Please cite this article in press as: Qui˜nonez-Olivas CG, et al. Muscle mass measured using bioelectri-www.elsevier.es/rmuanl
ORIGINAL
ARTICLE
Muscle
mass
measured
using
bioelectrical
impedance
analysis,
calf
circumference
and
grip
strength
in
older
adults
C.G.
Qui˜
nonez-Olivas
a,∗,
R.
Salinas-Martínez
a,
X.A.
Ortiz-Jiménez
b,
D.G.
Gámez-Trevi˜
no
a,
G.
Guajardo-Álvarez
a,
B.
González-García
aaGeriatricServicesatthe‘‘Dr.JoséEleuterioGonzález’’HospitalUniveristariodelaUniversidadAutónomadeNuevoLeón,
NuevoLeón,Mexico
bSchoolofPsychology,UniversidadAutónomadeNuevoLeón,NuevoLeón,Mexico
Received4March2016;accepted7June2016
KEYWORDS Muscle; Gripstrength; Calfcircumference
Abstract
Objective: Todeterminethecorrelationbetweenmusclemass,measuredusingbioelectrical impedanceanalysis(BIA),withcalfcircumferenceandgripstrength.
Materialsandmethods: Cross-sectionalandobservationalstudy.Includingallfunctionaladults over60 yearsofageseeninourGeriatricClinicduringthemonthsofMarch2013---February 2014.Measurementsofweight,height,BMI,calfcircumference,gripstrengthandmusclemass byBIAweremadeafterthesignatureofinformedconsent.
Results:105patients wereevaluated,73 womenand32 men,withameanageof76years (SD±7.3).Musclemassshowedamildpositive correlationwithcalf circumference:Pearson (r=0.31;p=0.000)andamoderatepositivecorrelationwithgripstrength:Pearson(r=0.50; p=0.000).
Discussion: Muscle massby BIA has apositive correlation with calf circumference andgrip strength,andisareliablemeasuretoassessmusclemassandphysicalperformanceinolder adultsingeriatricambulatoryclinicsandcanbeusedinthediagnosisofsarcopeniainMexican patients.
©2016UniversidadAut´onomadeNuevoLe´on.PublishedbyMassonDoymaM´exicoS.A.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
∗Correspondingauthorat:ServiciodeGeriatría,HospitalUniversitario‘‘Dr.JoséEleuterioGonzález’’,UniversidadAutónomadeNuevo León,ColoniaMitrasCentro,AvenidaGonzalitosyMaderoenMonterrey,NuevoLeón,Mexico.Tel.:+528181232436.
E-mailaddress:[email protected](C.G.Qui˜nonez-Olivas).
http://dx.doi.org/10.1016/j.rmu.2016.06.005
1665-5796/©2016UniversidadAut´onomadeNuevoLe´on.PublishedbyMassonDoymaM´exicoS.A.Thisisanopenaccessarticleunderthe
Please cite this article in press as: Qui˜nonez-Olivas CG, et al. Muscle mass measured using
bioelectri-Introduction
Therelationbetweenmusclemassandaginghasled scien-tiststoinvestigate itschanges,causes andconsequences. Initially,IrwinRosenbergproposedtheterm‘‘sarcopenia’’ in 1989(from theGreek ‘‘sarx’’ or ‘‘meat’’+‘‘penia’’ or ‘‘loss’’)todescribethedecreaseofmusclemassrelatedto age.1 Since itsdefinition, authors have demonstratedthe absolute loss of muscle mass from the age of 50, witha decreaseof1.1and1.9kgperdecadeformanandwomen, respectively.2
Epidemiological studies of sarcopenia, with more rep-resentative samples from Europe and the U.S., show prevalencefigureswhichrangefrom10%inadultsolderthan 60upto60%inadultsolderthan80.3,4
In 2010, the European Working Group on Sarcopenia in Older People (EWGSOP)5,6 aided studies by Baumgart-ner,etal.andJanssen etal.tocreatediagnosticcriteria. TheyuseddualenergyX-rayabsorptiometry(DEXA)and bio-electricalimpedanceanalysis(BIA)todeterminemuscular mass.6---8 The EWGSOP’s final intended resultwasan algo-rithm for sarcopenia that fulfilled the following criteria: lowphysicalperformancemeasuredbywalkingspeed(4m course)and/or decreasedgripstrength,plusacriterionof lowmuscularmassbelowthestandarddeviations,tomake adefinitivediagnosis.6,9
