www.elsevier.es/rmuanl
SCIENTIFIC
LETTER
Case
report:
Diagnostic
reconceptualization
in
the
DSM-V
on
somatoform
disorders
D.
Ibarra-Patrón
∗,
G.
Medina-Vidales,
C.
Garza-Guerrero
DepartmentofPsychiatry,‘‘Dr.JoséEleuterioGonzález’’UniversityHospital,UANL,Monterrey,NuevoLeón,Mexico
Received26August2014;accepted11November2014 Availableonline6April2015
KEYWORDS
Somaticsymptoms disorder;
DSM-5; Classification; Evaluation; Diagnosis; Treatment
Abstract Psychosomaticdisordersareamongthemostcommonpsychiatricdisordersin gen-eral practice, with a prevalence of 16%. These patients often turn to different general practitionersand/ornon-psychiatricspecialistsforlongperiodsoftimeandrepresenta diag-nosticandtherapeutic challenge,as thepossibleorganiccomponentmakesitcomplexand difficulttomanage.
Thereportedcaseisa24-year-oldmalepatientwithadiagnosisofSomaticSymptomsDisorder andmultiplepsychiatriccomorbidities.Thepurposeofthisstudyistoreviewthe reconceptu-alizationofSomatoformDisorders’DSM-5diagnosis,whichcanbeusefulforpsychiatristsand non-psychiatricphysiciansfortheapproachandmanagementofthesepatients.
©2014UniversidadAutónomadeNuevoLeón.PublishedbyMassonDoymaMéxicoS.A.Allrights reserved.
Introduction
Psychosomaticdisordersareamongthemostcommon psy-chiatric disorders in general practice, with a prevalence of 16%.1---3,5 Before going to a psychiatrist,these patients usuallyseegeneralphysicians and/ornon-psychiatric spe-cialistsforlongperiodsoftime2,4,6whichisenabledbythese patients’ resistance to acknowledging that their physical
∗Correspondingauthorat:DepartamentodePsiquiatría,Hospital
Universitario‘‘Dr.JoséEleuterioGonzález’’,UANL,Av.FranciscoI
MaderoyGonzalitoss/n,ColoniaMitrasCentro,C.P.64460
Monter-rey,NuevoLeón,Mexico.Tel.:+528183480585.
E-mailaddress:[email protected](D.Ibarra-Patrón).
problemcan belinkedtoor exacerbatedby anemotional andnotonlyanorganicorigin,resultinginmultiple thera-peuticmanagementsandchronicuseofhealthservices.2,4,5,8 Moreover, the important association of psychiatric comorbidity (depression, anxiety and psychopathology of character),aswellasmedicalillnesses,1,2,4,6,7makesthema diagnosticandtreatmentchallengenotonlyforthe psychia-trist,butalsoforgeneralpractitionersandotherspecialties, sincethepossibleorganiccomponentmakesthemcomplex anddifficulttomanage.4,7
Regardingitsevolution,chronicity, social and interper-sonal dysfunction, difficulties at work and the frequent use of medical services are the common characteristics of these disorders, which lead to an elevated level of dissatisfaction in both the doctor and the patient.5,7,8
http://dx.doi.org/10.1016/j.rmu.2015.02.001
Thepresentarticlepresentsthecaseofapatientwho exem-plifiesthispathology.
Case
presentation
and
discussion
Thepatientisa24-year-oldmale,fromMonterrey,Mexico. Heissingle,worksatafleamarket,withanuppersecondary levelofcompletededucationandalowsocioeconomic sta-tus.Hehadabackgroundofexcellentschoolperformance with academic scholarship through secondary school and highschool.Priortotheonsetofthepsychopathology,there wasadequateandconstantwork activity,aswell asmore social,recreationalandinterpersonal involvement.During hischildhood,hereferstobeingsexuallyabused(improper touching)ontwooccasionsanddescribesastressingfamily environmentwithconstantverbalandpsychologicalabuse towardhimandotherfamilymembers.Thisprolongsuntil adolescence. Subsequent to his parents’ separation, he maintainsascarce,almostnull,relationshipwithhisfather, whichstandsasaneventwhichimpactshischildhoodand personaldevelopmentinanegativeway.
