestra una disminución importante de la necesi-dad de este tipo de fármacos, con un resultado estadísticamente significativo (p <0,005).
Antes de la operación, 7 pacientes (21,9%) tenían fibrilación auricular (FA); la fracción de eyección del ventrículo izquierdo fue menor de 45% en 9 pacien-tes (28,1%) y más de 45% en el resto. Los diámetros de la aurícula derecha fueron menores de 45 mm, 45-55 mm y mayores de 55 mm en 7 (21,9%), 16
(50%) y 9 pacientes (28,1%), respectivamente; y los del ventrículo derecho fueron menores de 30 mm, 30-50 mm, y mayores de 50 mm en 6 (18,7%), 20 (62,6%) y 6 pacientes (18,7%), respectivamente.
La media de los diámetros de aurícula y ventrí-culo derechos fue de 48,5 ± 6,7 y 36,9 ± 8,4 mm, respectivamente, antes de la operación. El mayor diámetro auricular derecho fue de 57 mm y el del ventrículo derecho, de 46 mm. Los valores de la fracción de eyección del ventrículo izquierdo, los diámetros de aurícula y ventrículo derechos y la
Tabla. Comparación de los datos pre y posoperatorios respecto a parámetros clínicos y variables ecocardiográficas.
Variable Preoperatorio Posoperatorio Valor de p
Capacidad funcional (NYHA)
Clase I 8 14 0,005
Clase II 10 15 0,005
Clase III 9 2 0,005
Clase IV 5 1 0,005
Uso de diuréticos 22 9 0,005
Fibrilación auricular 7 6 0,801
Fracción de eyección (%)
≤ 45 9 7 0,522
> 45 23 25 0,129
Diámetro de aurícula derecha (mm) 48,5 ± 6,7 41,9 ± 4,1 0,005 Diámetro de ventrículo derecha (mm) 36,9 ± 8,4 30,7 ± 7,8 0,005 Presión en arteria pulmonar (mmHg) 47,2 ± 11,1 37,8 ± 10,9 0,005
Significación estadística: p<0,05
Cierre quirúrgico de comunicación interauricular
CorSalud 2019 Ene-Mar;11(1):46-53 50
PAP antes y después de la operación se muestran en la tabla. Los diámetros de las cavidades derechas se redujeron significativamente después de la ope-ración (p<0,005). Los de la aurícula fueron mucho menores de 50 mm en 24 pacientes. El telecardio-grama mostró mejoras significativas en la vascu-larización pulmonar y reducción del tamaño del ventrículo derecho.
Las PAP se redujeron significativamente después de la operación (p <0,005) y solo fueron mayores de 60 mmHg en 2 pacientes. Aunque el número de pa-cientes con una fracción de eyección del ventrículo izquierdo superior a 45% aumentó en el período pos-operatorio, en comparación con el prepos-operatorio, este resultado no fue estadísticamente significativo (p=0,129)
El ecocardiograma preoperatorio demostró in-suficiencia tricuspídea leve en 3 (9,3%) pacientes y moderada o grave en 15 (46,9%), en estos últimos se realizó la prueba con inyección de agua en el trasoperatorio. En los 11 pacientes (34,4%) donde se demostró insuficiencia grave, se realizó anuloplastia de De Vega. Después de la operación, solo 2 pacien-tes presentaron insuficiencia tricuspídea leve. A los que se les realizó anuloplastia tricuspídea por el mé-todo de De Vega evolucionaron favorablemente du-rante el período de seguimiento.
Un paciente (3,1%) tenía insuficiencia mitral debi-do a una hendidura (cleft) mitral y se le realizó val-vuloplastia. Otro paciente (3,1%) tenía una conexión anómala de venas pulmonares, que fue tratada junto con la CIA, y 10 pacientes (31,2%) tenían insuficien-cia aórtica que no fue clínicamente significativa.
El porcentaje de pacientes con FA disminuyó después de la operación (de 21,8% a 18,7%), pero
esta diferencia no fue significativa (Tabla). Aunque
2 pacientes recuperaron el ritmo sinusal normal después de la operación, 1 de ellos tuvo una nueva FA en el período posoperatorio. Para prevenir las complicaciones tromboembólicas, en 5 pacientes con FA se inició tratamiento anticoagulante inmedia-tamente después de la extracción de los tubos de drenaje torácico.
Seguimiento tardío
Veintinueve pacientes mantuvieron un seguimiento entre 3 meses y 3,1 años (media de 2,2 años). Se per-dieron 2 pacientes durante el seguimiento, después de mudarse a otra ciudad en Turquía, y otro murió en un accidente de tráfico. Los 29 pacientes presen-taron clase funcional I o II en el seguimiento a medio plazo, 3 de ellos restauraron el ritmo sinusal en el
segundo año de seguimiento. No aparecieron arrit-mias tardías en ningún paciente. Se mantuvo el tra-tamiento anticoagulante en los pacientes que conti-nuaron con la FA. Se detectó insuficiencia mitral grave en 1 paciente durante el seguimiento, causada por un prolapso de ambas valvas, y se le realizó re-emplazo valvular mitral a los 2 años de la operación inicial. También se detectó insuficiencia tricuspídea grave en 1 paciente con anuloplastia de De Vega, en quien se optó por tratamiento médico.
