. . . .
. . . .
CLINICAL RESEARCH
Prevention and epidemiology
Effect of statin therapy on cardiovascular and
renal outcomes in patients with chronic kidney
disease: a systematic review and meta-analysis
Wanyin Hou
1, Jicheng Lv
1*
, Vlado Perkovic
2, Lihong Yang
3, Na Zhao
1, Meg J. Jardine
2,
Alan Cass
2, Hong Zhang
1, and Haiyan Wang
11
Renal Division, Peking University First Hospital, Institute of Nephrology, Peking University and Key Laboratory of Renal Disease, Ministry of Health of China, No. 8, Xishiku Street,
Xicheng District, Beijing, China;2
The George Institute for Global Health, University of Sydney, New South Wales, Australia; and3
Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, Guangdong, China
Received 27 August 2012; revised 17 December 2012; accepted 5 February 2013; online publish-ahead-of-print 6 March 2013
See page 1772 for the editorial comment on this article (doi:10.1093/eurheartj/eht136)
Aims The effects of statin therapy in patients with chronic kidney disease (CKD) remain uncertain. We undertook a
sys-tematic review and meta-analysis to investigate the effects of statin on major clinical outcomes.
Methods and results
We systematically searched MEDLINE, Embase, and the Cochrane Library for trials published between 1970 and November 2011. We included prospective, randomized, controlled trials assessing the effects of statins on cardio-vascular outcomes in people with kidney disease. Summary estimates of relative risk (RR) reductions were calculated with a random effects model. Thirty-one trials that include at least one event were identified, providing data for 48 429 patients with CKD, including 6690 major cardiovascular events and 6653 deaths. Statin therapy produced
a 23% RR reduction (16 – 30) for major cardiovascular events (P,0.001), an 18% RR reduction (8 – 27) for coronary
events, and 9% (1 – 16) reduction in cardiovascular or all-cause deaths, but had no significantly effect on stroke (21%,
– 12 to 44) or no clear effect on kidney failure events (5%,21 to 10). Adverse events were not significantly increased
by statins, including hepatic (RR 1.13, 95% CI 0.92 – 1.39) or muscular disorders (RR 1.02, 95% CI 0.95 – 1.09). Sub-group analysis demonstrated the relative effects of statin therapy in CKD were significantly reduced in people with
advanced CKD (P,0.001) but that the absolute risk reductions were comparable.
Conclusion Statin therapy reduces the risk of major cardiovascular events in patients with chronic kidney disease including those
receiving dialysis.
-Keywords Cardiovascular events † Statin † Chronic kidney disease † Meta-analysis
Introduction
Chronic kidney disease (CKD) is a major public health problem.1
Cardiovascular disease (CVD) continues to be the leading cause of morbidity and mortality among people with CKD worldwide, with rates of cardiovascular events and mortality consistently
increasing as kidney function declines.2,3 Dialysis patients have
mortality rates up to 40-fold higher than the general population,
with CVD being responsible for up to 50% of these deaths.4
Patients with CKD have higher prevalence of a number of risk factors for CVD, including lipid abnormalities, hypertension, obesity, and diabetes.
Kidney Disease Outcome Quality Initiative (K/DOQI) clinical practice guidelines have recommended statin therapy for the pre-vention of CVD in patients with CKD and high-LDL cholesterol
(LDL-C) levels.5 However, the value of this approach continues
to be debated, particularly in those with the most advanced kidney dysfunction. Levels of cholesterol in patients with kidney disease do not always have the same log-linear relationship with
cardiovascular events observed in the general population.6
Indeed, a ‘U’-shaped or inverse relationship has been described in cohort studies of dialysis patients where people with the lowest levels of LDL-C have the worst outcomes. The burden of CVD may not be predominantly due to atherosclerotic disease
*Corresponding author. Tel:+86 10 83572388, Fax:+86 10 66551055, Email:[email protected]
Published on behalf of the European Society of Cardiology. All rights reserved.&The Author 2013. For permissions please email: [email protected]
European Heart Journal (2013)34, 1807–1817
doi:10.1093/eurheartj/eht065
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
in people with severely decreased GFR when compared with people with normal renal function. Emerging data suggest the pattern of cardiovascular pathology may be different in advanced CKD, with vascular stiffness and calcification, structural heart disease, and sympathetic overactivity contributing to an increasing
risk of cardiac arrhythmia and heart failure.7 Thus, the effect of
statin therapy may be less compared with the general population. In the past few years, several large-scale trials of statin therapy in people with CKD have been completed, including the recent
large SHARP (Study of Heart and Renal Protection) trial.8
Although some of these trials have shown benefit,8 others
have shown no effect,9,10 leading to uncertainty about the
pres-ence and magnitude of cardiovascular protective effects and there-fore difficulties for clinicians in the interpretation of the results.
Two recent overviews have investigated the effect of statin in patients with CKD. However, both have not evaluated the effect
of kidney function on the statin therapy.11,12 In this systematic
review, we sought to synthesize all the available clinical trial data and define better the balance of risks and benefits of statin in patients with CKD and also the effect of kidney function on statin use.
Methods
Data sources, search strategy, and selection
criteria
We performed a systematic review of the published literature according to the approach recommended by the statement for the conduct of meta-analyses of intervention studies. We included data from randomized, controlled trials in which statin was given for at least 6 months to patients with CKD. These data were extracted either from studies conducted solely in people with kidney disease, or from subsets of other trials where data on the CKD population could be obtained.
Relevant studies were identified by searching the following data sources: MEDLINE via Ovid (from 1950 to November 2011), Embase (from 1966 to November 2011), and the Cochrane Library database (Cochrane Central Register of Controlled Trials; no date re-striction), with relevant text words and medical subject headings that included all spellings of ‘kidney disease’, ‘dyslipidemia’, ‘hypercholester-olemia’, ‘cardiovascular disease’, ‘myocardial infarction’, ‘revascularisa-tion’, ‘stroke’, ‘simvastatin’, ‘atorvastatin’, ‘rosuvastatin’, ‘pravasatin’ (see Supplementary material online). Trials were considered without language restriction. Reference lists from identified trials and review articles were manually scanned to identify any other relevant studies. The ClinicalTrials.gov website was also searched for randomized trials that were registered as completed but not yet published.
The literature search, data extraction, and quality assessment were undertaken independently by two authors (W.H. and L.Y.) using a stan-dardized approach. All completed randomized, controlled trials asses-sing the effects of statin compared with placebo and/or compared with conventional therapy in CKD, and that reported one or more of the primary or secondary outcomes, were eligible for inclusion. Trials that recruited patients with kidney transplants were not included in this study.
