Journal:
MEDIMA
Article
Number:
1350
Please
your
responses
and
any
corrections
to:
E-mail:
[email protected]Dear
Author,
Please
check
your
proof
carefully
and
mark
all
corrections
at
the
appropriate
place
in
the
proof
(e.g.,
by
using
on-screen
annotation
in
the
file)
or
compile
them
in
a
separate
list.
Note:
if
you
opt
to
annotate
the
file
with
software
other
than
Adobe
Reader
then
please
also
highlight
the
appropriate
place
in
the
file.
To
ensure
fast
publication
of
your
paper
please
return
your
corrections
within
48
hours.
Your
article
is
registered
as
a
regular
item
and
is
being
processed
for
inclusion
in
a
regular
issue
of
the
journal.
If
this
is
NOT
correct
and
your
article
belongs
to
a
Special
Issue/Collection
please
contact
[email protected]
immediately
prior
to
returning
your
corrections.
For
correction
or
revision
of
any
artwork,
please
consult
http://www.elsevier.com/artworkinstructions
Any
queries
or
remarks
that
have
arisen
during
the
processing
of
your
manuscript
are
listed
below
and
highlighted
by
flags
in
the
proof.
Click
on
the
‘
Q
’
link
to
go
to
the
location
in
the
proof.
Location
Query
/
Remark:
click
on
the
Q
link
to
go
in
article
Please
insert
your
reply
or
correction
at
the
corresponding
line
in
the
proof
Q1
AU:
The
author
names
have
been
tagged
as
given
names
and
surnames
(surnames
are
highlighted
in
teal
color).
Please
confirm
if
they
have
been
identified
correctly.
Please
check
this
box
or
indicate
your
approval
if
you
have
no
corrections
to
make
to
the
file
JID:MEDIMA [m5G;March15,2018;18:55]
Highlights
ContentslistsavailableatScienceDirect
Medical
Image
Analysis
journalhomepage:www.elsevier.com/locate/media
Graphical
Abstract
MedicalImageAnalysisxxx(2018)xxx–xxx
Vortical features for myocardial rotation assessment in hypertrophic cardiomyopathy using cardiac tagged magnetic resonance
SantiagoSanz-Estébaneza,∗,LucilioCordero-Grandeb,TeresaSevillac,
AnaRevilla-Orodeac,RodrigodeLuis-Garcíaa,MarcosMartín-Fernándeza,
CarlosAlberola-Lópeza
aLaboratoriodeProcesadodeImagen,DepartmentofTeoríadelaSeñaly ComunicacioneseIngenieríaTelemática,ETSIT,UniversidaddeValladolid,Campus MiguelDelibess.n.,Valladolid40011,Spain
bCentrefortheDevelopingBrainandDepartmentofBiomedicalEngineering,Division ofImagingScienceandBiomedicalEngineering,King’sCollegeLondon,StThomas’ Hospital,LondonSE17EH,U.K
JID:MEDIMA [m5G;March15,2018;18:55]
MedicalImageAnalysisxxx(2018)xxx–xxx
ContentslistsavailableatScienceDirect
Medical
Image
Analysis
journalhomepage:www.elsevier.com/locate/media
Vortical
features
for
myocardial
rotation
assessment
in
hypertrophic
cardiomyopathy
using
cardiac
tagged
magnetic
resonance
Santiago
Sanz-Estébanez
a,∗,
Lucilio
Cordero-Grande
b,
Teresa
Sevilla
c,
Ana
Revilla-Orodea
c,
Q1
Rodrigo
de
Luis-García
a,
Marcos
Martín-Fernández
a,
Carlos
Alberola-López
aaLaboratoriodeProcesadodeImagen,DepartmentofTeoríadelaSeñalyComunicacioneseIngenieríaTelemática,ETSIT,UniversidaddeValladolid,Campus MiguelDelibess.n.,Valladolid40011,Spain
bCentrefortheDevelopingBrainandDepartmentofBiomedicalEngineering,DivisionofImagingScienceandBiomedicalEngineering,King’sCollege London,StThomas’Hospital,LondonSE17EH,U.K
cUnidaddeImagenCardiaca,HospitalClínicoUniversitariodeValladolid,CIBERdeenfermedadescardiovasculares(CIBERCV),Valladolid47005,Spain
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received6June2017 Revised10January2018 Accepted14March2018 Availableonlinexxx
Keywords: Myocardialrotation Taggedmagneticresonance Vorticalfeatures
Hypertrophiccardiomyopathy
a
b
s
t
r
a
c
t
Leftventricularrotationalmotionisafeatureofnormalanddiseasedcardiacfunction.However,classical torsionandtwistmeasuresrelyonthedefinitionofarotationalaxiswhichmaynotexist.Thispaper re-viewsglobalandlocalrotationdescriptorsofmyocardialmotionandintroducesnewcurl-based(vortical) featuresbuiltfromtensorialmagnitudes,intendedtoprovidebettercomprehensionaboutfibrotictissue characteristicsmechanical properties.Fifty-sixcardiomyopathypatientsand twenty-twohealthy volun-teershavebeenstudiedusingtaggedmagneticresonancebymeansofharmonicphaseanalysis.Rotation descriptorsarebuilt,withnoassumptionaboutaregulargeometricalmodel,fromdifferentapproaches. Theextractedvorticalfeatureshavebeentestedbymeansofasequentialcardiomyopathyclassification procedure;theyhaveprovenuseful fortheregionalcharacterizationoftheleftventricular functionby showinggreatseparabilitynot onlybetweenpathologic andhealthypatients butalso, andspecifically, betweenheterogeneousphenotypeswithincardiomyopathies.