DISCUSIÓN
El tratamiento quirúrgico de la CIA se ha realizado con éxito en muchos centros durante más de 40 años. Las tasas de morbilidad y mortalidad periope-ratorias eran de 10 a 20% a finales de la década de 1950 y disminuyeron a 6% después de la década de
1960, hasta alcanzar un 0,5% en la actualidad6. Esta
mejoría del éxito quirúrgico y las tasas de supervi-vencia, así como la reducción de las complicacio-nes, se deben a las mejores técnicas operatorias y de los cuidados posoperatorios; por lo que el cierre quirúrgico de esta enfermedad congénita muy co-mún se ha recomendado más, recientemente, inclu-so en pacientes de mayor edad. No obstante, a pesar del éxito del procedimiento y de sus escasas com-plicaciones, se han publicado varios estudios en los últimos años que cuestionan la estrategia del cierre quirúrgico de rutina en pacientes con PAP eleva-da5,7-10.
La reparación quirúrgica sigue siendo el principal tratamiento de la CIA. La creencia previa de que solo el 50% de los pacientes con CIA no corregida sobreviven más de 40 años y que menos del 10% alcanzan los 60 años, no se ha confirmado en
mu-chos estudios observacionales2,6. Por lo tanto, la
es-peranza de vida de los pacientes con CIA no tratada
generalmente se acorta1,4,9,11-13. En particular, se
esti-ma que cuando aparecen los síntoesti-mas, los pacientes que reciben tratamiento quirúrgico tienen una ma-yor supervivencia que los que reciben tratamiento médico, y es similar a la de los pacientes que fueron
operados en su segundo o tercer año de vida7.
De-bido que la FA y otras arritmias, así como el flujo sanguíneo pulmonar, la sobrecarga de cavidades derecha y la aparición de la HTP, tienden a aumen-tar con la edad, la CIA debe corregirse incluso si el paciente está asintomático.
significati-vo e independiente de morbilidad y mortalidad2.
Murphy et al12 informaron que los pacientes que
recibieron la cirugía después de los 40 años de edad tenían mayor riesgo de complicaciones cardiovascu-lares postoperatorias, en cambio los niños y adultos jóvenes tienen un excelente pronóstico. Algunos de los pacientes operados en nuestra serie tenían más de 50 o 60 años y no se hubo morbilidad ni mortali-dad posoperatoria. Nuestros resultados sugieren que el cierre quirúrgico de la CIA mejora los sínto-mas y previene complicaciones posteriores en estos pacientes. El porcentaje de pacientes con clase fun-cional III-IV, según la NYHA, disminuyó de 43,8% a 9,3% después de la operación. Este resultado
coin-cide con lo encontrado por otros autores7,14, quienes
han planteado que la reparación quirúrgica de la CIA aumenta significativamente la supervivencia a largo plazo en pacientes de mediana edad y an-cianos.
Otros estudios han demostrado que la frecuencia de FA en pacientes con CIA aumenta a medida que
avanza la edad1,7,8,12. Además, se ha encontrado que
los trastornos del ritmo auricular son inducidos por diferentes mecanismos en los períodos pre y pos-operatorio; y antes de la cirugía, la principal causa
de FA es la distensión/dilatación auricular15. Aunque
no se conoce el mecanismo exacto, el desarrollo de FA en pacientes operados de CIA puede estar en relación con la cicatrización en el área del foco ectópico tras la reparación quirúrgica o en la zona de la canulación venosa durante la cirugía. El ta-maño de la aurícula derecha en nuestros pacientes disminuyó de 48,5 ± 6,7 a 41,9 ± 4,1 mm después de la operación, y uno de los que presentaba FA volvió al ritmo sinusal en el período posoperatorio; pero estos resultados no fueron estadísticamente signifi-cativos. No obstante, este caso nos mostró que el cierre de la CIA debe realizarse antes de la aparición de la FA.
La embolización en el posoperatorio de pacientes tratados quirúrgicamente cobra gran importancia por la posibilidad de lesión cerebral, de prolongar la estadía hospitalaria y aumentar los costos sanitarios. Su incidencia está estrechamente relacionada con la edad y los trastornos del ritmo cardíaco en el
peri-operatorio15. La FA es una posible causa del
aumen-to de la incidencia de episodios tromboembólicos en
pacientes operados de CIA14-16. Debido al alto riesgo
de embolia cerebral en pacientes ancianos con FA crónica, preferimos comenzar el tratamiento anticoa-gulante (warfarina) después de la cirugía, en los pa-cientes que la presentaron. También intentamos
reducir el riesgo de tromboembolismo, relacionado con los parches quirúrgicos, al cerrar las CIA peque-ñas mediante sutura directa; y debido a la necesidad de utilizar los parches en los defectos grandes, uti-lizamos los pericárdicos en lugar de los de dacrón debido a la predisposición tromboembólica de estos últimos.
Aunque no se recomienda el tratamiento anti-coagulante de rutina después del cierre de una CIA
con parche7, administramos warfarina en el período
posoperatorio a los pacientes con FA crónica y en los demás iniciamos tratamiento con aspirina. El valor del INR (international normalized ratio) se mantuvo entre 2,5-3,5 en pacientes tratados con warfarina, y sugerimos continuar el tratamiento con aspirina, durante al menos 3 meses –de acuerdo con las recomendaciones de las publicaciones actuales–,
en pacientes sin FA16-18. En los pacientes con FA no
se observaron complicaciones tromboembólicas en el posoperatorio, ni durante el seguimiento; lo que demostró que a pesar de presentar esta arritmia, el tratamiento anticoagulante previno posibles
episo-dios embólicos. Según Shah et al9, la incidencia de
embolia sistémica ha sido informada en pacientes con CIA, independientemente a que hayan sido tra-tados quirúrgicamente o con tratamiento farmacoló-gico; por lo tanto, después del cierre de estos defec-tos septales, se recomienda un adecuado control de las arritmias y el uso de tratamiento anticoagulante, en pacientes con FA, para prevenir eventos trombo-embólicos.