Data extraction, quality assessment,
and outcome estimation
Published reports were obtained for each eligible trial, and relevant in-formation was extracted into a spreadsheet. The data sought included
baseline patient characteristics (age, sex, history of diabetes, history of CVD, mean systolic and diastolic blood pressure values, lipid concen-trations), statin used, dose of drug, follow-up duration, change in LDL-C concentrations, outcome events, and adverse events. Study quality was judged by the proper conduct of randomization, conceal-ment of treatconceal-ment allocation, similarity of treatconceal-ment groups at baseline, the provision of a description of the eligibility criteria, completeness of follow-up, and the use of an intention-to-treat analysis, and was
quan-tified with the Jadad scale.13Any disagreement in the abstracted data
was adjudicated by a third reviewer (J.L.).
We collected data for major cardiovascular events (defined as a composite including fatal or non-fatal myocardial infarction, fatal or non-fatal stroke, revascularization procedures, cardiovascular death, and heart failure, or comparable definitions used by individual authors), cardiovascular mortality, all-cause death, new onset cancer, and other drug-related adverse events. We listed all cardiovascular events for each included studies in Supplementary material online,
Table S2. Trials that compare high- vs. low-dose statin therapy met the inclusion criteria but in a separate analysis. Kidney failure events were defined as a 25% decrease in the estimated GFR, doubling of serum creatinine, or end stage renal disease (ESRD) as defined by the authors of each study.
When required quantitative data were not provided in the relevant
article from the text, we use the g3 data software (http://www.frantz.fi/
software/g3data.php) to extract exact numbers from published figures.
Statistical analysis
Individual patient data were not available from the studies in this ana-lysis, so tabular data were used. Individual study relative risks (RRs) and 95% CIs were calculated from event numbers and total population at
risk extracted from each trial, using a standard method14before data
pooling. In the calculation of risk ratios, the total number of patients randomly assigned in each group was used as the denominator. Summary estimates of risk ratios were obtained with a random
Figure 1 Identification process for eligible studies.
W. Houet al.
1808
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
. . . .
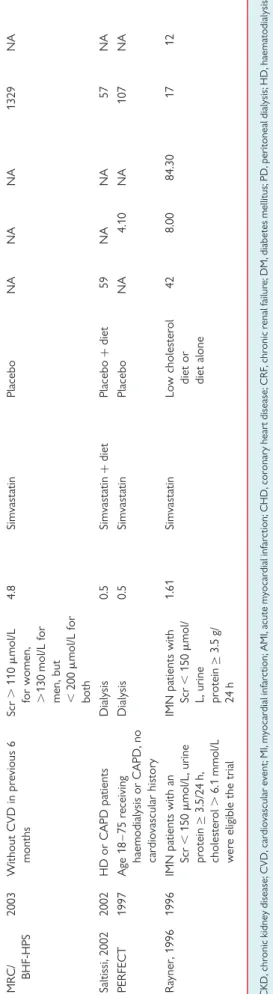
. . . . Table 1 Characteristics of studies reporting the effects of statin in patients with chronic kidney disease
Study Year Inclusion criteria Definition of CKD Duration of time, year
Treatment group Control group Mean age, years
Baseline Number of patients
History of CVD (%) LDL- C,
mmol/L eGFR, mL/min/ 1.73 m2
Han, 2011 2011 PD.3 months Dialysis 0.5 Rosuvastatin 10 mg/ day+ARB 80 mg/day
Placebo+ARB 80 mg/day
49 4.83 NA 124 0
ATTEMP 2011 CKD stage 3 patients with metabolic syndrome, no CVD or DM
CKD stage 3, eGFR¼30 – 59 mL/min/ 1.73 m2
3.5 Atorvastatin LDL-C target on 100 mg/L
Atorvastatin LDL-C target on 130 mg/dL
57 4.37 47.60 349 2
SHARP 2011 History of CKD, age.40, Scr: men.150mmol/L, women .130mmol/L
Increased Scr: men .150mmol/L, women .130mmol/L
4 Simvastatin+ezetimibe Placebo 62 2.70 26.60 9438 15
Air Force/ Texas
2009 Hyperlipidaemia, no CVD or DM
eGFR,60 mL/min/ 1.73 m2
5.2 Lovastatin Placebo 62 3.90 53.00 304 0
JUPITER 2010 No history of CVD, LDL-C,130 mg/dL
eGFR,60 mL/min/ 1.73 m2
1.9 Rosuvastatin Placebo 70 2.82 56.00 3267 0
LORD 2008 History of CKD, Scr.120mmol/L
Increased Scr 120mmol/L
2.5 Atorvastatin Placebo 60 3.22 31.90 123 17
PANDA 2010 Type 2 DM Urinary albumin creatinine.5 mg /mmol
2.1 Atorvastatin Atorvastatin 64 3.06 71.70 119 28
MEGA 2009 No history of CHD and/or stroke
eGFR,60 mL/ min/1.73 m2
5.3 Pravastatin Diet therapy NA 4.00 52.60 2978 0
AURORA 2009 ESRD patients, regular haemodialysis for at least 3 months
Dialysis 3.2 Rosuvastatin Placebo 64 2.59 NA 2776 40
CARDS 2009 Type 2 DM or with risk factors such as hypertension, proteinuria, no CVD history
eGFR,60 mL/min/ 1.73 m2
3.9 Atorvastatin Placebo 65 3.10 53.30 970 0
ALLIANCE 2009 With known CHD patients eGFR,60 mL/min/ 1.73 m2
4.53 Atordvastatin Usual care (atorvastatin will not be excluded from the usual-care group)
66 3.83 51.30 579 100
4S 2008 With a history of MI and/or stable angina
eGFR,60 mL/min/ 1.73 m2
5.5 Simvastatin Placebo 63 4.97 54.80 409 100
ALLHAT 2008 Stage 1 or 2 hypertension with at least one additional CHD risk factor
eGFR,60 mL/min/ 1.73 m2
4.8 Pravastatin Usual care 71 3.79 50.80 1557 18
Continued
Effects
of
statin
therap
y
in
pati
ents
with
CKD
1809
. . . .