© 2018 Published by Elsevier B.V.
1. Introduction
1
Hypertrophic cardiomyopathy (HCM) (Maron et al., 2014) is 2
a relatively common heart muscle disease with a heteroge-3
neousphenotypicexpressionthatoccasionallyoverlapswithother 4
pathologiesthatalsopresentleftventricularhypertrophy. Differen-5
tiatingtheunderlyingetiology oftheventricularhypertrophy isa 6
frequentclinicalproblemwithrelevantimplicationssinceeach eti-7
ologyneedsaspecificmanagement andpresentsadifferent prog-8
nosis.HCMischaracterizedbyahypertrophiedandnondilatedleft 9
ventricle(LV)(Baron,2008),oftenwithanasymmetricalwall thick-10
ness distribution. HCMoccurs inthe presence ofmyocyte hyper-11
trophy andinterstitial and replacement fibrosis, which causethe 12
walls of the ventricles to thicken (Maron et al., 1992) and a re-13
duction on the cavity volume is usually observed. This thicken-14
∗ Correspondingauthor.
E-mail addresses: [email protected] (S. Sanz-Estébanez),
[email protected] (L. Cordero-Grande), [email protected] (R. de Luis-García), [email protected] (M. Martín-Fernández), [email protected] (C. Alberola-López).
URL:http://www.lpi.tel.uva.es/ssanest(S.Sanz-Estébanez)
ingmayblockbloodflowoutoftheventricle.Therefore,themain 15 features of a HCM heart summarize in increased LV mass and 16 thickenedwalls,especiallyintheinterventricularseptum(Urbano- 17
Moral etal., 2014). Theseabnormalities lead toalteredforces re- 18 vealingasignificant reductionin thediagonalcomponents ofthe 19 strain(Saltijeraletal.,2010).Previousstudieshaveshownthatre- 20 gionalLV dysfunctions predate over themorphologic changes re- 21 latedwiththephenotypicexpressionofhypertrophyandobstruc- 22
tion(Dhillonetal.,2014). 23
As previously stated, etiological factors are of great impor- 24 tanceinthecardiovascular diseasedetection(Maronetal.,2006). 25 Globalindices,suchasthegloballongitudinalstrain(Shimonetal., 26
2000), havebeen employed for cardiovascular disease identifica- 27 tion, reporting noticeable prognostic value; however, local mea- 28 surementscould providemore insight to the behavior offibrotic 29 tissue (Piella etal., 2010). Inthis direction, it hasbeen hypothe- 30 sizedthatthepresenceofgreatermyocardialtwistmaybeassoci- 31 atedwithagreaterdegreeofmyocardialfibrosisinHCMpatients. 32 Consequently,assessmentofLVrotationmechanicsasacharacter- 33 isticofcardiac functionmayhelp differentiatethepresenceoffi- 34 brosis(Young andCowan, 2012). Consistently withthese studies, 35 weadheretotheappropriatenessoflocalanalysesandtheirclini- 36
https://doi.org/10.1016/j.media.2018.03.005
calvalueonthebasis thatmostheartdiseasestypically affect lo-37
calizedregions of the myocardium. In addition,local studies can 38
beusedtoimprovecardiacanalytics,whichmayhelppredictthe 39
effectsofspecificcardiovasculardiseasesonthetissue. 40
Rotation parameters have recentlygained increasing attention 41
dueto their simplicityandease ofquantification;they constitute 42
interesting measures ofcardiac performance which provide addi-43
tionalinformation on myocardial mechanics as a complement of 44
standard pump function indices (Rüssel et al., 2009a). However, 45
most of the rotation parameters described in the literature im-46
plicitlyrequirean accuratedescription ofan axisofrotation.The 47
center of mass given by myocardial boundaries is widely used 48
assuch; however, the heart can translate during the cardiac cy-49
cle,whichcommonlyresultsinmisalignmentsofthecenteralong 50
subsequentframes, incurringinestimationerrors. Hence,non bi-51
asedcalculation methods,whichcompensatecentroidmotion,are 52
mandatory forthe use of LV torsionas a measure of myocardial 53
dysfunctionquantification(Senguptaetal., 2008). Still, additional 54
drawbackshavebeenreported;Young etal.(1994)statethat, for 55
HCM,theaxisofrotationisshiftedfromtheLVcenterofmass to-56
wards theinferoseptal region. In addition,for HCM patients, due 57
totheircharacteristicasymmetricalwallthicknessdistribution, ac-58
curatecentroidestimationcouldbecomeanextremelychallenging 59
task. 60
Imagingtechniquesprovideessentialinformationforthestudy 61