La incidencia de insuficiencia tricuspídea asocia-da aumenta con la easocia-dad. En este estudio, se detectó regurgitación moderada o grave de esta válvula en un 46,9% de los pacientes. En estos casos, el eco-cardiograma tiene, en ocasiones, una tendencia a la sobreestimación. Si antes de la operación se encuen-tran signos de insuficiencia tricuspídea moderada o grave, se recomienda realizar pruebas de competen-cia valvular con inyección de agua para decidir si existe indicación de anuloplastia tricuspídea. En estos pacientes, además del cierre de la CIA, sugeri-mos la importancia de la anuloplastia tricuspídea para reducir el índice cardiotorácico, mejorar la ca-pacidad funcional y mantener el ritmo sinusal nor-mal.
cor-Cierre quirúrgico de comunicación interauricular
CorSalud 2019 Ene-Mar;11(1):46-53 52
tocircuito y causar la muerte17,18. Es difícil predecir
en qué paciente con CIA se desarrollará esta en-fermedad vascular pulmonar. En los que tienen HTP grave, su cierre es muy difícil y peligroso. Fiore et
al7 informaron que el resultado operatorio en su
serie de pacientes con CIA, mayores de 50 años, no se vió influenciado por la presencia de HTP, cuando no existían resistencias vasculares muy aumentadas. Otros autores han sugerido que los aumentos de la PAP no están necesariamente relacionados con la edad, y el tamaño del cortocircuito no lo está con la
gravedad de los síntomas17,18. La cirugía debe
reali-zarse cuanto más joven sea el paciente, probable-mente antes de que se produzcan cambios estruc-turales en el miocardio o en la vasculatura
pulmo-nar19. A pesar de que la HTP grave fue poco
frecuen-te en nuestros pacienfrecuen-tes, sugerimos que, en quienes la padezcan, los cirujanos sean exquisitos al tomar la decisión de operar, independientemente de su edad.
La clase funcional avanzada, según la NYHA, tie-ne un importante impacto en la mortalidad tempra-na y tardía. En esta investigación encontramos utempra-na mejoría significativa del estado funcional, pues el porcentaje de pacientes con clases I y II aumentó de 56,2% en el preoperatorio a 90,6% después del
trata-miento quirúrgico (Tabla).
Además de la mejoría en la clase funcional de la NYHA, la correción quirúrgica de la CIA mejora la calidad de vida de los pacientes adultos y prolonga su esperanza de vida, al reducir las arritmias y el deterioro del lecho vascular pulmonar, y prevenir el desarrollo de insuficiencia cardíaca congestiva debi-do al crecimiento de las cavidades cardíacas; todebi-do lo cual produce resultados satisfactorios en beneficio de la función cardíaca. Debido a que no existe un tratamiento no quirúrgico alternativo que sea seguro y efectivo en relación al cierre quirúrgico (además del procedimiento de intervencionismo estructural con dispositivos de cierre septal), consideramos que el cierre anatómico debe realizarse lo antes posible en pacientes adultos mayores de 40 años de edad, con un índice Qp/Qs ≥ 1.5 y aumento de la PAP, incluso en aquellos mayores de 60 años que están en las clases funcionales III y IV de la NYHA. En los pacientes que reciben tratamiento quirúrgico debe controlarse estrechamente la aparición o permanen-cia de FA o flutter auricular, para prevenir o reducir la morbilidad y la mortalidad asociadas con el embolismo cerebral, y el tratamiento anticoagulante debe mantenerse en pacientes con FA persistente.
CONCLUSIONES
El cierre quirúrgico de la CIA en pacientes adultos mayores de 40 años puede mejorar la función car-díaca medida por ecocardiografía y reducir los sínto-mas clínicos. Si no se utiliza ningún tratamiento en estos pacientes, los síntomas son escasos y rara vez se encuentran alteraciones en los parámetros hemo-dinámicos con peligro para la vida. Sin embargo, la reparación quirúrgica debe realizarse lo antes posi-ble, especialmente cuando se detecta en pacientes adultos.
BIBLIOGRAFÍA
1. Jiang H, Wang ZW, Zhu HY, Zhang RF, Gong HD,
Wang HS, et al. Surgical treatment of secundum atrial septal defects in adults over 30 years old. Zhonghua Wai Ke Za Zhi. 2004;42(16):961-4.
2. John Sutton MG, Tajik AJ, McGoon DC. Atrial
sep-tal defect in patients ages 60 years or older: oper-ative results and long-term postoperoper-ative follow-up. Circulation. 1981;64(2):402-9.
3. Burke RP, Horvath K, Landzberg M, Hyde P,
Col-lins JJ, Cohn LH. Long-term follow-up after surgi-cal repair of ostium primum atrial septal defects in adults. J Am Coll Cardiol. 1996;27(3):696-9.
4. Attie F, Rosas M, Granados N, Zabal C, Buendía
A, Calderón J. Surgical treatment for secundum atrial septal defects in patients >40 years old. A randomized clinical trial. J Am Coll Cardiol. 2001; 38(7):2035-42.
5. Konstantinides S, Geibel A, Kasper W, Just H. The
natural course of atrial septal defect in adults - a still unsettled issue. Klin Wochenschr. 1991; 69(12):506-10.
6. Konstantinides S, Geibel A, Olschewski M,
Gör-nandt L, Roskamm H, Spillner G, et al. A compari-son of surgical and medical therapy for atrial sep-tal defect in adults. N Engl J Med. 1995;333(8):469-73.
7. Fiore AC, Naunheim KS, Kessler KA, Pennington
DG, McBride LR, Barner HB, et al. Surgical clo-sure of atrial septal defect in patients older than 50 years of age. Arch Surg. 1988;123(8);965-7.