. . . . Table 1 Continued
Study Year Inclusion criteria Definition of CKD Duration of time, year
Treatment group Control group Mean age, years
Baseline Number of patients
History of CVD (%) LDL- C,
mmol/L eGFR, mL/min/ 1.73 m2
TNT 2008 With clinically evident CHD eGFR,60 mL/min/ 1.73 m2
5 Atorvastatin 80 mg/day Atodvastatin 10 mg/day
66 2.49 53.00 3107 100
Melanie S. Joy, 2008
2008 Hyperlipidaemia and CKD patients
Dialysis 0.69 Atorvastatin No treatment 65 2.92 NA 45 51
4D 2005 Type 2 DM receiving maintenance haemodialysis for,2 years
Dialysis 4 Atorvastatin Matching placebo 66 3.23 NA 1255 29
Stegmayr, 2005
2005 GFR,30 measured by clearance of either creatinine, Cr51-EDTA, or iohexol.
eGFR,30 mL/min/ 1.73 m2
2.58 Atorvastatin Placebo 68 3.56 NA 143 37
LIPS 2004 Successfully undergone their first PCI, mild renal impairment
Renal impairment, creatinine clearance ,55.9 mL/min
3.8 Fluvastatin Placebo 69 3.39 NA 310 100
Vincenzo Panichi, 2005
2005 CRF with
hypercholesterolaemia (LDL-C.100 mg/dL)
Mean creatinine clearance 45 mL/ min
0.5 Simvastatin Placebo 58 3.59 45.00 55 NA
Dornbrook, 2005
2005 Hyperlipidaemia and undergoing long-term dialysis
Dialysis 1.67 Atorvastatin No treatment 66 3.05 NA 19 NA
Verma, 2005 2005 GFR,60; no clinical evidence of acute renal failure
eGFR,60 mL/min/ 1.73 m2
0.38 Rosuvastatin No treatment 73 3.62 42.30 91 0
UK-HARP-I 2005 Scr≥150mmol/L Scr≥150mmol/L 1 Simvastatin Placebo 54 3.21 NA 448 9 PREVEND IT 2004 No antihypertension therapy
and Tchol,8 mmol/L or Tchol,5 previous MI
Microalbuminuria with 15 – 300 mg/ 24 h
3.83 Pravastatin Placebo 52 4.10 NA 864 3
Verglione, 2004
2004 C-reactive protein≥3 mg/L; undergo HD treatment for at least 6 months
Dialysis 0.5 Atorvastatin Placebo 65 NA NA 33 NA
Tonelli, 2004 (PPP)
2004 CKD subgroup of trials in WOSCOPS, LIPID, CARE
eGFR,60 mL/min/ 1.73 m2
5 Pravastatin Placebo NA NA NA 16 824 NA
Lins, 2004 2004 CRF treated with
haemodialysis.3months and hyperlipidaemia
Dialysis 0.23 Atordvastatin Placebo 64 3.39 NA 42 NA
CARE 2003 GFR,60, with AMI and hyperlipidaemia
eGFR,60 mL/min/ 1.73 m2
5 Pravastatin Placebo 63 3.61 53.20 690 11
W
.
Hou
et
al
.
1810
effects model. The percentage of variability across studies attributable
to heterogeneity beyond chance was estimated with theI2statistic. For
each trial, we calculated not only the average risk reduction, but also the average risk reduction per 1.0 mmol/L LDL-C reduction at the end of each trial where data were available (1 divided by the observed LDL reduction, for example, if the RR was 0.7 and the reduction in systolic blood pressure was 0.8 mmol/L, the standardized RR estimate was 0.71/0.8.15
Potential publication bias was assessed with the Egger test and represented graphically with Begg funnel plots of the natural log of the RR vs. its standard error.
We explored potential heterogeneity in the estimates of treatment effect with univariate meta-regression (for end-of-trial parameters such as achieved LDL-C concentrations) and by comparing summary results obtained from the subsets of studies grouped by number of patients, number of mortality events, publication year, statin used, diabetic status, stage of CKD, baseline morbidity, and study quality.
A two-sidedP-value,0.05 was regarded as significant for all analyses.
All statistical analyses were done with STATA (version 12.0).
Results
The literature search yielded 2310 articles, of which 134 were
reviewed in full text (Figure1). Of these, 31 randomized, controlled
trials met the inclusion criteria. These trials included a total of 48 429 patients with CKD, in whom 6690 major cardiovascular events were reported from 22 studies, and 6653 deaths from 23 studies. Study follow-up duration ranged from 6 months to 4.9 years. Thirteen trials were placebo-controlled and 18 trials used
open-label designs. Ten trials reportedpost hocanalyses of the
sub-group with CKD, four compared intensive lipid-lowering therapy to conventional or low-dose therapy. Formal statistical testing suggested the possibility of publication bias for the outcome of major cardiovascular outcomes with a borderline Egger test result
(P¼0.062, see Supplementary material online,Figure S1).
Table1summarizes the characteristics of the included studies.
Ten trials with 4503 participants were exclusively undertaken in
dialysis patients,9,10,16–1818 trials (n¼33 252) were in non-dialysis
patients, and another 3 trials (n¼10 029) had a mixed population
that included both dialysis and non-dialysis patients. Baseline esti-mated GFR levels for the participants in the trials were reported in the published paper or could be calculated or estimated from
the inclusion criteria (Figure 2). Two trials were undertaken in
people with diabetes and CKD.
The mean age of the study participants ranged between 42 and 73 years. Included studies were undertaken in Europe, North America, and in some part of Asia and Africa. The agents used in the studies varied: 12 studies assessed the effects of ator-vastatin, 8 assessed simator-vastatin, 5 assessed praator-vastatin, 4 assessed rosuvastatin, where 1 assessed fluvastatin and 1 lovastatin.
We also recorded key indicators of trial quality, in particular the process of randomization, concealment of allocation, and the use of intention-to-treat analysis techniques, blinding, withdraws and
dropouts (see Supplementary material online,Table S1). Overall,
13 trials had a Jadad scale of 4, others scored≤3.