ofthesepathologies;severalmodalitieshavebeenproposedinan 62
effortto measureadvanced cardiac mechanics in the LV: speckle 63
tracking echocardiography (Helle-Valle et al., 2005; Bansala and
64
Kasliwalb, 2013), Cine Displacement Encoded (DENSE) Magnetic 65
Resonance Imaging (MRI) (Zhong et al., 2010) or traditional cine 66
Steady State Free Precession (SSFP) MRI, combined with feature 67
trackingtechniques,(Heermannetal.,2014),tomentionafew. Nev-68
ertheless,myocardialtissue tagging withcardiovascular magnetic 69
resonanceiscurrentlythegoldstandardforassessingregional my-70
ocardialfunction (Shehataetal.,2009).Ifitisnot widelyusedin 71
thedaily practiceis becauseit istime consuming, butto date is 72
anaccuratemethodtomeasureregionalcontractility(Jeungetal.,
73
2012).MR-Tagging(Ibrahim,2011) isusuallyperformedbyspatial 74
magnetizationmodulation(SPAMM)(AxelandDougherty,1989)or 75
avariant ofthistechnique. SPAMMis groundedon theability of 76
alteringthemagnetization ofthetissue (withinthelimitationsof 77
relaxationtimesinMR) eveninthepresenceofmotion.The tag-78
gingprocedureisbasedonthesuperpositionofaspatial modula-79
tionovertheappliedgradientswhichmaybesubsequentlytracked 80
throughoutthecardiaccycle,fromwhichthecardiacfunctioncan 81
beassessed. 82
Harmonic Phase (HARP) based methods (Osman et al., 2000) 83
arewidely used asamotion estimationtechniquein MR-Tagging 84
(MR-T).Thesemethodsarecapableofreconstructingdisplacement 85
fields accurately, grounded on the assumption of constant local 86
phase, which turns out to be more reliable than the constant 87
pixelbrightnessassumption.Thisapproachisbasedontheuseof 88
SPAMMtagpatterns,which modulatethe underlyingimage, pro-89
ducingasetofspectralpeaksintheFourierdomain.Eachofthese 90
spectralpeakscarry informationaboutaparticular componentof 91
tissuemotion,andthisinformationcan be extractedusingphase 92
demodulationmethods,obtainingtensorialdescriptorsof deforma-93
tionand,forourcase,rotationestimations. 94
Curlisadifferentialoperatorthatdescribestheinfinitesimal ro-95
tationofa vector field. Its directiondetermines the axisof rota-96
tionwhileitsmagnitudeshowstheamountofrotation.Theterm 97
vortex is commonlyassociated to a localized increased value on 98
themagnitudeofthegivencurlvector(thispropertywillbe here-99
afterreferred toasvorticity).The localrotation measured bythe 100
curloperatorshouldnotbeconfusedwiththebulkangular veloc-101
Table1
Demographicdataofthepathologicandhealthypatientsinthestudy(mean± std).
Patients HCM SLVH HealthyVol.
Numberofcases 39 17 22 Age 58± 16.3 69.8± 10.5 49.2± 21.8 Sex(M/F) 27/12 12/5 14/8 EjectionFraction(%) 70.4±5.4 69.7± 6.1 63.6± 6.5 DiastolicLVvolume(ml) 140.6±22.8 131±50.3 150.3±31.5 SystolicLVvolume(ml) 42± 9 41.8 ±22.4 53.8± 13.9 Wallthickening(%) 78.4±20.1 79.8± 18.6 89.6± 16.9
ityvectorobservedwithinthemyocardialtissuewithrespecttoa 102
fixedcardiacaxis. 103
Numerous 4D phase-contrast MRI (Köhler et al., 2013) stud- 104 ies havemade useof thecurl operator. Flow vortical patternsin 105 the heart chambers, the aorta, the carotid sinus and pulmonary 106 circulation are physiological, but can also be related to certain 107 pathologies including aortic aneurysms, pulmonary hypertension 108 andcongenitalheartdefects.Vorticalpatternsoftenoccurbecause 109 of morphological alterations, vessel widenings or after stenosis 110 (von Spiczaketal.,2015).Thesestructuresmayalterthepressure 111 andshearforcesonthewallsandtriggerprocessesleadingtocell 112
death. 113
Itisourunderstandingthatcurlcanalsoquantifythelocalro- 114 tationwithinthemuscle.Consequently,inthispaperweintroduce 115 a novel local rotation descriptor based on robust tensorial mea- 116 surements that relates the presence of increased vorticity values 117 with the hypertrophic tissue in the heart. Rotation is estimated 118 withoutinfluenceofglobalmyocardialparameters,such asaxisof 119 rotationorcavityradius,allowingaregionalcomparativestudyin 120 patientswithLVhypertrophyofdifferentetiologies;HCMandSec- 121 ondary forms of LV Hypertrophy (SLVH), as well ashealthy sub- 122 jects.Tothebestofourknowledge,thisisthefirststudythatre- 123 lateslocalvorticesinmyocardialtissuewiththepresenceoffibro- 124