8. Cheng TO. The natural course of atrial septal
de-fect in adults - a still unsettled issue. Clin Investig. 1992;70(1):85.
9. Shah D, Azhar M, Oakley CM, Cleland JG,
atrial septal defect in adults after medical or sur-gical treatment: a historical prospective study. Br Heart J. 1994;71(3):224-7.
10.Perloff JK. Surgical closure of atrial septal defect
in adults. N Engl J Med. 1995;333(8):513-4.
11.Driscoll D, Allen HD, Atkins DL, Brenner J,
Dun-nigan A, Franklin W, et al. Guidelines for evalua-tion and management of common congenital cardiac problems in infants, children, and adoles-cents. A statement for healthcare professionals from the Committee on Congenital Cardiac De-fects of the Council on Cardiovascular Disease in the Young, American Heart Association. Circula-tion. 1994;90(4):2180-8.
12.Murphy JG, Gersh BJ, McGoon MD, Mair DD,
Porter CJ, Ilstrup DM, et al. Long-term outcome after surgical repair of isolated atrial septal defect. Follow-up at 27 to 32 years. N Engl J Med. 1990; 323(24):1645-50.
13.Brickner ME, Hillis D, Lange RA. Congenital heart
disease in adults. First of two parts. N Engl J Med. 2000;342(4):256-63.
14.Shibata Y, Abe T, Kuribayashi R, Sekine S, Seki K,
Yamagishi I, et al. Surgical treatment of isolated secundum atrial septal defect in patients more than 50 years old. Ann Thorac Surg. 1996;62(4):
1096-9.
15.Chatzis A, Giannopoulos N, Vahlas C, Milonakis
M, Contrafouris C, Bobos D, et al. Surgical treat-ment of the atrial septal defect in adults: effective reduction in cardiac size and excellent overall clinical outcome. Rev Port Cir Cardiotorac Vasc. 2006;13(3):133-6.
16.Horvath KA, Burke RP, Collins JJ, Cohn LH.
Sur-gical treatment of adult atrial septal defect: early and long-term results. J Am Coll Cardiol. 1992; 20(5):1156-9.
17.Hörer J, Müller S, Schreiber C, Kostolny M,
Cleu-ziou J, Prodan Z, et al. Surgical closure of atrial septal defect in patients older than 30 years: risk factors for late death from arrhythmia or heart failure. Thorac Cardiovasc Surg. 2007;55(2):79-83.
18.Shaheen J, Alper L, Rosenmann D, Klutstein MW,
Falkowsky G, Bitran D, et al. Effect of surgical repair of secundum-type atrial septal defect on right atrial, right ventricular, and left ventricular volumes in adults. Am J Cardiol. 2000;86(12):1395-7.
19.Ghosh S, Chatterjee S, Black E, Firmin RK.
CorSalud 2019 Jan-Mar;11(1):46-53
RNPS 2235-145 © 2009-2019 Cardiocentro Ernesto Che Guevara, Villa Clara, Cuba. Article licensed under a Creative Commons Attribution – CC BY-NC-ND 4.0 46
Cuban Society of Cardiology
____________________________
Original Article
Surgical closure of atrial septal defect in patients aged 40 years
and older: Effect on cardiac function and
general clinical outcomes
Azman Ates
, Prof., MD; and Bilgehan Erkut, Prof., MD
Department of Cardiovascular Surgery, Medical Faculty of Ataturk University. Erzurum, Turkey.
Este artículo también está disponible en español
ARTICLE INFORMATION
Received: December 21, 2018 Accepted: February 1, 2019
Competing interests
The authors declare no competing interests
Acronyms
AF: atrial fibrillation
ASD: atrial septal defect
PAP: pulmonary artery pressure
PHT: pulmonary hypertension
Qp/Qs: ratio of pulmonary to systemic blood flow
Bilgehan Erkut, Prof, MD. Atatürk University Medical Faculty. Department of Cardiovascular Surgery, Erzurum, Turkey. E-mail address:
bilgehanerkut@yahoo.com
ABSTRACT
Introduction: Atrial septal defect (ASD) is one of the most common congenital
heart diseases in adult patients.
Objectives:We evaluated the early and mid-term results of surgical treatment of
secundum atrial septal defects in patients with ≥ 40 years in terms of cardiac func-tions and clinical outcomes.
Method:Thirty-two patients who had undergone surgical correction for secundum
atrial septal defect at the age of 40 years an older were examined. Echocardio-graphic parameters, cardiac functions and clinical status of all patients were com-pared before and after the operation to evaluate the efficacy of surgical treatment.
Results: The patients were followed for an average of 2,2 years (range 3 months –
3,1 years). There was no mortality in the postoperative period. In the early follow-up, there was no cerebrovascular thromboembolic event, functional capacities of the patients improved. No new atrial fibrillation occurred. Right atrial and ventricle diameters, and pulmonary artery pressures were significantly reduced, while ejection fractions did not change. The need for diuretic therapy was reduced after surgical treatment. No residual intracardiac shunt was detected during follow-up.
Conclusions:Surgical closure of atrial septal defects in adult patients over the age of 40 can improve cardiac function by echocardiography and reduce clinical com-plaints. Even if no intervention is made in such patients, the current complaints are scarce and life-threatening problems are rarely seen in hemodynamic parame-ters. However, surgical repair should be performed as soon as possible, especially when detected in adult patients.
Keywords:Atrial septal defect, Surgery, Adult, Outcome assessment (Health Care)
Cierre quirúrgico de comunicación interauricular en pacientes
mayores de 40 años de edad: Efecto sobre la función cardíaca y
resultados clínicos generales
RESUMEN
Introducción: La comunicación interauricular (CIA) es una de las cardiopatías
congénitas más frecuentes en los pacientes adultos.