Data regarding the effects of statin on major cardiovascular events were available from 22 trials, including 44 096 participants and 6695 events. Overall, statin therapy produced a 23% reduction
MR C/ BHF-HPS 20 03 W itho ut CVD in pre vio us 6 mon ths Scr . 110 m mol /L fo r wo men, . 130 mol/L for me n, but , 200 m mol/L for b oth 4.8 Simvas ta tin Pla cebo NA NA NA 1329 NA Salti ssi, 2002 20 02 HD or C A PD pa tients Dialy sis 0.5 Simvas ta tin + diet Pla cebo + diet 59 NA NA 57 NA PER FECT 19 97 A ge 18 – 75 re ceiving haem odialy sis or C APD, no ca rdio vascular his tor y Dialy sis 0.5 Simvas ta tin Pla cebo NA 4.10 NA 107 NA Ra yner, 1996 19 96 IMN pa tients with an Scr , 15 0 m mol/ L, urine pr ote in ≥ 3.5/2 4 h, cho les ter ol . 6.1 mmo l/L w er e elig ible the tria l IMN pa tients with Scr , 15 0 m mol/ L , urin e p ro tein ≥ 3.5 g/ 24 h 1.6 1 Simvas ta tin Lo w cho les te ro l diet or diet al one 42 8.00 84 .30 17 12 CKD, chr onic kidney disease; CVD, cardiovascular ev ent; MI, my ocardial infar ction; AMI, acute my ocardial infarction; CHD, coronary heart disease ;CRF ,chr onic renal failur e; DM, diabetes mellitus; PD, peritoneal dialysis; HD, haemat odialysis dialysis; C APD, continuous ambula tory peritoneal dialysis; IMN, idiopa thic membranous nephropat hy; Scr, serum cr eatinine; ESRD, end stage renal disease.
Effects of statin therapy in patients with CKD
1811
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
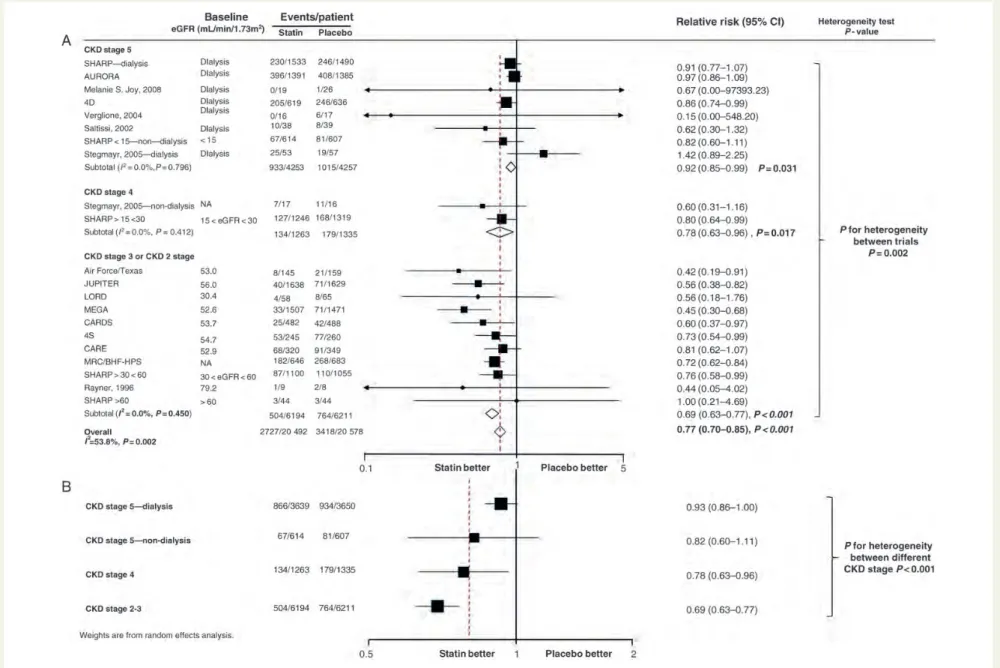
Figure 2 Summary of the effects of statin therapy on major cardiovascular events stratified by kidney function. Only one trial and one subgroup (SHARP.60 and Rayner, 1996) were in chronic kidney disease (CKD) 2 stage with few endpoints (4 cardiovascular events and 105 patients), and we combined chronic kidney disease stage 3 and chronic kidney disease stage 2 into one subgroup.
W
.
Hou
et
al
.
1812
in the risk of cardiovascular events (RR 0.77, 95% CI 0.70 – 0.85,
P,0.001) (Figure 2A) or an 18% per 1 mmol/L LDL (RR 0.82,
95% CI 0.74 – 0.91, P,0.001, see Supplementary material online,
Figure S2) with evidence of heterogeneity in the results of individual
trials. Subgroup analysis showed that statin effect was significantly
modified by kidney function (Figure2B). Four trials with 4154
par-ticipants that compared more vs. less intensive statin regimens showed that intensive statin therapy reduced cardiovascular events by 28% in people with CKD (see Supplementary material
online,Figure S3).
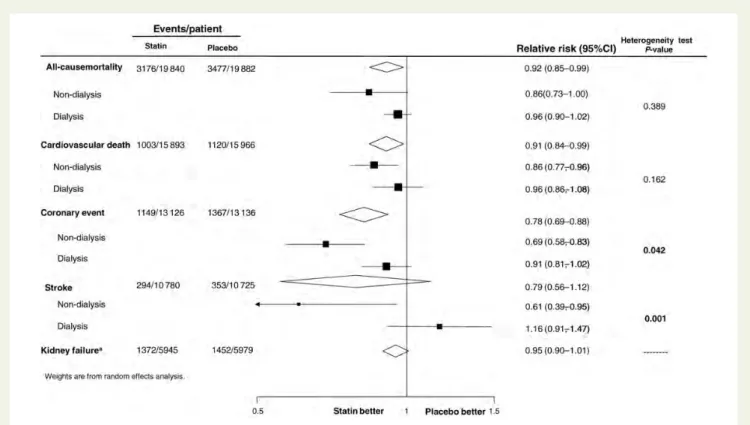
Data for coronary events were available from 15 trials8–10,19–29
including 26 262 patients in whom 2516 events were recorded. Statin therapy reduced the risk of coronary events by 22% (RR 0.78, 95% CI 0.69 – 0.88) without evidence of heterogeneity
(I2¼29.6%, P¼0.134) (Figure 3). Eight trials reported stroke,
including 21 505 and 647 events. Overall, there was no effect of statin therapy on the risk of stroke (RR 0.79, 95% CI 0.56 – 1.12)
with evidence of heterogeneity between trials (P-value for
hetero-geneity¼0.001).
Cardiovascular death was reported in 11 trials including 31 859 patients among whom 2123 events were observed. Nineteen trials reported all-cause death, including 39 722 patients and 6653 events. Statin therapy reduced all-cause death (RR 0.92, 95% CI 0.85 – 0.99) and also cardiovascular death (RR 0.91, 95% CI
0.84 – 0.99) without clear evidence of heterogeneity (Figure3).