sis. 125
2. Materials and methods 126
2.1. Materials 127
Forthevalidationoftheproposedapproach,ourstudyisaret- 128 rospectiveanalysisbasedonadatabaseofpatientswhounderwent 129 the ordinary clinical protocol according to their symptoms; the 130 databaseconsistedin 78individualswho were affectedby either 131 primary HCMorSLVH (hypertensiveheart disease,aorticstenosis 132 orathlete heartdisease)orwere healthyvolunteers. Thenumber 133 ofpathologic patientswas56; 39ofthem, withages from30to 134 86, were diagnosed asprimary HCM. These patientsshowed hy- 135 pertrophy,predominantlyintheseptalregionoftheLV.Following 136 thesame protocol,17patientswere diagnosed ofSLVHaccording 137 to chronic pressure overload. The differential diagnosis between 138 primaryHCM andSLVHwasbasedonpreviousechocardiopraphic 139 studiesandclinical andfamilialrecords.Aboutthehealthyvolun- 140 teers,22wereincludedinthestudywithagesbetween16and84; 141 thesesubjectsunderwenttheMRI protocolbecauseofaprevious 142 suspicion of cardiac pathology but all of them turned out to be 143
healthy. 144
All subjectssigned the ordinary informed consentfor theMR 145 sessionandagreedinwritingtosharetheresultingimagesforre- 146 search purposes. Personaldata were treatedaccording tocurrent 147 legislation.Demographicdataofbothcontrolsandcases,thelatter 148 indexedbypathologytype,aregiveninTable1. 149 We have acquired short axis (SA) and long axis (LA) MR-T 150 datasetsforeachpatient, fromapexto base,usingaMRComple- 151 mentary SPAMM(C-SPAMM) SENSitivity Encoding (SENSE) Turbo 152
S.Sanz-Estébanezetal./MedicalImageAnalysisxxx(2018)xxx–xxx 3
JID:MEDIMA [m5G;March15,2018;18:55]
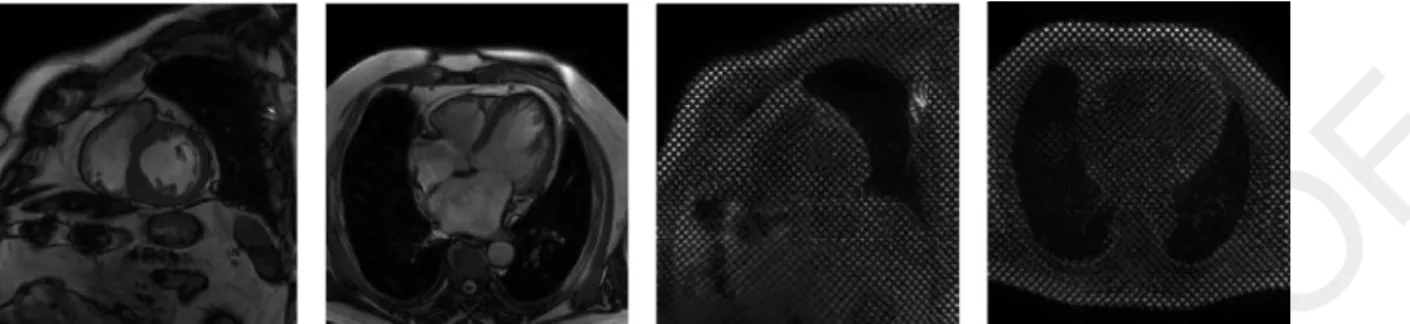
Fig.1. Exampleimagesofthesequencesacquiredforthestudy.MR-CineSA,MR-CineLA,MR-TaggingSAandMR-TaggingLA,fromlefttoright.
Table2
DetailsonthesequencesofMRimagesusedinthepaper.p:ReconstructedPixelResolution(mm).s:SliceThickness(mm).Np:Numberofpixelsfordimension.Nt: NumberofTemporalPhases.Ns:Numberofslices.TR:RepetitionTime(ms).TE:EchoTime(ms).α:FlipAngle(degrees).
Parameters p s Np Nt Ns TR TE α
MR-TSA 1.21-1.32 10 256–432 16–25 10–15 2.798-6.154 1.046-3.575 7–25 MR-CSA 0.96-1.18 8–10 240–320 30 10–15 2.902-3.918 1.454-2.222 45 MR-TLA 1.21-1.34 10 240–340 15–27 1–3 2.903-4.507 1.097-2.897 10–45 MR-CLA 0.98-1.25 8–10 256–448 30 1–3 2.858-3.529 1.251-2.132 45
Field Echo sequence on a Philips Achieva 3T scanner. Regarding 153
the tagging parameters, we validate the method for a fixed tag 154
spacing of k i = 1/
λ
, withλ
=7mm using two differentorienta-155
tions U i=
(
cos(
θ
i)
;sin(
θ
i))
withθ
=[π
/4;3π
/4]forthestripedi-156
rections. 157
Additionally, we have also acquired a balanced SSFP SA MR-158
Cine(MR-C)sequenceatthesamespatiallocationforeachpatient; 159
snapshotsoftheacquiredsequencesare showninFig.1.The my-160
ocardium has beensegmentedin theend-diastolic (ED) phaseof 161
the MR-C sequence by two cardiologists. Cine segmentations are 162
usedtoalignthetaggingorientationstoacommonreference sys-163
tem to correct for patient motion.The ED segmentation is used 164
to define a region of interest (ROI) in which to compute mean-165
ingfulmeasurements.Resolutiondetailsaboutthesesequencesare 166
includedinTable2. 167
2.2. Methods
168
2.2.1. Preprocessing
169
Wehaveimplemented apreprocessingpipelineinorderto(a) 170
propagatetheROIinMR-CfromEDtotheend-systolic(ES)phase 171
—in which subsequent calculations will be carried out— and (b) 172
aligntheMR-CandMR-TsequencesatES.Thesetwostepsare: 173
• Registration The MR-C sequence is processed by means of a 174
groupwiseelasticregistrationprocedure(Cordero-Grandeetal.,
175
2013a)inordertopropagatetheEDsegmentationstowardsES 176
phase. The transformation is achieved by B-spline based Free 177
Form Deformations (FFD) (Rueckert et al., 2006). A gradient-178
descent optimization scheme is performed where the sumof 179
thesquareddifferencesofimageintensitiesisusedas registra-180
tion metric. A smoothness penalty term has also been intro-181