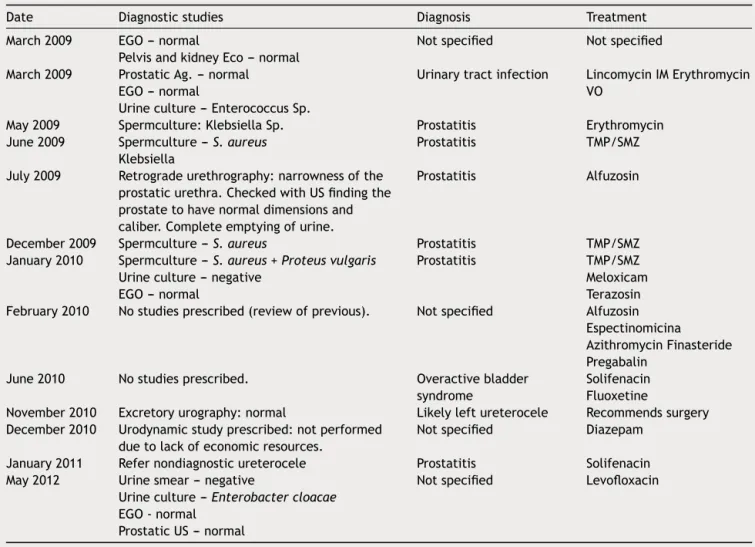
HehasattendedthePsychiatricOutpatientClinic volun-tarily on July 2012 after presenting depressive symptoms for more than 6 months, secondary to pollakiuria with an evolution of 4 years, which began after his father’s
death, presenting 20---25 urinations a day, with intervals of 10---20min in-between and without disrupting sleeping hours.He deniespainwhileurinating, pushing, tenesmus, fever or any other added symptoms. Over 4 years the patientsawmultipledoctorsanddifferenturologists,who requestedpara-clinicalstudies, withdifferent non-certain diagnosesanddiversepharmacologicaltreatmentswithout improvementsintheurinarysymptom.(Table1)
At first, in view of the diagnostic doubt and lack of responsetotreatments, thepatientthought thatthe ori-ginofthesymptom wascausedbyaphysicalillness;then, heassociateditwiththeunresolvedmourningofhisfather’s deathwhichconcurswiththeonsetofthesymptoms.
Secondary to the onset of the urinary symptom, the patient interrupts his personal and professional growth: quitshisjob,stopsfrequentinghisfriendsandremains iso-latedathomeforover2years,focusinghislifeonattending specialistsandtryingtosolvehissymptoms.Twoyearslater, thepatientreducesthefrequencyofurination, accomplish-ingaurinationrate ofonceevery2h, andbeginsworking part-time.However,thesenseofurgencytourinateaswell astheconstantpreoccupationofnotbeingabletoreacha placetourinate,leadtoapoorworkinggrowthand avoid-anceofinterpersonalrelationshipswithlimitedsocialand recreationalactivities.
Table1 Medicalhistoryinrelationtotheurinarysymptom.
Date Diagnosticstudies Diagnosis Treatment
March2009 EGO---normal
PelvisandkidneyEco---normal
Notspecified Notspecified
March2009 ProstaticAg.---normal EGO---normal
Urineculture---EnterococcusSp.
Urinarytractinfection LincomycinIMErythromycin VO
May2009 Spermculture:KlebsiellaSp. Prostatitis Erythromycin
June2009 Spermculture---S.aureus
Klebsiella
Prostatitis TMP/SMZ
July2009 Retrogradeurethrography:narrownessofthe prostaticurethra.CheckedwithUSfindingthe prostatetohavenormaldimensionsand caliber.Completeemptyingofurine.
Prostatitis Alfuzosin
December2009 Spermculture---S.aureus Prostatitis TMP/SMZ
January2010 Spermculture---S.aureus+Proteusvulgaris
Urineculture---negative EGO---normal
Prostatitis TMP/SMZ
Meloxicam Terazosin February2010 Nostudiesprescribed(reviewofprevious). Notspecified Alfuzosin
Espectinomicina AzithromycinFinasteride Pregabalin
June2010 Nostudiesprescribed. Overactivebladder
syndrome
Solifenacin Fluoxetine
November2010 Excretoryurography:normal Likelyleftureterocele Recommendssurgery December2010 Urodynamicstudyprescribed:notperformed
duetolackofeconomicresources.