Kidney failure events defined as a 25% decrease in the estimated GFR, doubling of serum creatinine, or ESRD were reported in six
trials8,20,23,26,30,31 including 11 924 participants and 2824 events.
There was no clear evidence that statins reduced the risk of
kidney failure (RR 0.95, 95% CI 0.90 – 1.01) (Figure3).
Figure 3 Summary of the relative risks of all outcomes.aKidney failure events defined as a 25% decrease in the estimated GFR, doubling of
serum creatinine, or ESRD.
. . . . Table 2 Absolute risk reduction and number needed to treat of statin in patients with chronic kidney disease
CKD stagea Statin, number of patients
Placebo, number of patients
Experiment CVE
Control CVE
ARR (95% CI) (per study duration on average)
NNT (95% CI) (per study duration on average)
CKD stage 5 4283 4237 933 1015 0.022 (0.004 – 0.040) 46 (25 – 257) CKD stage 4 1263 1335 134 179 0.028 (0.003 – 0.053) 36 (19 – 330) CKD stages 3, 2 6194 6211 504 764 0.042 (0.031 – 0.052) 24 (19 – 32)
CVE, cardiovascular event. a
CKD stage 5: estimated GFR (eGFR),15 mL/min/1.73 m2
; CKD stage 4: eGFR 15 – 30 mL/min/1.73 m2
; CKD stage 3: eGFR 30 – 60 mL/min/1.73 m2
; CKD stage 2: eGFR
60 – 90 mL/min/1.73 m2.
Effects of statin therapy in patients with CKD
1813
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
The heterogeneity in the effect across the included studies was assessed by subgroup analysis and meta-regression. This revealed that the effect of statin therapy on major cardiovascular events was modified by the average baseline kidney function of the
parti-cipants in the included trials (P-value for heterogeneity,0.001),
with a progressively smaller relative risk reduction (RRR) with a lower estimated GFR. The RRR for cardiovascular event in trials with CKD stage 5 including patients with dialysis (8
trials8–10,27,29,32 with 7987 participants) was 8% (95% CI 1 – 14,
I2¼0%) and 22% (95% CI 4 – 37,I2¼0%) in stage 4 (2 trials or
subgroups,8,27 2598 patients) and 31% (95% CI 4 – 37,I2¼0%)
in stage 3 or 2 (11 trials or subgroups with 12 330 participants). Only two small trials or subgroups included 107 participants with CKD stage 2, so meta-analysis was not separately done in this group. The benefits of statin in patients not on dialysis (RR
0.70, 95% CI 0.63 – 0.88) was larger (P-value for heterogeneity,
0.001) than those in patients on dialysis (RR 0.92, 95% CI 0.85 – 0.99). Adjusting the risk ratio for cardiovascular events by weighted average LDL-C reduction did not substantially modify these findings. Reductions in the risk of cardiovascular events per 1 mmol/L LDL-C reduction at the end of each trial were 27%
(RR 0.73, 95% CI 0.65 – 0.83, P,0.001) in patients with CKD
not requiring dialysis compared with 10% (RR 0.90, 95% CI
0.83 – 0.97,P¼0.01) in patients requiring dialysis (P-value for
het-erogeneity¼0.007) (see Supplementary material online, Figure
S2). Similar findings were observed for coronary events (RR
0.69, 95% CI 0.58 – 0.83 in the non-dialysis population and RR
0.91, 95% CI 0.81 – 1.02 in the dialysis population, P-value for
heterogeneity¼0.042) and stroke (RR 0.61, 95% CI 0.39 – 0.95
in non-dialysis patients and RR 1.16, 95% CI 0.91 – 1.47 in dialysis
patients,P-value for heterogeneity¼0.001) (Figure3).
As the risk of CVD increased as the kidney function deterio-rated, but with the risk ratio lower, we calculated the absolute risk reduction among patients with different CKD stages
[Table 2; we also provide three models for the number needed
to treat (NNT), see Supplementary material online,Tables S3.1 –
3.3]. The NNT to reduce one major cardiovascular event was
46 in CKD stage 5 (25 – 257), 36 in CKD stage 4 (19 – 330), and 24 in CKD stages 2 – 3 (19 – 32).
Subgroup analysis was done for major cardiovascular events
according to other baseline characteristics (Figure 4). The effect
sizes were greater in trials that recorded a higher mean baseline
LDL-C concentration (P-value for heterogeneity¼0.012). On
univariate meta-regression, there was a trend for statin therapy Figure 4 Subgroup analyses for the effects of statin on major cardiovascular events.aTrials that recruited only patients with chronic kidney
disease.bTrials that were conducted in the general population where subgroups of patients with kidney disease were available.
W. Houet al.
1814
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
to produce the greatest benefit when LDL-C concentrations were
improved most (Figure 5, P¼0.062) in non-dialysis patients. In
contrast, no clear relationship between LDL-C reduction and cardiovascular benefit was observed in patients receiving dialysis.
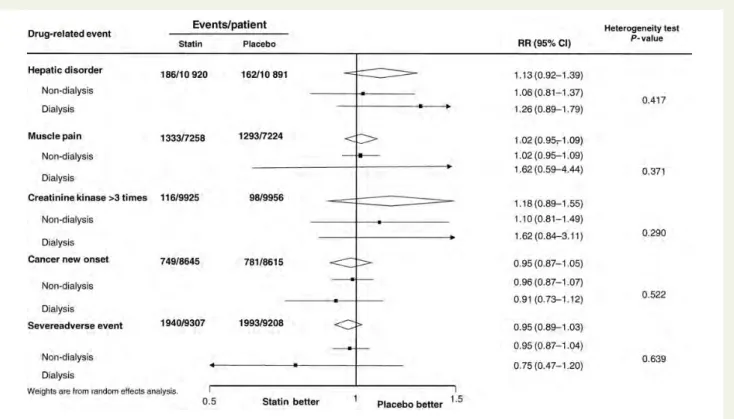
Key adverse outcomes were reported by few trials. For hepatic
impairment6,8,9,25,26,32,33 (RR 1.13, 95% CI 0.92 – 1.39), muscle
pain6,26–28,34–36(RR 1.02, 95% CI 0.95 – 1.09), increased creatinine
kinase level6,8,16,22,24,26,28,30,31,37,38 (RR 1.18, 95% CI 0.89 – 1.55),
cancer morbidity6,8,24,39(RR 0.95, 95% CI 0.87 – 1.05), and severe
adverse event8,9,25,26,30,32,36 (RR 0.95, 95% CI 0.89 – 1.03) in the
analysis (Figure 6), no significant difference in risk was observed
in the statin-treated participants.