ducedto constrain the spline-based FFDtransformation to be 182
smooth. 183
• AlignmentAnaffine registrationmethodisperformedtoalign 184
MR-T and MR-C images at ES phase. The MR-T sequence has 185
beendetaggedbymeansofahomomorphicfilteringprocedure 186
(Makrametal.,2015)priortothealignmentprocess. 187
2.2.2. Motion estimation
188
3D HARP motion reconstruction using the C-SPAMM tech-189
nique requires a minimum of 3 linearly independent wave vec-190
tors (Osmanet al., 2000). We haveextended theaforementioned 191
HARPmethodologyforthecomputationofthedeformation gradi- 192 enttensorusingSAandLAimagesontheintersectionoftheslices 193 asshowninFig.2.ForpointsonwhichLA axisimageswere not 194 available,2D motion hasbeenreconstructed. The motionestima- 195 tiontechniqueisbasedontheextractionofthelocalphaseofthe 196 gridpatternaccordingtothemethodpresentedinCordero-Grande 197
etal.(2011,2016).AwindowedFourierTransform(WFT)isapplied 198 to the image at ES phase. The WFT provides a representation of 199 theimagespectruminthesurroundingsofeachpixeloftheorig- 200 inalimage,soHARPbandpassfilteringtechniquescanbedirectly 201 appliedon thespatially localizedspectrum oftheimage. Toade- 202 quatelyretrievetheshapeofthespectral peaks,wehaveresorted 203 toananisotropicfilteringapproachcombiningGaussianband-pass 204 andall-pass filters asproposed in Sanz-Estébanez et al.(2016a). 205 Finally,eachoftheimagephase
ϕ
i (x )(twoforeachplane)canbe 206 extractedinthespatialdomainfromtheinverseWFToftheafore- 207mentionedfilteredspectrum. 208
As mentioned before, we have extended the HARPmethodol- 209 ogy by allowing the estimation of motion under the application 210 of a set of four wave vectors. Therefore, 3D deformation gradi- 211 ent tensor can be robustly recovered at the intersection points 212 ofbothaxes, byapplyingthemethodology presentedinCordero- 213
Grandeetal.(2016).Thematerialdeformationgradienttensor F (x ) 214 canbe estimatedfromthe gradientofthe phaseimage asstated 215
inOsmanetal.(2000)as: 216
K=
∂ϕ
∂
x(
x)
F(
x)
=Y(
x)
F(
x)
, (1)where K representsthetwostripeorientationsoffourgivenwave 217 vectorscorresponding toeach taggedimage.Robustestimationof 218
F (x )isachievedthroughLeastAbsoluteDeviation(LAD)procedure. 219 The reconstruction is performed via Iteratively Reweighted Least 220
Squares(IRLS): 221
Fl+1
(
x)
=(
YT(
x)
Wl(
x)
Y(
x))
−1YT(
x)
Wl(
x)
K, (2)with W l (x )adiagonalweightingmatrix,whichisupdatedateach 222 iteration by considering fitting residuals (Cordero-Grande et al., 223
2016). 224
Fromthisestimatedtensor,themaincardiacfunctioncharacter- 225 isticscanbeobtainedthroughtheLagrangianstraintensor,defined 226
as: 227
E
(
x)
=1 2(
F(
x)
Fig.2. Thefigureontheleftsketchestheproposed3DHARPmotionreconstructionschemefortheintersectedpointsbetweenSAandLAplanes,whichareshowninthe figureontherightovertheSA.
The spatial resolution of the reconstructed tensors depends on 228
thewidthoftheHARPband passfilter(ParthasarathyandPrince,
229
2003;2004);theHARPmethodisupperlimitedbyhalfofthetag 230
spacing(smalldeformation assumption). However, WHARP meth-231
ods(Sanz-Estébanezetal.,2016a;Cordero-Grandeetal.,2016) try 232
toaccommodatethebandpassfiltertothelocalfrequencyofthe 233
signalinordertoapproachtothemaximumachievableresolution. 234
Therefore,effectiveHARPresolution willvary dynamically, allow-235
inglargedeformations,asthoseobservedatES,beingcapturedat 236
amaximalscaleof1.5timeshalfthetagspacing. 237
These tensors have been calculated atES, where the greatest 238
deformationalongthecardiaccycletakesplace. 239
2.2.3. Rotation parameters
240
Inaddition tothickeningandshortening,themyocardium also 241
undergoes a wringing motion during systolic phases due to the 242
obliquely oriented subendocardial and subepicardial myofibers. 243
Manydescriptorshavebeenproposedtomeasurethismotionthat 244
relyoneitherglobalinformationderivedfromsimplified anatomi-245
calmodelsorontensorialstrainanddeformationmagnitudesbuilt 246
fromlocalmotionestimates. 247
Measures based on global information. It is well known that the 248
LVapexgloballyrotatesanticlockwiseata relativelyconstantrate 249