Notspecified Diazepam
January2011 Refernondiagnosticureterocele Prostatitis Solifenacin May2012 Urinesmear---negative
Urineculture---Enterobactercloacae
EGO-normal ProstaticUS---normal
Six months prior to attending psychiatric consultation hebegins tofeelsadnessevery day for almostthe entire day; thissadness is linked tohis urinaryproblem and his difficultiesinaccomplishingthingsin hispersonallifeand at work. He refers to feeling ‘‘handicapped’’, saying he felt‘‘liketrash’’,occasionalcrying,anhedoniaand melan-choly.Amonthagohebegantopresentterminalinsomnia, reductionofappetite,weaknessandoccasionalfeelingsof hopelessness, causing significant discomfort which inter-feres with his performance in his everyday activities. He denieshavingthoughtsofdeath,orsuicidalthinkingand/or planning.
Previoustothe pollakiuria,a patternof preoccupation abouttrivialsituationswithatendencyforthecatastrophic is noticed, which causes a persistentand general anxiety notlimitedtoaspecificsituationandismanifestedby con-stanthandsweating,palpitations,mildtremors,occasional irritability,fatigueanddifficultyfocusing.Theanxiety symp-tomsfluctuate,buthavealongevolution,whichhasbeen exacerbatedoverthelast6months.
Structural
exam
The patient manifests evasive and dependent behavior, whichhashadhim workingfor thelast2yearsata place whichdoesnotrepresentasignificantchallengenordoesit demandformalobligations,hidingbehindhisurinary prob-lem to avoid looking for a stable job, with a dependent andvictimizedline.Theevasivebehaviorisalsomanifested byhisdisproportionalfearwhenfacingeverydaysituations, generating anguish and resulting in deterioration of work andinterpersonalrelations.
He presents a predominately devaluated self-concept, describinghimself asscared,insecureandfeelingthat he haslittlevalue;thisinterfereswithhisinterpersonal rela-tionships with others. He displayed defense mechanisms, mainlyrepressive,likerationalization,constantlyusinghis urinary symptom as an excuse to justify his evasive and dependent traits; affective isolation when describing his father’sdeathasaneventthatcaused littlepainand dis-placing,redirectingthatpaintowardhisurinarysymptom.
Despite his difficulty torelate to others, hemanifests an ability to empathize with others and an ability to be grateful,expressinggratitudeforthetimededicatedtohis evaluation.Regarding hisaggressive impulses’control, he doesnotpresentfrequentsituationswhichputhimin con-flict,thusmakinghisabilitytocontainandrepressemotions evident.However,onafewoccasionswewereabletosee theinfiltrationofprimaryprocessthinking,causing himto make impulsive decisions, later realizing this through his abilityforself-reflexivethinking.
In respect to the quality of his interpersonal relation-ships, he is unable to establish long lasting friendships or romantic relationships and maintains a superficial and not very affective relationship with his family members. Regardinghistoleranceofanxiety,wecanobservea peren-niallyapprehensivetendencyandatendencytoexaggerate catastrophes, which is expressed through his urinary fre-quencyandineverydaysituations,likesweatypalmswhen interactingwithpeople,andinhissexlife,presenting antic-ipatoryanxietyofnotreachingafullerection.
Despiteobservinginthepatientthecognitiveabilityand desiretodevelop thepersonalandprofessionalaspectsof hislife,hedoesnotperformanytypeofactivitieswherehe experiencespleasureandsatisfaction.
Thepatienthasself-reflexiveabilitytosuggestthat pol-lakiuriaisthesuperficialsymptomcoveringdeeperproblems relatedtoself-esteemandhischaracter.
DSM-V
diagnosis
300.82.SomaticSymptomDisorder. 300.02.GeneralizedAnxietyDisorder. 296.21MajorDepressiveDisorder. 3001.9UnspecifiedPersonalityDisorder.
Diagnostic
analysis
TheDSM-Vmodifies theSomatomorphic Disordersand cre-atesanewdiagnosticentityinitsplace;SomaticSymptoms Disorder(SSD)and relateddisorders.Evidenceofmultiple labandimagingstudieswithoutsignificantpathological find-ings,whichexplaintheseverityofthesymptoms,alongwith the lack of responseto several medicaltreatments given bydifferenturologists,ruledoutthepresenceofaknown medicalcondition thatcouldexplainthe patient’surinary symptom,thusconcluding,accordingtotheDSM-V,the pres-enceofaSDD(Table2).8
The urinary symptom generated discomfort and major anxietywhichimpactedthedifferentareasofthepatient’s lifeinanegativeway,sincetheconstantfeelingofinability hindered hisdevelopmentinhiswork,social andpersonal life (Criterion A).The symptom became the centerof his life, and he devoted excessive time and energy worrying about hishealth andsearchingfor an effectivetreatment forover4years(CriteriaBandC).Thesuddenonset,witha persistentcourseandlongevolutionofasingleverysevere somaticsymptom,producingmarkedanxietyanddisability inhiseverydaylife,specifiesthediagnosisasSevere Persis-tentSomaticSymptomsDisorder.