The conclusions were not changed after adjustment for publica-tion bias with the trim-and-fill method (data not shown).
Discussion
The management of lipids in people with CKD has been an area of intense debate over recent years, particularly in those with more advanced kidney dysfunction. This large quantitative review, includ-ing 31 trials with more than 48 000 individuals, suggests that therapy with statin reduces the risk of cardiovascular events
across different levels of kidney function. Major cardiovascular events are reduced by 23%, including a 22% reduction in coronary events, and 9% reduction in cardiovascular or all-cause death. No significant effect was observed on the risk of kidney failure, or on the risk of adverse events including cancer mortality.
The most important new finding of this study is the clear result that the effect of statin therapy is significantly modified by kidney function. The observed beneficial effects appear to be smaller in people with stage 5 kidney disease and those requiring dialysis. Similar findings were observed for coronary heart disease and stroke. Importantly, the absolute risk reductions and NNT were only slightly less in people with advanced kidney disease, suggesting that statin therapy still confers important benefits in these indivi-duals. In this analysis, we did not find that the adverse events of statin were increased in the patients with CKD, which suggested the safety of using statin in this population. However, this is still needed to be cautious given many trials included in this
meta-analysis arepost hocanalysis, and adverse events are reported
by only a few trials. For the effect on stroke risk in patients with dialysis, the risk ratio even goes in the opposite direction (RR 1.16, 95% CI 0.90 – 1.47), and more data are still needed to evaluate the safety of statin in dialysis patients.
The effects of LDL-lowering with statin therapy in patients without CKD have been described by the Cholesterol Treatment Trialists’ (CTT) Collaboration, and shown that statin therapy can safely reduce the 5-year incidence of major coronary events, cor-onary revascularization, and stroke by about one-fifth per mmol/L
reduction in LDL-C.40In this study, LDL-C-lowering with statin in
CKD could yield 18% reduction per 1.0 mmol/L reduction in major cardiovascular events, which is close consistent with the effects seen in the CTT study. Our study is also consistent with the results from the SHARP study and supports statin use in patients with CKD, including dialysis patients. However, SHARP did not have sufficient power to assess the effects separately in dialysis and non-dialysis patients. This large meta-analysis with more than four times of participants strongly supports larger benefits in patients with less severe renal impairment. Further support comes from the meta-regression analysis that a linear association trend exists in patients with non-dialysis although not obvious in patients with dialysis.
The reason for the lesser RRR in patients with ESRD than those achieved in patients with less severe kidney disease may reflect differences in the distribution of CVD among these groups of patients. Cardiovascular disease may have different aetiological pathways in people with ESRD compared with those with better renal function, and indeed may have a different
pathophysi-ology.39,41,42 Cardiovascular risk factors specific to ESRD include
calcium and phosphorus dysregulation, anaemia, hyperhomocystei-naemia, increased levels of oxidant stress, and chronic
inflamma-tion.33,37–39,43–45 In addition, the burden of cardiovascular
dysfunction may be further accelerated by haemodynamic instabil-ity in dialysis patients. It is postulated that statins may not impact the substantial proportion of cardiovascular events in ESRD popu-lations resulting from non-ischaemic myocardial abnormalities, left ventricular hypertrophy, and fluctuations in electrolytes and fluid
volumes.43These may explain the more modest relative effect of
statins than that seen in an earlier stage of kidney disease. Figure 5 Univariate meta-regression exploring the role of
achieved lipid concentrations on the effectiveness of statin therapy on cardiovascular events. Meta-regression of cardiovas-cular events and LDL cholesterol reduction difference between statin and placebo or conventional therapy groups. Black circle were trials exclusively in dialysis patients (PREVEND IT, ATTEMP, Air Force, JUPITER, PANDER, ALLIANCE, LIPS, Rayner 1996). White circle were trials exclusively in non-dialysis patients(AURORA; 4D; Melanie S. Joy, 2008; Saltissi, 2002). Grey Circles were trials of mixed population, respectively indicated Stegmayr 2005 and SHARP. They were included in both
non-dia-lysis and dianon-dia-lysis trials in the regression ananon-dia-lysis.P-value for
non-dialysis patients¼0.062, coefficient¼20.503;P-value for
dialy-sis patients¼0.625, coefficient¼20.234.
Effects of statin therapy in patients with CKD
1815
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
Trials including individuals with high average baseline LDL-C concentrations reported significantly greater proportional risk reductions, a finding that accords with the results in the general population. Importantly, we noted a significant relationship between the magnitude of LDL-C-lowering achieved with therapy and the reported risk reductions in patients with non-dialysis patients, although this phenomenon was not observed in patients with ESRD. This further supports the hypothesis that the excess of cardiovascular events observed in people with advanced kidney disease may not be atherosclerotic in nature,
and therefore not able to be reduced with statins.7However, in
this analysis, given that the rates of cardiovascular events and mor-tality consistently increase as kidney function deteriorates, clinically meaningful absolute risk reductions can still be achieved in patients with severe kidney dysfunction. In the subgroup analysis, we also noted significant heterogeneity between trials only involving patients with kidney disease and trials in the general population where the subgroup with CKD was available. This difference may be due to different kidney functions among these trials. The trials with CKD are mostly studies involving patients with dialysis,
whereas in the post hoc analysis, participants were mainly
non-dialysis patients.
This meta-analysis benefits from a large volume of data available, and the resultant precision in the observed benefits across a broad range of kidney function. Our study does, however, have limitations mainly as a result of it being based on published data, which limits the capacity to fully explore effects in subgroups. The different defi-nitions used by the contributing trials cannot be fully integrated, and
the outcome definitions, in particular, required some grouping of event types. Also in the meta-regression assessing kidney function and the effect of statins, we were only able to use the mean baseline GFR of the included trials rather than individual patient kidney function.
In conclusion, this study has provided strong evidence that statin therapy reduces the risk of major vascular events, as well as cardio-vascular and all-cause death in patients with CKD, across a broad range of kidney functions including patients with dialysis. Although the relative vascular protection of statins is significantly modified by kidney function, meaningful reductions in absolute risk would be expected to be achieved in every stage of CKD. Additional protective strategies are required to address the large excess of cardiovascular events in the population with ESRD.
Supplementary material
Supplementary material is available at European Heart Journal
online.