throughoutsystole.Onthecontrary,thebase,initiallyrotating an-250
ticlockwise,reverses directionproviding a net clockwiserotation 251
atESphase. Theresulting differenceofthese twomotions is de-252
fined as twist, defined to be positive by convention (Young and
253
Cowan,2012). 254
Thereiscurrentlyalackofstandardizationformethodsusedto 255
characterizetheglobalLV twisting motion.Thesedescriptorsrely 256
ongeometricalmodels oftheheart fortorsionandtwist calcula-257
tion.Consequently,both a well-definedfixed axisofrotation and 258
regularmyocardial radiiover thewhole heartare mandatory.For 259
example,torsion has been traditionally calculated as relative ro-260
tationindegrees(Lorenzetal., 2000), rotationper length in de-261
grees/mm,torsionalshear angle,alsoin degrees(Buchalteretal.,
262
1990), and longitudinal-circumferential shear strain (dimension-263
less)(Fung,1965).Traditionalrotationindicesareobtainedby vec-264
torial product between position vectors at ES u ES and ED u ED 265
phasesas: 266
sin
(
β
)
=|
uED ×uES|
|
uED||
uES|
. (4)As statedabove,twistcomputationdependsontheexact loca-267
tions ofthe apical and basal slicesand requires accurate motion 268
compensation,specially forcentroidmotion correction. Twist per 269 unit lengthisalsowidespread, sincetorsionisrelatively constant 270 in the longitudinaldirection (Young and Cowan,2012). Nonethe- 271 less, thismeasuredoesnotscale appropriately betweenhearts of 272 differentsizesandwehavenotobservedasignificantcomplemen- 273 taryvaluewithrespecttothetwist. 274 The torsional shear angle is a measure of the change in an- 275 gle between line segments which are initially aligned with the 276 anatomical axes of the LV. Many studies have used the formula 277 given by Aelen etal. (1997). However, it hasbeen demonstrated 278 thatitusuallyoverestimatesdeformation(Rüsseletal.,2009b),so 279 wehaveresortedtoanunbiasedalternativeformulabasedoncir- 280
cumferentialdisplacements: 281
T =
(
β
apex r apex −β
base r base)
D , (5)
where D is the distance between selected segments.1 However, 282
HCMcharacteristicendocardialirregularitiesmayhindertheaccu- 283 rateestimationofboth themyocardialradiusandtheaxis,which 284
arecrucialinthisformulation. 285
Tensorial descriptors. Anotherimportantgroupofrotationdescrip- 286 tors focus on the properties of the tissue that provide localized 287 characterization of the motionby tensorial analysis.As stated in 288 solidmechanics(Fung,1965),the3D strainstateatanypointina 289 bodycan befullyrepresentedbythreediagonalstrainsandthree 290 shear strains. From them, the longitudinal-circumferential shear 291 (E lc )isausefulmeasurecloselyrelatedtotorsion.Accordingtothis 292 analysis, local torsion measures can be defined, i.e., the 3D local 293
torsionshearcanbegivenby: 294
sin
(
θ
lc)
=√ 2 E lc 1 +2 E cc 1 +2 E ll, (6)
where E cc and E ll represent the circumferential and longitudi- 295 nal strains, respectively; these components can be obtained by 296 straightforward operations on the Cartesian components in (3). 297 Nevertheless,shear strainsareseveralmagnitudes lower thandi- 298 agonalstrains,sofactorsotherthaninotropicstatemaygreatlyaf- 299 fectitsestimation(Petitjeanetal.,2005). 300 Angular variation between two states of stress in the plane 301 inCartesian coordinates can beexpressed by a singleangle
φ
as 3021Rotationparameterβ hasbeenpixelwiseestimated;therefore,rotation mea-suresexpressedon(5)arereferredtothemedianoftherotationdistributionon basalandapicalsegments.
S.Sanz-Estébanezetal./MedicalImageAnalysisxxx(2018)xxx–xxx 5
JID:MEDIMA [m5G;March15,2018;18:55]
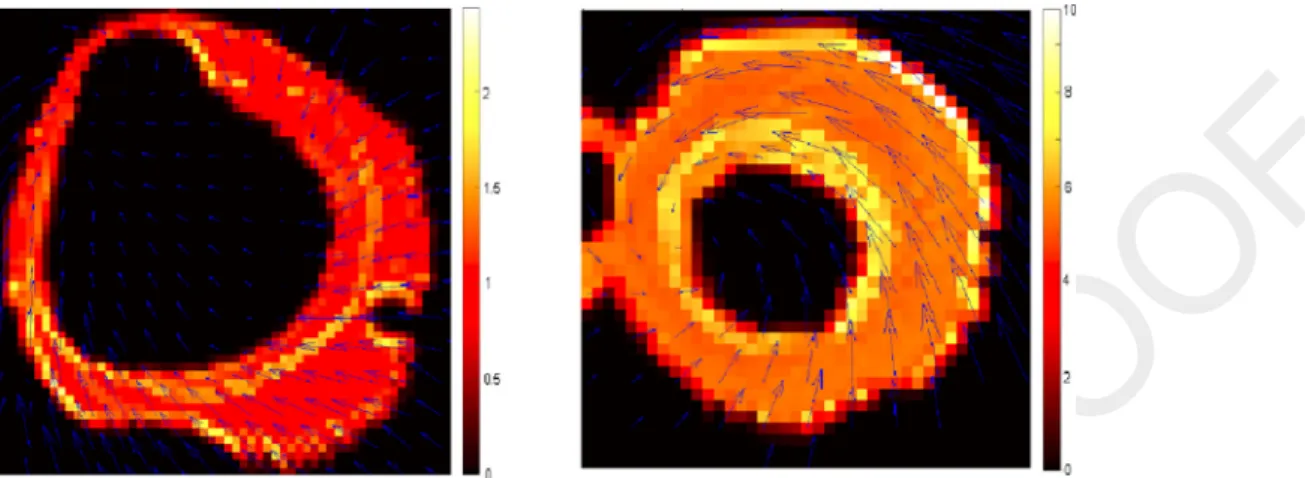
Fig.3. ExamplesofvorticityvectormodulusatESfrom(9)inbasalandapicalslices,leftandrightrespectively.Thearrowsshowtheextractedcardiacdisplacementfield whilethecolourrepresentstheintensityofvorticity(unitless).SomeoutliersareobservedneartheboundariesduetothedifficultyofHARPmethodsintrackingmaterial pointsinthepresenceofgreatintensitychanges.Scalesaresettobestaccomodatetherangeofvaluesonthegivencardiacplane,sincemyocardialrotationvariesin modulusanddirectionalongthecardiacaxis.