Thenewcomponentsofsomaticsymptomsdisordersare incorporated in this newedition of the DSM-V: affection, cognitionandbehaviorwithinSSDcriteria,providingamore accurate and more comprehensive vision of the patients’ realsignsandsymptoms,incomparisontotheDSM-IV,which evaluatesonlysomaticsymptoms(1ormore).This diagnos-tic reconceptualization providesa useful tool for primary care doctorsor any other non-psychiatrist specialist. This couldbeverybeneficialinordertoreachaproperdiagnosis andtreatmentinanearliermanner,improvingtheprognosis andavoidingeconomicexpensesinhealthcare.6,7,9,10
Additionally,thecriteriaforamajordepressivedisorder, withamoderatesingleepisode,aremet,clinicallyevident andverballyexpressedbythepatient.
Table2 DiagnosticcriteriaforSomaticSymptomsDisorderDSM-V.
SomaticSymptomsDisorder
A.Oneormoresomaticsymptomsthatcausediscomfortorleadtosignificantproblemsineverydaylife.
B.Excessivethoughts,feelings,orbehaviorsrelatedtothesomaticsymptomsorassociatedwithpreoccupationover healthasismanifestedbyoneormoreofthefollowingcharacteristics:
1.Disproportionateandpersistentthoughtsabouttheseverityofthepatient’sownsymptoms. 2.Persistentlyelevateddegreeofanxietyaboutthepatient’shealthorsymptoms.
3.Excessivetimeandenergydedicatedtothesesymptomsortoworryingabouthealth.
Althoughasomaticsymptommaynotbecontinuallypresent,thesymptomaticdisorderispersistent(generallymorethan sixmonths).
Specifyif:
Predominanceofpain(beforepainfulcondition):thisspecifierappliestoindividualswhosesomaticsymptomsimply painoverall.
Specifyif:
Persistent:Apersistentcourseischaracterizedbythepresenceofintensesymptoms,importantalterationand prolongedduration(morethansixmonths).
Specifytheactualseverity:
Light:OnlymatchesoneofthesymptomsspecifiedincriterionB.
Moderate:Matches2ormoreofthesymptomsspecifiedincriterionB.
Severe:Matches2ormoreofthesymptomsspecifiedncriterionBandadditionallymultiplesomaticcomplaintsexist (oroneveryintensesomaticsymptom).
discomfortinsocial,workandinterpersonalareas.Wecan alsoobservedependentpersonalitytraitswiththepatient’s difficultytomakedecisionsandnotassumingresponsibility accordingtohisageandstageinlife.
Therapeutic
plan
When SSDs coexist with a mood or anxiety disorder, the administrationofpsychiatricmedicationsisindicated,along withapsychotherapeutictreatment.Therefore,wedecided tofollowacombinedtreatment.2,5,12---14
Pharmacological
treatment
ThepharmacologicaltreatmentapproachtoSSDshasbeen complicatedduetothelackofconceptualclarityand exces-sive emphasis on the psychosocial causation and efficacy of psychological treatments.15 Every type of psychiatric medication is usedin clinical practiceto treat SSDs, and therearesystemicstudiesfocusedonfivemainmedication groups:tricyclicantidepressants(TCAs),inhibitorsof sero-toninreuptake(SRI),serotoninandnoradrenalinereuptake inhibitors(SNRIs),atypicalantipsychotics,andherbal-based medications.12,15Evidenceshowsthatthesefivegroupsare effectiveforawidevarietyofdisordersandthatalltypes ofantidepressantsseemtohavecertaindegreeof effective-nessonSDDsandrelateddisorders.12,13,15TCAsandSRIsare themostutilizedpharmacologicalagentsinSSDs. Neverthe-less,therearelittledatasupportingitseffectivenessasa stand-alonetreatment.2,5,12,13
The researchleaves manyunanswered questionsabout dosage,treatmentduration,improvementsustainabilityin thelongrunandvariabilityinresponsestodifferenttypes ofmedications.15AccordingtoCarlat(2012)theevidenceof somatictreatmentofdepressioninadultsreportssertraline
tobeafirst-choiceantidepressantthatishardtotop,given itscombinationofefficacy,tolerabilityandlowcost.16
In the reported case, 50mg of sertraline/day is pre-scribed,alongwithlong-actingbenzodiazepine(clonazepam 0.5mg) at night due to the presence of comorbidity withdepressionandanxiety.Thedepressionsymptomsare resolvedwithin2months;however,doctorsdecidedto dou-blethesertralinedosage(100mg)at 6weeksandtripleit (150mg)at3monthsduetothepersistenceoftheanxiety symptom.The urinarysymptomoccurswithlessfrequency untilitisfullyresolvedafter6monthsofcombined treat-ment.Clonazepamissuspendedafter4monthsduetoagood responsetotheantidepressantandtoavoiddependenceon themedication.Becauseofthesignificantimprovementin theurinarysymptomaswellasthedepressiveandanxiety symptoms,SRI isgraduallyreduced to50mg/day until its fullsuspension2yearslater.Thepatienttoleratesthe med-icationadequatelywithoutanyreportofsignificantadverse sideeffects.