Funding
This study was supported by grants from the Major State Basic
Research Development Program of China (973 program,
No. 2012CB517700), National Natural Science Foundation of China (No. 81270795, 30825021), Natural Science Fund of China to the In-novation Research Group (81021004) and Program for New Century Excellent Talents in University from the Ministry of Education of China (NCET-12-0011).
Figure 6 Adverse events of statin reported in the trials with chronic kidney disease. Drug-related adverse events (hepatic disorder defined as
ALT or AST.normal×3 times; muscle pain; creatinine kinase.normal×3 times; cancer new onset; severe adverse event) were involved in
the meta-analysis.
W. Houet al.
1816
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
Conflict of interest: none declared.
References
1. James MT, Hemmelgarn BR, Tonelli M. Early recognition and prevention of
chronic kidney disease.Lancet2010;375:1296 – 1309.
2. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and
the risks of death, cardiovascular events, and hospitalization.N Engl J Med2004;
351:1296 – 1305.
3. Yach D, Leeder SR, Bell J, Kistnasamy B. Global chronic diseases.Science2005;
307:317.
4. Sarnak MJ, Levey AS. Cardiovascular disease and chronic renal disease: a new
paradigm.Am J Kidney Dis2000;35(4 Suppl. 1):S117 – S131.
5. Snyder JJ, Collins AJ. KDOQI hypertension, dyslipidemia, and diabetes care guide-lines and current care patterns in the United States CKD population: National
Health and Nutrition Examination Survey 1999 – 2004.Am J Nephrol2009;30:
44 – 54.
6. Liu Y, Coresh J, Eustace JA, Longenecker JC, Jaar B, Fink NE, Tracy RP, Powe NR, Klag MJ. Association between cholesterol level and mortality in dialysis patients:
role of inflammation and malnutrition.JAMA2004;291:451 – 459.
7. Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in
chronic renal disease.Am J Kidney Dis1998;32(5 Suppl. 3):S112 – S119.
8. Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano M,
Kasiske B, Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U,
Ophascharoensuk V, Fellstrom B, Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Gronhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham M, Majoni W, Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, Simpson D, Sleight P, Young A, Collins R. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of
Heart and Renal Protection): a randomised placebo-controlled trial.Lancet2011;
377:2181 – 2192.
9. Fellstrom BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, Chae DW, Chevaile A, Cobbe SM, Gronhagen-Riska C, De Lima JJ, Lins R, Mayer G, McMahon AW, Parving HH, Remuzzi G, Samuelsson O, Sonkodi S, Sci D, Suleymanlar G, Tsakiris D, Tesar V, Todorov V, Wiecek A, Wuthrich RP, Gottlow M, Johnsson E, Zannad F. Rosuvastatin and cardiovascular events in
patients undergoing hemodialysis.N Engl J Med2009;360:1395 – 1407.
10. Wanner C, Krane V, Marz W, Olschewski M, Mann JF, Ruf G, Ritz E. Atorvastatin
in patients with type 2 diabetes mellitus undergoing hemodialysis.N Engl J Med
2005;353:238 – 248.
11. Palmer SC, Craig JC, Navaneethan SD, Tonelli M, Pellegrini F, Strippoli GF. Ben-efits and harms of statin therapy for persons with chronic kidney disease: a
sys-tematic review and meta-analysis.Ann Intern Med2012;157:263 – 275.
12. Upadhyay A, Earley A, Lamont JL, Haynes S, Wanner C, Balk EM. Lipid-lowering therapy in persons with chronic kidney disease: a systematic review and
meta-analysis.Ann Intern Med2012;157:251 – 262.
13. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is
blind-ing necessary?Control Clin Trials1996;17:1 – 12.
14. Woodward M.Epidemiology: Study design and data analysis. 2nd edition. Boca
Raton, FL, USA: Chapman and Hall/CRC; 2005.
15. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the pre-vention of cardiovascular disease: meta-analysis of 147 randomised trials in the
context of expectations from prospective epidemiological studies.BMJ 2009;
338:b1665.
16. Han SH, Kang EW, Yoon SJ, Yoon HS, Lee HC, Yoo TH, Choi KH, Han DS, Kang SW. Combined vascular effects of HMG-CoA reductase inhibitor and angio-tensin receptor blocker in non-diabetic patients undergoing peritoneal dialysis. Nephrol Dial Transplant2011;26:3722 – 3728.
17. Joy MS, Dornbrook-Lavender KA, Chin H, Hogan SL, Denu-Ciocca C. Effects of
atorvastatin on Lp(a) and lipoprotein profiles in hemodialysis patients.Ann
Phar-macother2008;42:9 – 15.
18. Dornbrook-Lavender KA, Joy MS, Denu-Ciocca CJ, Chin H, Hogan SL, Pieper JA. Effects of atorvastatin on low-density lipoprotein cholesterol phenotype and
C-reactive protein levels in patients undergoing long-term dialysis.
Pharmacother-apy2005;25:335 – 344.
19. Asselbergs FW, Diercks GF, Hillege HL, van Boven AJ, Janssen WM, Voors AA, de Zeeuw D, de Jong PE, van Veldhuisen DJ, van Gilst WH. Effects of fosinopril and
pravastatin on cardiovascular events in subjects with microalbuminuria.Circulation
2004;110:2809 – 2816.
20. Chonchol M, Cook T, Kjekshus J, Pedersen TR, Lindenfeld J. Simvastatin for sec-ondary prevention of all-cause mortality and major coronary events in patients
with mild chronic renal insufficiency.Am J Kidney Dis2007;49:373 – 382.
21. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, Charlton-Menys V, DeMicco DA, Fuller JH. Effects of atorvastatin on kidney out-comes and cardiovascular disease in patients with diabetes: an analysis from the
Collaborative Atorvastatin Diabetes Study (CARDS).Am J Kidney Dis2009;54:
810 – 819.
22. Collins R, Armitage J, Parish S, Sleigh P, Peto R. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a
rando-mised placebo-controlled trial.Lancet2003;361:2005 – 2016.
23. Kendrick J, Shlipak MG, Targher G, Cook T, Lindenfeld J, Chonchol M. Effect of lovastatin on primary prevention of cardiovascular events in mild CKD and kidney function loss: a post hoc analysis of the Air Force/Texas Coronary
Athero-sclerosis Prevention Study.Am J Kidney Dis2010;55:42 – 49.