statedinFung(1965): 303
tan
(
2φ
)
=ε
2ε
xyxx −
ε
yy , (7)where
ε
representstheCauchy’s straintensor (ε
) directly related 304withthe stresstensor bythe Lamé parameters(Fung,1965). Par-305
ticularvaluesof
φ
showangularvariationofstressprincipal direc-306tionsbetweenbothstates(ESandEDphases). 307
Additionally,in Cordero-Grandeetal.(2013b) a novelrotation 308
parameter hasbeenproposed builtfromthe (longitudinal) trans-309
formationthatsuffersalocalcoordinateatEDthroughtimeinthe 310
LR planeasgivenbythematerialdeformationgradienttensor F . 311
α
LRl = arctan(
−Flr /F ll
)
. (8)Ourworkellaborates onvorticalpatternswidelyemployed for 312
theidentificationofabnormalflowpatterns.Nonetheless,theterm 313
vortex bearsdifferent interpretations asdefined inthe literature. 314
Formostflowstudiesperformedinclinicalpractice,theterm vor-315
tex denotes rotating motion, where stream or pathlines tend to 316
curl back onthemselves (Markl etal., 2011). Influid dynamics,a 317
vortexisaregioninafluidinwhichtheflowisrotatingaroundan 318
axisline,whichmaybestraightorcurved.Moreexplanatorynotes 319
on the theoretical definitionof the term vortex can be found in 320
Stalderetal.(2010).Inthispaper,thetermvortexwillbeusedin 321
thesolid mechanics contextasalocalabnormallyincreased rota-322
tioncomponent. Inordertofindevidenceofperturbations within 323
themyocardialtissue,materialvorticalpatternscanthenbe asso-324
ciated to increased valuesof an dynamicrotation parameter ex-325
tractedfromthedeformationgradienttensor. 326
Thecurlofagivendeformationfield u describeslocalspinning 327
vectors(seeFig.3)andcanbecalculatedas: 328
ω
(
t)
=ω
x
(
t)
ω
y(
t)
ω
z(
t)
=1
2
∇
×u(
t)
= 1 2⎛
⎜
⎜
⎜
⎝
∂
u z∂
y −∂
u y∂
z∂
u x∂
z −∂
u z∂
x∂
u y∂
x −∂
u x∂
y⎞
⎟
⎟
⎟
⎠
= 1 2
Fzy −F yz F xz −F zx F yx −F xy
(9)
where F ab represents a component of the material deformation 329
gradient tensor in Cartesian coordinates. Hereinafter, vortical pa-330
rameterswillbeexpressedinCartesiancoordinatesasopposedto 331
thecylindricalcoordinatesfromthestraintensorusedin(6). 332
In this paper we hypothesize that local increasing of vortic- 333 ity values (in modulus) arises within myocardial segments with 334 fibrosis-relatedperturbations.Nonetheless,highvorticityvalues,ir- 335 respectiveofthefibrosisdegree,arepronetoappearinmyocardial 336 boundaries,givingrisetomultipleoutliersinrotationestimation. 337 Thesevorticitymeasuresareinsensitivetothedefinitionofthe 338 rotationaxis,although3D deformationsare neededforits proper 339 reconstruction.WhenLAinformationisnotavailable,onlythelon- 340 gitudinalcomponent(
ω
z )ofthevorticityvectorcanbeestimated. 341 In addition, if the cardiac axis is not planned properly, vorticity 342 parameters will be estimated with a systematic error related to 343 theangularerroroftheaxis.However,asitiscommoninclinical 344 practice,wewillassume thatthemainaxisofrotationwilllie on 345 theLAplanes(i.e.,willbenormaltotheSAimageplanes).Hence, 346 theω
z componentofthevorticityvectorprovidesclinicalcompli- 347 anceasitisalignedwiththewringingmotionofmyocardialfibers. 348 Thus,aphaseincrementduetotheaforementionedlocalrotation 349canbeextractedbyintegration: 350
t ES
t ED
ω
z(
t)
d t =ϑ
(
t ES)
−ϑ
(
t ED)
=ϑ
(
t ES)
≈ω
z(
2 t ES)
(
t ES −t ED)
.(10)
This parameter will be referred to as local rotation ϑ. Therefore, 351 twistmotionwillbeapproximatedas 352
Twist
ϑ
=|
ϑ
base−ϑ
apex|
(11)Forcomparative purposes,wewillalsoestimate ϑand
β
rota- 353 tiondistributionswithtwootherdifferentmethodologies.First,we 354 willanalysethecapabilitiesoftheelasticregistrationalgorithmde- 355 scribedinSection2.2.1appliedtoMR-Ctodetectrotationfromthe 356 estimateddeformationfields.Second,wehaveemployed anatlas- 357 based approach that consists of a spheroidal model (Young and 358Axel, 1992) fitted at ED and that deforms due to the forces ex- 359 ertedfromastripetrackingprocedure(Young etal., 1995) onthe 360 MR-Tsequencethroughoutthecardiaccycle.Deformationsarefor- 361 mulatedfromcontinuousparameterfunctionswhich,in addition, 362 include parameterized twisting and rotation axis deformation as 363 givenin Park et al. (1996)and, therefore,can be applied to any 364
shape. 365
2.2.4. Classification 366
We have resorted to a classification method (Sanz- 367
Fig.4. Pipelineforthefeatureselectionandclassificationstages.