In Mexico, the public health care system does not havethenecessary toolstomeasuremuscularmass.Thus, dynamometryhasbeenwidelyusedtoevaluategripstrength andphysical performance in older adults.10 Gripstrength is a predictive factor of adverse results such as institu-tionalization or mortality, but is limited in patients with deterioratedcognitiveability, duetothedifficultiesin its executionor alackofmotivation.11 Anthropometric meas-uressuchascalfcircumference(CC)havealsobeensought asawaytomeasuremuscularmassandfunctionality,based principallyonastudyby Rollandetal.whodemonstrated thatolder adultswitha CCof less than31cmhada high specificity(91%)inasarcopeniadiagnosis,andwere associ-atedwithdisabilityintheactivitiesoftheirdailylives.12
Arangoetal.intheCoyoacancohort,alsousedaCCless than31cmtoestimatesarcopeniaprevalence.13 However, itisimportanttoconsiderthananthropometricssuchasCC arepronetoerrorduetoadiposedepositsinmusclefibers andlossofskinelasticityinolderadults,whichcancausean underestimationinsarcopenia’sprevalenceinpersonswith obesity.14
Bioelectricalimpedanceanalysis(BIA)is areproducible methodtomeasurebody composition,andhas been used topredictmusclemassdecreasesinolderadults.However, therelimitations,suchashydrationstate,inadequate pro-teiningestionandphysicalcondition.Despitethis,BIAcould be a useful tool to measure muscular mass in the Mex-ican population, with a lower cost compared to imaging studiesanda decreaseinlimitations comparedtoCCand grip strength in patients with obesity, depression or cog-nitive deterioration,which arecommonsyndromes in the olderly.15---17
The objective of this study is to determine the rela-tionbetweenmuscular massmeasured byBIA andCCand gripstrengthintheolderadultpopulationofNortheastern Mexico.
Material
and
method
Design
This was a transversal study in Monterrey, Nuevo León between March 2013 and February 2014 in the ambula-tory populationof olderadultsthatcametotheGeriatric Services at the ‘‘Dr. José Eleuterio González’’ University Hospital of the AutonomousUniversity of Nuevo Leónfor theirfirstconsultation.
Population
Anon-probabilisticsamplewasusedforthisstudy,included allpatientswhichcameforaconsultationduringthestudy’s timeperiod. The totalsample size of thosewhocame to theirconsultation betweenMarch2013andFebruary 2014 was283.
Out of these 283 patients, we selected 105 that met theinclusioncriteria,whichwere:independetintheirbasic dailylivingactivities,withKatzindex≥5.Weexcludedany patientwithanarticularprosthesisorosteosynthesis,useof pacemakers,hormonereplacementtherapywithandrogens, growthhormoneor steroiduse inthepast yearandother chronicoracuteseverecomorbiditythatcausecachexia(or secondarysarcopenia)duetothecatabolicdiseaseprocess itself,suchasNYHAIIIheartfailure,chronicobstructive pul-monarydiseaseGOLDCorD,chronicliverdiseaseCHILDBor Cand/orstage5chronickidneydisease(Terminaldisease). ThestudywasapprovedbytheEthicsandResearch Com-mittee of the ‘‘Dr. José Eleuterio González’’, University HospitalwiththecodenumberGE12-001.
Instruments
A routine clinical service case history, including relevant pathologicalhistory andclinimetry,composedofscales of functionandcognitivestatus,wasperformed.
Toevaluatethefunctionality,weusedtheBasicActivity ofDailyLivingIndex,developedbyKatzetal.18and Lawton-Brody’sof InstrumentalActivities of DailyLifeIndex.19 To evaluatecognitivestate, weappliedtheMini-MentalState Examination(MMSE)developedbyFolsteinetal.20 andthe GeriatricScaleofDepression(GDS)byYesavageetal.21was usedtoevaluatestateofmind.Theanthropometrywas reg-isteredusingweight,height,bodymassindex(BMI)andcalf circumference(CC).
Gripstrengthofthedominanthandwasdeterminedwith a Takei A5401 digital dynamometer (MedicalSystems Plus IndustryandCommerceMarketingCo.Ltd.,Besiktas Istan-bul,Turkey).Thismeasurementwasperformedthreetimes, withanintervalofoneminutebetweeneachmeasurement, andweusedtheaverageofthethreeresults.
Please cite this article in press as: Qui˜nonez-Olivas CG, et al. Muscle mass measured using
bioelectri-Table1 Clinimetricandanthropometriccharacteristics.