Objetivo: Se evaluaron los resultados iniciales y a medio plazo del tratamiento
quirúrgico de la CIA tipo ostium secundum en pacientes mayores de 40 años de edad en relación con la función cardíaca y los resultados clínicos.
Método:Se estudiaron 32 pacientes, mayores de 40 años de edad, a quienes se les
los parámetros ecocardiográficos, de función cardíaca y el estado clínico de todos los pacientes antes y después de la operación para evaluar la eficacia del trata-miento quirúrgico.
Resultados: Los pacientes fueron seguidos durante un promedio de 2,2 años
(rango 3 meses – 3,1 años). No hubo mortalidad en el postoperatorio. En el segui-miento temprano, no hubo ningún evento tromboembólico cerebrovascular y mejoraron las capacidades funcionales de los pacientes. No ocurrieron nuevas fibrilaciones auriculares. Los diámetros de la aurícula y el ventrículo derechos, y las presiones de la arteria pulmonar se redujeron significativamente, mientras que no se encontró variación en la fracción de eyección. La necesidad de tratamiento diurético se redujo después del tratamiento quirúrgico. No se detectó ningún cortocircuito intracardíaco residual durante el seguimiento.
Conclusiones: El cierre quirúrgico de la CIA en pacientes adultos mayores de 40
años puede mejorar la función cardíaca medida por ecocardiografía y reducir los síntomas clínicos. Incluso, si no se utiliza ningún tratamiento en estos pacientes, los síntomas son escasos y rara vez se encuentran alteraciones en los parámetros hemodinámicos con peligro para la vida. Sin embargo, la reparación quirúrgica debe realizarse lo antes posible, especialmente cuando se detecta en pacientes adultos.
Palabras clave: Comunicación interauricular, Cirugía, Adulto, Evaluación de
resul-tado (Atención de Salud)
INTRODUCTION
Atrial septal defect (ASD) is one of the most com-mon congenital heart diseases in adult patients. While it is present in approximately 10% of newborn infants, ASD is responsible for 40% of congenital
heart diseases in adult life1.
Surgical closure of ostium secundum type atrial septal defects can be safely performed with very low morbidity and mortality even though there is still an existing discussion between surgical indications and
treatment options for adult patients with ASD2,3. In
addition, life-threatening complications such as heart failure, pulmonary hypertension, thromboembolic complications and arrhythmias, which may occur
later, with full surgical correction, are prevented4,5.
Symptoms and pathological hemodynamic problems appear to be minimal in this type of patient and surgical repair should be performed as soon as
pos-sible after diagnosis2,3.
In this study, we analyzed the early and mid-term effects and results of the surgical treatment of ASD in patients over 40 years of age.
METHOD
Between August 2009 and November 2018, 32 pa-tients over 40 years of age were diagnosed with ASD
at Atatürk University Faculty of Medicine Depart-ment of Cardiovascular Surgery and Erzurum Re-gional Training and Research Hospital.
Twelve patients (37.5%) hospitalized for surgery consisted of 50 years of age and 4 patients over 60 years of age (12.5%). Twenty one of our patients (65.7%) were male and 11, female (34.3%). The first diagnosis was made by echocardiographic exami-nation in all patients. All of them were above 40 years of age and underwent coronary angiography in addition to cardiac catheterization. No significant changes were observed in the coronary arteries of any of the patients. The ratio of pulmonary to systemic blood flow (Qp/Qs) was determined by oximetry. The study patients had predominant left-to-right inter-atrial shunt with Qp/Qs of at least 1.5:1. In our cases, the mean Qp/Qs rate was between 1.5-2.0, 2.0-3.0, and ≥3.0 in 9 (28.1%), 19 (59.4%), and 4 (12.5%) patients, respectively.
Additional cardiac pathologies such as severe co-morbid disease, previous cardiac surgery, congeni-tal cardiac malformation, rheumatic valve disease, coronary artery disease at diagnosis, mitral or aortic regurgitation, and left ventricular dysfunction were not included in this study. The patients were eval-uated clinically and echocardiographically during the follow-up period of 2.2 years.
Surgical closure of atrial septal defect
CorSalud 2019 Jan-Mar;11(1):46-53 48
- Mild PHT: pulmonary artery pressure (PAP)
be-low 50 mmHg (n=16, 50%)
- Moderate PHT: PAP between 50 and 75 mmHg
(n=12, 37.5%)
- Severe PHT: PAP greater than 75 mmHg (n=4,
12.5%)
Functional capacity (as Class I, II, III, IV according to New York Heart Association [NYHA]), diuretic requirements and rhythm changes were analyzed according to preoperative period in order to eval-uate the efficacy of surgical treatment. Eighteen pa-tients (56.3%) were in Class I and II, and 14 were in Class III and IV groups (43.7%). In addition to the right atrium and right ventricular diameters of the patients, PAPs and left ventricular ejection fraction were re-evaluated after the operation and compared with the preoperative results.
All operations were performed under cardiopul-monary bypass and body temperature between 32-36 °C. Twenty seven patients (84.4%) underwent median sternotomy and 5 (15.6%), right thoracoto-my. Cold crystalloid cardioplegic solution was given to the aortic root for myocardial protection.
The size of the defect was evaluated after right atriotomy, and tricuspid valve insufficiency was tested. After the defect was closed with primary or
patch (pericardial or dacron) (Figure 1), patients
with advanced tricuspid regurgitation were treated with De Vega annuloplasty.