24. Lemos PA, Serruys PW, de Feyter P, Mercado NF, Goedhart D, Saia F, Arampatzis CA, Soares PR, Ciccone M, Arquati M, Cortellaro M, Rutsch W, Legrand V. Long-term fluvastatin reduces the hazardous effect of renal
impair-ment on four-year atherosclerotic outcomes (a LIPS substudy).Am J Cardiol
2005;95:445 – 451.
25. Nakamura H, Mizuno K, Ohashi Y, Yoshida T, Hirao K, Uchida Y. Pravastatin and
cardiovascular risk in moderate chronic kidney disease.Atherosclerosis2009;206:
512 – 517.
26. Ridker PM, MacFadyen J, Cressman M, Glynn RJ. Efficacy of rosuvastatin among men and women with moderate chronic kidney disease and elevated high-sensitivity C-reactive protein: a secondary analysis from the JUPITER (Justification for the Use of Statins in Prevention-an Intervention Trial Evaluating Rosuvastatin)
trial.J Am Coll Cardiol2010;55:1266 – 1273.
27. Stegmayr BG, Brannstrom M, Bucht S, Crougneau V, Dimeny E, Ekspong A, Eriksson M, Granroth B, Grontoft KC, Hadimeri H, Holmberg B, Ingman B, Isaksson B, Johansson G, Lindberger K, Lundberg L, Mikaelsson L, Olausson E, Persson B, Stenlund H, Wikdahl AM. Low-dose atorvastatin in severe chronic
kidney disease patients: a randomized, controlled endpoint study.Scand J Urol
Nephrol2005;39:489 – 497.
28. Tonelli M, Moye L, Sacks FM, Cole T, Curhan GC. Effect of pravastatin on loss of renal function in people with moderate chronic renal insufficiency and
cardiovas-cular disease.J Am Soc Nephrol2003;14:1605 – 1613.
29. Vernaglione L, Cristofano C, Muscogiuri P, Chimienti S. Does atorvastatin
influ-ence serum C-reactive protein levels in patients on long-term hemodialysis?Am
J Kidney Dis2004;43:471 – 478.
30. Fassett RG, Robertson IK, Ball MJ, Geraghty DP, Coombes JS. Effect of atorvasta-tin on kidney function in chronic kidney disease: a randomised double-blind
placebo-controlled trial.Atherosclerosis2010;213:218 – 224.
31. Rayner BL, Byrne MJ, van Zyl Smit R. A prospective clinical trial comparing
the treatment of idiopathic membranous nephropathy and nephrotic
syndrome with simvastatin and diet, versus diet alone. Clin Nephrol1996;46:
219 – 224.
32. Saltissi D, Morgan C, Rigby RJ, Westhuyzen J. Safety and efficacy of simvastatin in
hypercholesterolemic patients undergoing chronic renal dialysis.Am J Kidney Dis
2002;39:283 – 290.
33. Luciak M, Trznadel K. Free oxygen species metabolism during haemodialysis with
different membranes.Nephrol Dial Transplant1991;6(Suppl. 3):66 – 70.
34. Verma A, Ranganna KM, Reddy RS, Verma M, Gordon NF. Effect of rosuvastatin on C-reactive protein and renal function in patients with chronic kidney disease. Am J Cardiol2005;96:1290 – 1292.
35. Baigent C, Landray M, Leaper C, Altmann P, Armitage J, Baxter A, Cairns HS, Collins R, Foley RN, Frighi V, Kourellias K, Ratcliffe PJ, Rogerson M, Scoble JE, Tomson CR, Warwick G, Wheeler DC. First United Kingdom Heart and Renal Protection (UK-HARP-I) study: biochemical efficacy and safety of simvastatin
and safety of low-dose aspirin in chronic kidney disease.Am J Kidney Dis2005;
45:473 – 484.
36. Lins RL, Matthys KE, Billiouw JM, Dratwa M, Dupont P, Lameire NH, Peeters PC, Stolear JC, Tielemans C, Maes B, Verpooten GA, Ducobu J, Carpentier YA. Lipid and apoprotein changes during atorvastatin up-titration in hemodialysis patients
with hypercholesterolemia: a placebo-controlled study. Clin Nephrol 2004;62:
287–294.
37. Astor BC, Muntner P, Levin A, Eustace JA, Coresh J. Association of kidney func-tion with anemia: the Third Nafunc-tional Health and Nutrifunc-tion Examinafunc-tion Survey
(1988 – 1994).Arch Intern Med2002;162:1401 – 1408.
38. London GM, Guerin AP, Marchais SJ, Metivier F, Pannier B, Adda H. Arterial media calcification in end-stage renal disease: impact on all-cause and
cardiovas-cular mortality.Nephrol Dial Transplant2003;18:1731 – 1740.
39. Francis ME, Eggers PW, Hostetter TH, Briggs JP. Association between serum homocysteine and markers of impaired kidney function in adults in the United
States.Kidney Int2004;66:303 – 312.
40. Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, Kirby A, Sourjina T, Peto R, Collins R, Simes R. Efficacy and safety of cholesterol-lowering
Effects of statin therapy in patients with CKD
1817
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/
treatment: prospective meta-analysis of data from 90,056 participants in 14
ran-domised trials of statins.Lancet2005;366:1267 – 1278.
41. Lindner A, Charra B, Sherrard DJ, Scribner BH. Accelerated atherosclerosis in
prolonged maintenance hemodialysis.N Engl J Med1974;290:697 – 701.
42. Ribeiro S, Ramos A, Brandao A, Rebelo JR, Guerra A, Resina C, Vila-Lobos A, Carvalho F, Remedio F, Ribeiro F. Cardiac valve calcification in haemodialysis
patients: role of calcium-phosphate metabolism.Nephrol Dial Transplant1998;
13:2037 – 2040.
43. Herzog CA, Mangrum JM, Passman R. Sudden cardiac death and dialysis patients. Semin Dial2008;21:300 – 307.
44. Roselaar SE, Nazhat NB, Winyard PG, Jones P, Cunningham J, Blake DR. Detec-tion of oxidants in uremic plasma by electron spin resonance spectroscopy. Kidney Int1995;48:199 – 206.
45. Stenvinkel P, Heimburger O, Paultre F, Diczfalusy U, Wang T, Berglund L, Jogestrand T. Strong association between malnutrition, inflammation, and
athero-sclerosis in chronic renal failure.Kidney Int1999;55:1899 – 1911.
W. Houet al.
1817a
by guest on July 21, 2014
http://eurheartj.oxfordjournals.org/