Variables Average(±SD)
Gender(%) 73M(69.5)/32(30.5)
Age(years) 76(±7.3)
Height(cm) 154(±9)
Weight(kg) 65.6(±13.9)
BMI(kg/m2) 27.5(±5.2)
Gripstrength(kg) 20.86(±7.9) Calfcircumference(cm) 34.3(±4.1) Muscularmass(kg) 12.98(±4.6)
KATZ(points) 5.8(±0.35)
Lawton-Brody(points) 5(±1.90)
MMSE(points) 23.0(±5.20)
GDS(points) 4.0(±3.50)
The tetrapole bioimpedometer (BIA Quantum IV Body CompositionAnalyzer,RJLsystems)evaluatesthebody tis-sue’s resistance to an electric current. The analysis was performedwiththepatientlyingdown,withfourattached electrodes,twoonthebackofthewristandtwoontheright ankle.Theresultsarepresentedasresistanceandreactance inohms, tolaterbeusedin oneofthevalidmusclemass (MM) estimationequations. We used a formuladeveloped byJanssenetal.7
Musclemass(kg)=[(height2/R×0.401)+(3825×gender) +(age×−0.071)]+5.102.
Height=cm,R=resistanceinohmsmeasuredbytheBIA. Gender=male:0,female:1.
Statisticalanalysis
Descriptive statistics were performed and expressed as mean and standard deviation (SD) for all variables and means of analysis werecompared between both genders. The normality of the variables was analyzed using the Kolmogorov---Smirnovtest.APearsoncorrelationcoefficient analysis was performed to calculate the association of quantitativevariables.Thevaluesofp=0.05orlesswas con-sideredstatisticallysignificant.Allanalyzeswereperformed usingSPSSforWindows(SPSSInc.,Chicago,IL,version20.0).
Results
Theseresultsarefromthetotalsampleof105patients,73 women(69.5%)and32men(30.5%)whohadanaverageage of76(±7.3)years.
Overall means of instruments, clinimetric evaluations andanthropometriccharacteristicssuchastheKatzIndex, Lawton-Brody,MMSE,GDS,weight,height,BMI,calf circum-ference, grip strength and muscle mass are described in
Table1.
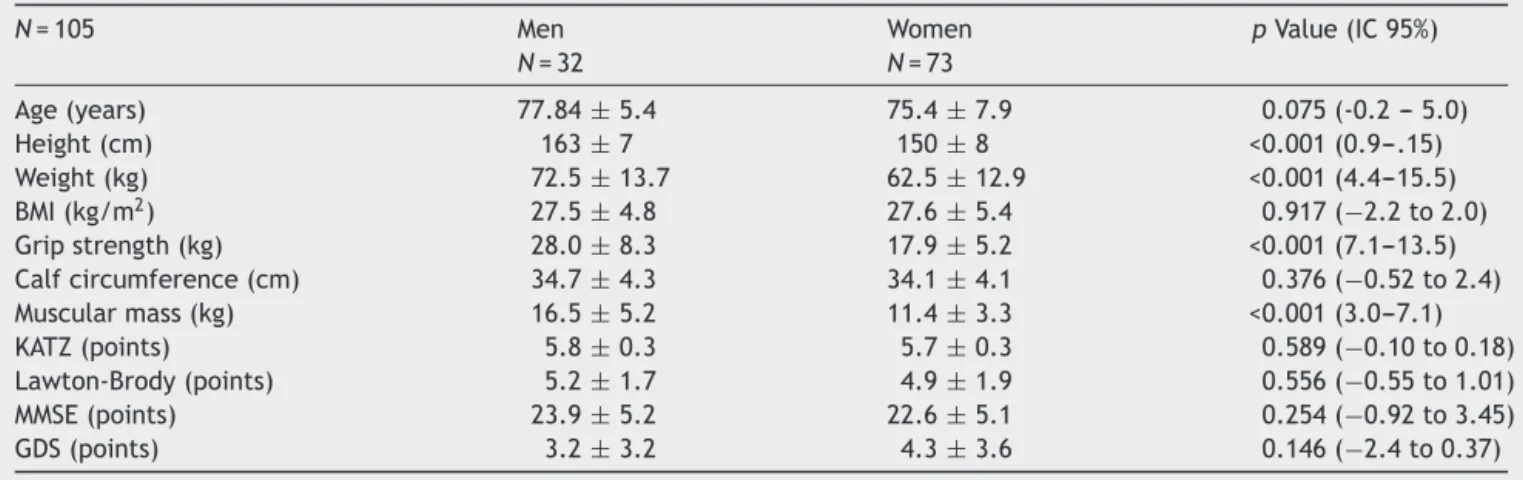
Intheanalysisbygender,menhadhighervalues, show-ingstatisticallysignificantdifferencesinmeanmusclemass andgripstrength,which wasexpectedduetotheirlarger sizeandweight,buttherewerenosignificantdifferencesin calfcircumference,showingthelowsensitivityofthecalf muscleasabiomarkerofsarcopenia(Table2).