Psychotherapeutic
treatment
Fromthe non-pharmacologic treatment, cognitive behav-ioral therapy (CBT) proved to be the most effective; however,theseinterventionshavenotbeenprovenefficient in the long run.5,12,13 According to Kaplanand Sadock, in boththeindividualandgrouppsychotherapyfields,theidea is to help patients face their somatic symptoms, express subjacent emotions and develop alternative strategies to express their feelings. Additionally, some results indicate thatpsychodynamicpsychotherapyisbeneficialto psycho-somaticpatients,where thetherapeutic alliance playsan importantroleand issolidified throughempathy withthe patient’ssuffering.17
Instead,theymustrecognizetherealityofthephysical ail-ments,eveniftheyunderstandthattheiroriginisbasically intrapsychic.2,4,5Aneasyroute ofentryintotheemotional aspectsofphysicalsufferingistheexaminationofits inter-personalramificationsinthepatient’slife.7,17
Wedecidedtobeginwithindividual,expressive psycho-dynamic psychotherapy,with a focuson object relations, twice a week, in 45---50-min sessions. During the first 6 months they included behavioral techniques focused on the urinary symptom. These techniques consisted of: emptying the bladder every 2h, going to the bathroom only to wash his hands and/or face and performing jaw exercises.
Inparalleltothepharmacologicaltreatment,thepatient commitstopsychotherapeutictreatment,withresultswhich impacted his life in a positive way;he enrolls in univer-sity, takes responsibility for his school expenses and his treatment and gradually becomes involved in social and recreationalactivities.Thepatientcontinueswith psycho-dynamicpsychotherapytokeepworkingonhisevasiveand dependentpersonalitytraits,whichcontributedtotheonset ofthephysical symptomandthesubsequentpersonaland professionaldeterioration.
Therapeutic
plan
analysis
The combination of treatments (pharmacological/ psychotherapeutic) can be necessary in patients with severe SSD of a long evolution as in the case presented, even more when there is a comorbidity with depression and/or anxiety.Consequently, despite thefact that there isnocompellingevidencefor theeffectivenessof antide-pressants in SSDs, the choice was based on tolerability, therapeutic efficiency in depression and anxiety and low cost,giventhepatient’seconomicproblems.
Despite the psychotherapeutic treatment of choice of SSDsbeing CBT, above the pharmacological treatment by itself or any other type of psychotherapy, these types of interventionshave notbeen proventobeeffective inthe longrun,sincemostclinicaltrialsonly evaluateresultsin theshort-term. In this case, the patientattends the psy-chiatricoutpatient clinic withthe ideaand hope that his physicalsymptommayhaveapsychologicalcause;aswell as a great motivation to improve his personality aspects which prevented him from relating toothers. Therefore, it is decided in conjunction with the patient to begin a long-term psychodynamic psychotherapy process comple-mented with behavioral techniques. The success of the treatmentobtainedthusfarseemsfavoredbyagood ther-apeuticalliance,self-reflectiveabilityandcommitmentto thetreatment.