Early postoperative evaluation was made in the first month after surgery. Later, all patients were followed-up each 3 months to 3.1 years (mean, 2.2 years) by questionnaire or telephone interview with the patient or the referring physician, or both. All patients were advised to appear for clinical and echocardiographic follow-up evaluations at 6- or 8-month intervals, or as soon as possible if either a new symptom appeared or the previous clinical state deteriorated.
Statistical analysis
Statistical analysis was performed with SPSS 10.0 (SPSS, Chicago, IL, USA). All results are expressed as mean ± standard deviation. Kolmogorov-Smirnov test was used for variable data. Paired t tests were used to compare echocardiographic parameters in pre- and postoperative patients. McNemar tests were used to compare diuretic application, rhythm status, and functional capacity of all patients before and after surgery. P value <0.05 was considered signifi-cant.
RESULTS
The analysis included 32 patients who underwent surgical repair of secundum ASD; 11 women (34.3%) and 21 men (65.7%), with a mean age of 46±9 years
Figure 1. Two patients who underwent surgical closure of ASD. Operation images of patients in whom dacron
(range, 40 to 72 years). The ASD diameter was 1.5 to 3.8 cm (mean; 2.1±0.8 cm). Its size distribution is
shown in figure 2.
ASD was closed with direct suture in 5 patients (9.8%). Pericardial patch (19 patients) or dacron patch (8 patients) were preffered for defect closure in other patients. During the sewing process, contin-uous sewing technique (with 4/0 or 5/0 prolene ma-terial) was used.
All of the patients survived after the operation. The functional capacities of the patients showed a significant improvement after the operation. While the number of patients in Class I and II increased, the number of patients in Class III and IV decreased (Table). Twenty-two patients (68.8%) had received diuretic treatment before the operation, whereas only 9 patients (28.1%) received diuretic treatment after the operation. The number of patients using diuretics significantly decreased and this result was statistically significant (p<0.005).
In the preoperative term, 7 patients (21.9%) had atrial fibrillation (AF). Left ventricular ejection frac-tion was <45% in 9 patients (28.1 %), and over 45% in the rest. The right atrial diameters (RADs) were <45 mm, 45-55 mm, and >55 mm in 7 (21.9%), 16 (50%), and 9 patients (28.1%), respectively. The right ventricle diameters (RVDs) were <30 mm, 30-50 mm, and >50 mm in 6 (18.7%), 20 (62.6%), and 6 patients
(18.7%), respectively. The mean of the RADs and the RVDs were 48.5±6.7 and 36.9±8.4 mm, respectively, before the operation. While the highest RAD was 57 mm, the highest RVD was 46 mm among patients. The values of left ventricular ejection fraction, RAD, RVD, and PAP before and after the operation are
shown in table. RADs and RVDs were significantly
decreased after the operation (p<0.005). The RADs were much smaller than 50 mm in 24 patients. Tele-cardiography showed significant improvements in pulmonary vascularity and reduction in the size of
Table. Comparison of preoperative and postoperative data (echocardiographic variables and clinical parameters).
Parameters Preoperatively Postoperatively P value
Functional capacity (NYHA)
Class I 8 14 0.005
Class II 10 15 0.005
Class III 9 2 0.005
Class IV 5 1 0.005
Diuretic usage 22 9 0.005
Atrial fibrillation 7 6 0.801
Ejection fraction (%)
≤ 45 9 7 0.522
> 45 23 25 0.129
Right atrial diameter (mm) 48.5 ± 6.7 41.9 ± 4.1 0.005 Right ventricule diameter (mm) 36.9 ± 8.4 30.7 ± 7.8 0.005 Pulmonary artery pressure (mmHg) 47.2 ± 11.1 37.8 ± 10.9 0.005
Statistical significance: p<0.05
Surgical closure of atrial septal defect
CorSalud 2019 Jan-Mar;11(1):46-53 50
the right ventricle. The PAPs were significantly de-creased after the operation (p<0.005). PAPs were more than 60 mmHg in only 2 patients. Although the number of patients with left ventricular ejection fraction above 45% increased in the postoperative period compared to preoperatively, this result was not statistically significant (p=0.129).
Preoperative echocardiography revealed moder-ate or severe tricuspid regurgitation in 15 patients (46.9%). It was trivial in 3 (9.3%) patients. Water com-puted test was performed peroperatively in patients with moderate and advanced tricuspid regurgitation. De Vega annuloplasty procedure was performed in 11 patients (34.4%) with advanced leakage. Postop-eratively, only 2 patients had mild tricuspid regurgi-tation. Patients with tricuspid annuloplasty by De Vega’s method did well during the follow-up period.
One patient (3.1%) had mitral regurgitation re-lated to mitral cleft and mitral valvuloplasty was performed. Another patient (3.1%) had anomalous pulmonary venous connection, which was treated with ASD. Ten patients (31.2%) had aortic regurgi-tation that was not clinically significant.
The percentage of patients with AF decreased after operation (from 21.8% to 18.7%), but this
differ-ence was not significant (Table). Although 2
pa-tients recovered normal sinus rhythm after the operation, 1 of them had new AF in the postopera-tive term. To prevent thromboembolic complica-tions, anticoagulation therapy was started immedi-ately after the re-moval of the thoracic drainage tubes in 5 patients with AF.
Late follow-up
Twenty-nine patients were followed from 3 months to 3.1 years (mean 2.2 years). Two patients were lost to follow-up after moving to another city in Turkey, and another died in a traffic accident. Twenty-nine patients were class I or II in the mid-term follow-up. Three patients returned to normal sinus rhythm in the second year of follow-up. Late arrhythmias did not develop in any patients. Anticoagulant therapy was continued in patients because of continued AF. Advanced mitral valve regurgitation was detected in 1 patient after the operation. Mitral regurgitation, caused by bileaflet mitral valve prolapse was de-tected; mitral valve replacement was performed 2 years after the initial operation. Tricuspid regurgita-tion occurred in 1 patients with De Vega annulo-plasty, who was medically treated.