Finally,a slightpositivecorrelation wasfoundbetween muscle mass by BIA and calf circumference (p=<0.001
45
r=0.312
40
35
30
25
0 5 10 15 20 25 30 35
Figure1 The resultofthe Person’s association testwas a slightpositivecorrelationbetweenmusclemassbyBIAandcalf circumference,r=0.312(p=<0.001).Muscularmass(kg).Calf circumference(cm).
50
r=0.505
40
30
20
10
0
0 5 10 15 20 25 30 35
Figure2 The resultofthe Person’s association testwas a moderatepositivecorrelationbetweenmusclemassbyBIAand gripstrength,r=0.505(p=<0.001).Gripstrength(kg).Muscular mass(kg).
is=0.31),aswellasamoderatepositiveassociationbetween muscle mass and grip strength (r=0.50, p=<0.001) and calfcircumference and grip strength (r=0.28, p=<0.001)
(Figs.1---3).
Discussion
Please cite this article in press as: Qui˜nonez-Olivas CG, et al. Muscle mass measured using
bioelectri-Table2 Clinicalcharacteristicsbygender.
N=105 Men
N=32
Women N=73
pValue(IC95%)
Age(years) 77.84±5.4 75.4±7.9 0.075(-0.2---5.0)
Height(cm) 163±7 150±8 <0.001(0.9---.15)
Weight(kg) 72.5±13.7 62.5±12.9 <0.001(4.4---15.5)
BMI(kg/m2) 27.5±4.8 27.6±5.4 0.917(−2.2to2.0)
Gripstrength(kg) 28.0±8.3 17.9±5.2 <0.001(7.1---13.5)
Calfcircumference(cm) 34.7±4.3 34.1±4.1 0.376(−0.52to2.4)
Muscularmass(kg) 16.5±5.2 11.4±3.3 <0.001(3.0---7.1)
KATZ(points) 5.8±0.3 5.7±0.3 0.589(−0.10to0.18)
Lawton-Brody(points) 5.2±1.7 4.9±1.9 0.556(−0.55to1.01)
MMSE(points) 23.9±5.2 22.6±5.1 0.254(−0.92to3.45)
GDS(points) 3.2±3.2 4.3±3.6 0.146(−2.4to0.37)
50
40
30
20
10
0
25 30 35 40 45
Figure3 The resultofthe Person’s association test was a slightpositivecorrelationbetweencalfcircumferenceandgrip strength,r=0.288(p=<0.001).Gripstrength(kg).Calf circum-ference(cm).
calfcircumference showed nostatistically significant dif-ferencebetweenwomen andmen,suggestingalimitation withthisformof measurement indiscriminating between musclemass,water,fatandbone,likeallanthropometric measurements.22 This is consistent with a study by Rol-land,etal.whichshowedthatacalfcircumferencelower than 31cm had high specificity but low sensitivity 44% in thepredictionof sarcopenia,limitingitsuseindiagnosing sarcopenia.12
BIA has been studied for over 10 years andhas a high positive correlation (r=0.095) with MRI, which is consid-eredthegoldstandardformeasuringmuscularmass.16 Our studysupportstheuseofBIAtomeasuremusclemasswith greaterreliabilitythancalfcircumferenceandalsoasatool toindirectlymeasurepatients’physicalperformancedueto thepositiveassociationwithgripstrength.Thereare stud-ieswhichshow thatthe lowergrip strengthincreasesthe
relativeriskofdisabilityinactivitiesinvolvedwithdaily liv-ing to 2.0 (95% CI 1.14---3.17). These have also shown an associationwithsarcopenia,withariskincreaseof4.8(95% CI1.4---16.8).9,23ThemeasurementofmusclemassbyBIAis particularlyrelevantinpatientswithdepressionand/or cog-nitiveimpairmentthatcannotcarryoutothermeasuresof forceorphysicalperformanceproperly.
Thelimitationofthisstudywasthesmalland unrepresen-tativesamplesizeweusedtogeneralizethefindingsforall olderadultsinNortheasternMexico.Weneedmorestudies toexaminethereliabilityofthesetoolstomeasuremuscle massintheelderly.
Ethical
norms
This studywasapprovedbytheEthicsand Research Com-mittee of the ‘‘Dr. José Eleuterio González’’ Hospital Univeristario dela Universidad AutonomadeNuevo Leon, withthecodenumberGE12-001.