Conclusions
The common characteristic evolution of chronicity, social dysfunction,work difficultiesandfrequent useof medical servicesleadtoalevelofdissatisfactionandfrustrationon thepatientaswellasthedoctor,aswellasahigheconomic costinhealthcareservices.2,4,5,18
One of the most valuable contributions in the re-conceptualization of the DSM-V for somatic disorders is
thatitobligesallnon-psychiatriccolleaguesinthemental health areatoplacestress, not onthedescription of the symptomperse,butinexploringhowthesymptomaffects the patient: (a) emotionally (i.e. makes him depressed, anguished,irritated,etc.); (b)cognitively(i.e.rumination onthesymptom,catastrophicideas,etc.);and(c) behav-iorally (i.e.constantmedical consultations, stop working, etc.).8
Even though the chief complaint was pollakiuria, by understanding howitaffected thepatient,notonly phys-ically, but also in other aspects of his life and his surroundings, it helped us situate the functioning of the symptom in hislife, to have a more realistic idea of the patient’sailment andtohave amoreempathictreatment towardhim. Thismoreintegralapproachallowedthe cre-ation of a treatment plan which included not only the symptom,butotheraspectsofthepatient’slifewhichwere subjacenttothephysicalsymptom.
TheDSM-VmodificationsinSSDdiagnosticcriterialeadall healthcareprofessionalstowardamoreintegralevaluation andapproach,whichmayhelpdoctorstohaveamore realis-ticcomprehensionofthepatient,thusavoidingimproperor incompletediagnosisand/ormanagement,whichonlyfavors chronicityandworsensprognosis.6,7,9---11,18
Conflict
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Funding
Nofinancialsupportwasprovided.
References
1.FinkP,HansenMS,OxhojML.Theprevalenceofsomatoform disordersamonginternalmedicalinpatients.JPsychosomRes. 2004;56:413---8.
2.BurtonC.Beyondsomatisation: a reviewofthe understand-ingandtreatmentofmedicallyunexplainedphysicalsymptoms (MUPS).BrJGenPract.2003;53:231---9.
3.Nimnuan C, Hotopf M, Wessely S. Medically unexplained symptoms:anepidemiologicalstudyinsevenspecialities.J Psy-chosomRes.2001;51:361---7.
4.Stephenson DT, Price JR. Medically unexplained physical symptoms in emergency medicine. Emerg Med J. 2006;23: 595---600.
5.Oyama O,Paltoo C,Greengold J.Somatoformdisorders. Am FamPhysician.2007;76:1333---8.
6.Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disor-ders: time for a new approach in DSM-V. Am J Psychiatry. 2005;162:847---55.
7.GhanizadehA,FiroozabadiA.Areviewofsomatoformdisorders inDSM-IV andsomaticsymptomdisordersinproposedDSM-V. PsychiatrDanub.2012;24:353---8.
8.Diagnosticandstatisticalmanualofmentaldisorders.5thed. DSM-5.Somaticsymptomandrelateddisorders.American Psy-chiatricAssociation;2013.p.309---14.
10.KroenkeK, Sharpe M, SykesR. Revisingthe classification of somatoformdisorders:key questions and preliminary recom-mendations.Psychosomatics.2007;48:277---85.
11.VoigtK, NagelA, MeyerB,etal.Towards positivediagnostic criteria: a systematic review of somatoform disorder diag-nosesandsuggestionsforfutureclassification.JPsychosomRes. 2010;68:403---14.
12.KroenkeK. Efficacy of treatment for somatoform disorders: a review of randomized controlled trials. Psychosom Med. 2007;69:881---8.
13.Sumathipala A. What is the evidence for the efficacy of treatments for somatoform disorders? A critical review of previous intervention studies. Psychosom Med. 2007;69: 889---900.
14.JacksonJL,KroenkeK.Prevalence,impact,and prognosisof multisomatoformdisorderinprimarycare:a5-yearfollow-up study.PsychosomMed.2008;70:430---4.
15.Somashekar B, Jainer A, Wuntakal B. Psychopharmacother-apy of somatic symptoms disorders. Int Rev Psychiatry. 2013;25:107---15.
16.CarlatD.Evidence-basedsomatictreatmentofdepressionin adults.PsychiatrClinNAm.2012;35:131---42.
17.SadockBJ,SadockVA.Kaplan&Sadock.SinopsisdePsiquiatría Clínica.Décima edición.TrastornosSomatomorfos.Lippincott WilliamsandWilkins;2009,634,636,647---649.