DISCUSSION
Surgical repair interventions for ASD have been successfully performed in many centers for more than 40 years. Perioperative morbidity and mortality rates were 10-20% at the end of the 1950s, these rates decreased to 6% after the 1960s, and up to 0.5%
now-adays6. This improvement in surgical success and
survival rates, and reduction in complications, are due to better operative techniques and better post-operative care. Therefore, the surgical closure of this very common congenital disease has recently been recommended at higher rates, even for older pa-tients. Despite successful and low complication operations, several studies have been published in the last few years that question the policy of routine
surgical closure in patients with high PAP5,7-10.
Surgical repair is still the main therapy for ASDs. The previous belief that only 50% of patients with unrepaired ASDs survive beyond the age of 40 years and less than 10% reach the age of 60 years, has not been confirmed in many other observational
stud-ies2,6. Therefore, life expectancy of patients with
untreated ASD is generally shortened1,4,9,11-13. In
par-ticular, when symptoms develop, it has been sug-gested that patients who are surgically treated have a significant survival advantage –compared to the medical treatment– similar of patients who were
operated in their second and third years7. Since AF,
pulmonary blood flow, right heart overload, ar-rhythmias and frequency of PHT tend to increase with age, ASD should be operated even if the patient is asymptomatic.
In the late follow-up period, age was found to be an important, meaningful and independent predictor
of morbidity and mortality2. Murphy reported that
patients undergoing surgery after age 40 had a high-er risk of postophigh-erative cardiovascular complica-tions and an excellent prognosis in children and
young adults12. Some of the patients we underwent
surgical correction were over 50 or 60 years old. No morbidity or mortality was found in these patients. Our results suggest that surgical closure of ASDs im-proves symptoms and prevents later complications in these patients. The proportion of patients with NYHA class III-IV decreased from 43,8% to 9,3% postoperatively. This result was found to be con-sistent with the results in the other published
ar-ticles7,14. These investigators reported that surgical
Studies have shown that the frequency of AF in
patients with ASD increases as age increases1,7,8,12. In
addition, the causes of atrial rhythm disorder were found to be induced by different mechanisms in the preoperative and postoperative periods. Before
surgery, the main cause of AF is atrial distension15.
Although the exact mechanism is not known, AF development in patients after ASD closure may be considered in relation to scarring in the area of ectopic focus or in the area of venous cannulation at the surgical repair site. Right atrial size decreased from 48.5±6.7 to 41.9±4.1 mm in our patients after the operation, and one the patients with AF returned to sinus rhythm, postoperatively. But, this was not statistically significant. Furthermore, in this case, it showed us that the ASD closure should be per-formed before the occurrence of AF.
Embolization in the postoperative period in pa-tients treated surgically is important for long-term hospitalization, cerebral injury and hospital ex-penses. This incidence is closely related to the age and the rhythm problems of the patient at the
opera-tion stage15. AF is a possible cause of an increased
incidence of thromboembolic events in patients
operated on to correct ASD14-16. Because of the high
risk of cerebral embolism in elderly patients with chronic AF, we preferred to begin anticoagulant therapy (warfarin) in patients with AF after surgery. We also aimed to reduce the risk of patch-related thromboembolism in small ASD patients by direct suture. Because of the necessity of patching in large defects, we used pericardial patch instead of dacron patch because of thromboembolic predisposition.
Although routine anticoagulant therapy was not
recommended after patch closure of ASD7, warfarin
was administered to patients with chronic AF in the postoperative period and aspirin treatment was started in the other patients. The INR value was kept between 2.5-3.5 in patients treated with warfarin. We suggested that aspirin therapy should be continued for at least 3 months in patients without AF accord-ing to the recommendations in the current
publica-tions16-18. No thromboembolic complication was seen
in the postoperative period and follow-up in our patients with AF. This showed that despite being AF, anticoagulant therapy prevented possible embolic
events. According to Shah et al9, the incidence of
systemic emboli was reported in ASD patients treated both medically and surgically; therefore, af-ter closure of ASDs, careful monitoring of arrhyth-mias and anticoagulants were recommended to prevent thromboembolic events.
The associated incidence of tricuspid regurgi-tation increases with age. In this study, moderate or severe tricuspid regurgitation was detected in 46,9% of the patients. Echocardiographic examination of the tricuspid valve sometimes has a tendency of overestimation. If preoperatively it shows moderate or severe signs of tricuspid regurgitation in patients, water proficiency testing is recommended to decide on tricuspid annuloplasty indication. In addition to ASD closure in these patients, we suggest that a tricuspid annuloplasty is important in decreasing cardiothoracic ratio, improving functional capacity and providing normal sinus rhythm.
PHT is a serious complication that affects the prognosis of ASD. In general, severe PHT associated with ASD is rare. But rarely, it can often develop at an advanced age (between 30 and 40 years of age), progressing rapidly to reverse shunting and causing
death17,18. It is difficult to predict in which patient
with ASD pulmonary vascular disease will develop. In patients with severe PHT, the operation of ASD is
very difficult and dangerous. Fiore and colleagues7
reported that the operative outcome in their series of ASD patients older than 50 years was not in-fluenced by the presence of PHT in the absence of greatly increased vascular resistance. Others have suggested that increases in PAP are not necessarily related to age, and shunt size is not related to
severity of symptoms17,18. Surgery should indeed be
performed in the younger patient and probably before structural changes in the myocardium or
pulmonary vasculature have occurred19. Despite
rare severe PHT in our patients, we suggest that, in patients with PHT, surgeons should be cautious in deciding to operate, irrespective of their age.