Funding
Property of the Geriatric Service of the ‘‘Dr. José Eleu-terio González’’ Hospital Univeristario de la Universidad AutonomadeNuevoLeon.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Acknowledgements
To Luis Miranda Plata and Carlos Beltrán García, social servicemedicalinternsattheGeriatricServiceofthe‘‘Dr. José EleuterioGonzález’’Hospital Univeristariodela Uni-versidadAutonomadeNuevoLeon.
References
Please cite this article in press as: Qui˜nonez-Olivas CG, et al. Muscle mass measured using
bioelectri-2.SayerAA,SyddallH,MartinH,etal.Thedevelopmentalorigins ofsarcopenia.JNutrHealthAging.2008;12:427---32.
3.BaumgartnerRN,KoehlerKM,GallagherD,etal.Epidemiology ofsarcopeniaamongtheelderlyinNewMexico.AmJEpidemiol. 1998;147:755---63.
4.Laurentani F, Russo C, Bandinelli S, et al. Age-associated changes in skeletal muscles and their effect on mobil-ity: an operational diagnosis of sarcopenia. J Appl Physiol. 2003;95:1851---60.
5.Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: Europeanconsensuson definitionand diagnosis. AgeAgeing. 2010;39:412---23.
6.Alexa ID, Ilie AC,Moros¸anu A, et al. Approaching frailtyas thenew geriatric syndrome.Rev Med ChirSocMed NatIasi. 2013;117:680---5.
7.JanssenI,HeymsfieldSB,RossR.Lowrelativeskeletalmuscle mass (sarcopenia) in older persons is associated with func-tional impairment and physical disability. J Am GeriatrSoc. 2002;50:889---96.
8.BurtonLA,SumukadasD.Optimalmanagementofsarcopenia. ClinIntervAging.2010;5:217---28.
9.Al Snih S, Markides K, Ottenbacher K, et al. Hand grip strengthandincidentADLdisabilityinelderlyMexican Amer-icansovera seven-yearperiod.AgingClinExpRes.2004;16: 481---6.
10.Stevens PJ, Syddall HE, Patel HP, et al. Is grip strength a good marker of physical performance among community-dwelling older people. J Nutr Health Aging. 2012;16: 769---74.
11.Alfaro-AchaA,AlSnihS,RajiMA,etal.Handgripstrengthand cognitivedeclineinolderMexican.JGerontolABiolSciMed Sci.2006;61:859---65.
12.Rolland Y, Lauwers V, Cournot M, et al. Sarcopenia, calf circumference,andphysicalfunctionofelderlywomen:a cross-sectionalstudy.JAmGeriatrSoc.2003;51:1120---4.
13.Arango-Lopera VE, Arroyo P, Gutiérrez-Robledo LM, et al. Prevalence of sarcopenia in Mexico City. Eur Geriatr Med. 2012;3:157---60.
14.Aleman Mateo H1, Lee SY, Javed F, et al. Elderly Mexicans havelessmuscleandgreater totaland truncalfatcompared toAfrican-AmericansandCaucasianswiththesameBMI.JNutr HealthAging.2009;13:919---23.
15.Roubenoff R1,BaumgartnerRN, HarrisTB, etal. Application ofbioelectrical impedance analysisto elderly populations.J GerontolABiolSciMedSci.1997;52:M129---36.
16.Janssen I,HeymsfieldSB,BaumgartnerRN,et al.Estimation ofskeletalmusclemassbybioelectricalimpedanceanalysis.J ApplPhysiol.2000;89:465---71.
17.ChienMY,HuangTY,WuYT.Prevalenceofsarcopeniaestimated usingabioelectricalimpedanceanalysispredictionequationin community-dwellingelderlypeopleinTaiwan.JAmGeriatrSoc. 2008;56:1710---5.
18.KatzS,StroudMW.Functionalassessmentingeriatrics:areview ofprogressanddirections.JAmGeriatrSoc.1989;37:267---71.
19.Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist.1969;9:179---86.
20.FolsteinM,FolsteinSE,McHughPR.‘‘Mini-MentalState’’a prac-ticalmethodforgradingthecognitivestateofpatientsforthe clinician.JPsychiatrRes.1975;12:189---98.
21.YesavageJA,BrinKTL,RoseTL,etal.Developmentand vali-dationofageriatricdepressionscale:apreliminaryreport.J PsychiatRes.1983;17:37---49.
22.HughesVA,RoubenoffR,WoodM,etal.Anthropometric assess-mentof10-ychangesinbodycompositionintheelderly.AmJ ClinNutr.2004;80:475---82.