The advanced NYHA classification had a pro-nounced impact on early and late mortality. We found a significant improvement in functional status that the rate of patients with class I and II was in-creased from 56,2% to 90,6% after surgical treatment (Table).
Surgical closure of atrial septal defect
CorSalud 2019 Jan-Mar;11(1):46-53 52
devices), we believe that anatomic closure must be performed without delaying the initial treatment for ASD with a Qp/Qs ratio ≥ 1.5 and increasing PAP for adults > 40 years old, even these over 60 years of age, who are in NYHA classes III and IV. Patients who are surgically treated should be closely moni-tored for AF or atrial flutter to prevent or reduce the morbidity and mortality associated with cerebral thromboembolism, and the anticoagulation regimen should be maintained in patients with persistent AF even if the patients were operated.
CONCLUSIONS
Surgical closure of atrial septal defects in adult pa-tients over the age of 40 can improve cardiac func-tion by echocardiography and reduce clinical com-plaints. Even if no intervention is made in such patients, the current complaints are scarce and life-threatening problems are rarely seen in hemody-namic parameters. However, surgical repair should be performed as soon as possible, especially when detected in adult patients.
REFERENCES
1. Jiang H, Wang ZW, Zhu HY, Zhang RF, Gong HD,
Wang HS, et al. Surgical treatment of secundum atrial septal defects in adults over 30 years old. Zhonghua Wai Ke Za Zhi. 2004;42(16):961-4.
2. John Sutton MG, Tajik AJ, McGoon DC. Atrial
sep-tal defect in patients ages 60 years or older: oper-ative results and long-term postoperoper-ative follow-up. Circulation. 1981;64(2):402-9.
3. Burke RP, Horvath K, Landzberg M, Hyde P,
Col-lins JJ, Cohn LH. Long-term follow-up after surgi-cal repair of ostium primum atrial septal defects in adults. J Am Coll Cardiol. 1996;27(3):696-9.
4. Attie F, Rosas M, Granados N, Zabal C, Buendía
A, Calderón J. Surgical treatment for secundum atrial septal defects in patients >40 years old. A randomized clinical trial. J Am Coll Cardiol. 2001; 38(7):2035-42.
5. Konstantinides S, Geibel A, Kasper W, Just H. The
natural course of atrial septal defect in adults - a still unsettled issue. Klin Wochenschr. 1991; 69(12):506-10.
6. Konstantinides S, Geibel A, Olschewski M,
Gör-nandt L, Roskamm H, Spillner G, et al. A compari-son of surgical and medical therapy for atrial
sep-tal defect in adults. N Engl J Med. 1995;333(8):469-73.
7. Fiore AC, Naunheim KS, Kessler KA, Pennington
DG, McBride LR, Barner HB, et al. Surgical clo-sure of atrial septal defect in patients older than 50 years of age. Arch Surg. 1988;123(8);965-7.
8. Cheng TO. The natural course of atrial septal
de-fect in adults - a still unsettled issue. Clin Investig. 1992;70(1):85.
9. Shah D, Azhar M, Oakley CM, Cleland JG,
Niho-yannopoulos P. Natural history of secundum atrial septal defect in adults after medical or sur-gical treatment: a historical prospective study. Br Heart J. 1994;71(3):224-7.
10.Perloff JK. Surgical closure of atrial septal defect
in adults. N Engl J Med. 1995;333(8):513-4.
11.Driscoll D, Allen HD, Atkins DL, Brenner J,
Dun-nigan A, Franklin W, et al. Guidelines for evalua-tion and management of common congenital cardiac problems in infants, children, and adoles-cents. A statement for healthcare professionals from the Committee on Congenital Cardiac De-fects of the Council on Cardiovascular Disease in the Young, American Heart Association. Circula-tion. 1994;90(4):2180-8.
12.Murphy JG, Gersh BJ, McGoon MD, Mair DD,
Porter CJ, Ilstrup DM, et al. Long-term outcome after surgical repair of isolated atrial septal defect. Follow-up at 27 to 32 years. N Engl J Med. 1990; 323(24):1645-50.
13.Brickner ME, Hillis D, Lange RA. Congenital heart
disease in adults. First of two parts. N Engl J Med. 2000;342(4):256-63.
14.Shibata Y, Abe T, Kuribayashi R, Sekine S, Seki K,
Yamagishi I, et al. Surgical treatment of isolated secundum atrial septal defect in patients more than 50 years old. Ann Thorac Surg. 1996;62(4): 1096-9.
15.Chatzis A, Giannopoulos N, Vahlas C, Milonakis
M, Contrafouris C, Bobos D, et al. Surgical treat-ment of the atrial septal defect in adults: effective reduction in cardiac size and excellent overall clinical outcome. Rev Port Cir Cardiotorac Vasc. 2006;13(3):133-6.
16.Horvath KA, Burke RP, Collins JJ, Cohn LH.
Sur-gical treatment of adult atrial septal defect: early and long-term results. J Am Coll Cardiol. 1992; 20(5):1156-9.
17.Hörer J, Müller S, Schreiber C, Kostolny M,
failure. Thorac Cardiovasc Surg. 2007;55(2):79-83.
18.Shaheen J, Alper L, Rosenmann D, Klutstein MW,
Falkowsky G, Bitran D, et al. Effect of surgical repair of secundum-type atrial septal defect on right atrial, right ventricular, and left ventricular volumes in adults. Am J Cardiol.
2000;86(12):1395-7.
19.Ghosh S, Chatterjee S, Black E, Firmin RK.