to classify heterogeneous groups of ventricular hypertrophy (and 371
controls) from myocardial functional descriptors. The proposed 372
classification method is grounded on the idea that populations 373
overlap strongly irrespective of the specific features selected for 374
classification ifthe problemis addressed through a singlestage. 375
Our purpose is to classify a sample into one of three classes, 376
namely,control, primaryHCMandsecondaryhypertrophy(SLVH). 377
Sincesecondaryhypertrophypatientshavesubtledifferenceswith 378
respecttotheother twoclasses,wehaveresortedto atwo-stage 379
classification procedure. Thus, we have divided the classification 380
process in three stages and performed a feature selection step 381
for each stage independently, following a sequential methodol-382
ogythat adapts to the characteristics of the population at every 383
stage. Different machine learning methods (both supervised and 384
unsupervised)havebeenimplementedforeachstageandalltheir 385
possiblecombinationshavebeentested. 386
Mechanicaldescriptorsextractedfromtheaforementioned ten-387
sorsarean essentialpartoftheclassification procedure.Wehave 388
considered different groups of features. First, the components of 389
the strain tensor in the cylindrical coordinate system {R , C , L } 390
are accounted for. We also use twist and torsion features (see 391
Table 3) built from the aforementioned rotation parameters as 392
extracted from the MR-T and MR-C sequences, as well as using 393
thespheroidalmodelwehavepreviouslyreferredto.Additionally, 394
since some rotation-related componentshave opposite directions 395
inapexandbase,weconsiderthelocationofthezerocrossingfor 396
thesecomponentsaswell. 397
For the feature extraction step, we have previously se- 398 lected for each feature the mostrepresentative cardiac segments 399 (Cerqueira,2002)withinclinicalpractice.Fortwistandtorsionde- 400 scriptors,wehaveconsidered septalsegments,whereas fortenso- 401 rialparameters,mid-ventricularorbasalsegments havebeencho- 402 sen.InTable3weshow thesegments involvedinthecalculation 403 ofeachofthe features;then theoverall featureis,forrobustness 404 purposes, the median of the distribution within those segments, 405 which will be the input to the classifier. For the twist parame- 406 ters the feature extracted is the difference between medians on 407 apical andbasal septalsegments.Ontheother hand,forthezero 408 crossingparameter,thefeaturerepresentstheheightofthecardiac 409 axisatwhichthegivenrotationparameter,estimatedslicebyslice, 410 changesitssign.Noticethatthefeatureextractionstepisgrounded 411 onclinicalknowledge,i.e.,itisnotdata-driven. 412 As reflected in Fig. 4, after feature extraction we carry out a 413 normalizationstageinordertodiminishtheinfluenceofpossible 414 outliers. A sigmoidal function, withits scale factorset according 415 toTheodoridis andKoutroumbas(1999),isusedtothisend. Data 416 aremappedontheinterval(0,1)byimposingageneralizedlogistic 417 function;outlierswilltendtoappearateitherofthetwoextremes, 418 whilemaintaininga linearrelationfortherestofthe data.Then, 419 normalizedfeaturesarearrangedinvectorswithdifferentnumber 420
S.Sanz-Estébanezetal./MedicalImageAnalysisxxx(2018)xxx–xxx 7
JID:MEDIMA [m5G;March15,2018;18:55]
Table3
Cardiacsegmentsinvolvedduringthefeatureextractionstageforeachoneofthemotiondescriptorsemployedintheclassificationprocedure.Foreachrow,onlyonefeature willbeextracted,summarizingallthesegmentsindicatedbelow.Theextractedfeatureswillbetheinputtothefeatureselectionstep,fromwhichthefinal(survivor)feature vector(from2to5components)willarise.Thenumberwithinbracesindicatestheequationthatdefinestheparameter.
Segment 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Err(3) √ √ √ √ √ √
Ecc(3) √ √ √ √ √ √
Ell(3) √ √ √ √ √ √
Elc(3) √ √ √ √ √ √
||ω||(9) √ √ √ √ √ √ √ √ √ √ √ √
Twistϑ(11) √ √ √
Twistβ(4) √ √ √
Twistφ(7) √ √ √
T(5) √ √ √ √ √ √ √ √ √ √
αLRl(8) √ √ √ √ √
θlc(6) √ √ √ √
ωzzerocross.(9) √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ βzerocross.(4) √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √
ofcomponents(2through5).Allpossiblecombinationsoffeatures 421
indicatedinTable3havebeentested. 422
Featureselectionandclassificationperformanceassessmenthas 423
beencarriedoutinasimilarbutsequentialmanner.Forboth,data 424
samples have been randomized and a Leave-10-out method has 425
been applied; the proportions of control/primary/secondary have 426
been keptunaltered alongtrials. Specifically,forfeature selection 427
inthefirstclassificationstage,weclassifythesamplesincontrols 428
andprimariesandcalculatetheaccuracy;thefeaturesetwiththe 429
highestfigureisselectedforthisstage.Inparallel,andforthe sec-430
ond stage, controlsand secondaries are classified on one branch 431
(left branch) andprimariesand secondarieson theother branch. 432
In thiscase, features are selectedwith the criterion of maximiz-433
ing the sensitivitytosecondaries soasto avoidbias towardsthe 434
groupswithlargersamplesize,speciallybetweenHCM andSLVH. 435
Thisprocedure hasbeenlabelledin Fig.4as K-fold Feature Selec-
436
tion .Asforfindingclassification performance,asimilarcross vali-437
dationprocedurehasbeencarriedout(labelledinFig.4as Leave-
438
10-out Classification ) onnewrandomizations.Theclassifierstested 439
havebeenFuzzyc-Means(FCM)(Bezdec,1981)andSupportVector 440
Machines (Cortes and Vapnik,1995) both withquadratic (SVMq) 441
andGaussian(SVMg)kernels(Vertetal.,2004). 442
In order to assess the performance of a given feature in the 443
classification procedure we have measured its surviving percent 444
rate. This parameter shows the membership probability of the 445
givenfeature tothe featurevector extractedfromthefeature se-446
lectionstep;inotherwords,itisthefrequencythatthefeatureis 447
employedwithinanyofthestagesoftheclassificationalongtrials. 448
3. Results
449
3.1. Rotation analysis
450
Torsionis knownto be dependent onLV shape,with reduced 451
twistinmoresphericallyshapedheartsandincreasedtorsionwith 452
concentrichypertrophyduetoanincreasedleverarmfor myocar-453
dial fibers.InHCM, torsionhasbeenreportedtoincrease despite 454
reduced circumferential and longitudinal shortening (Young and
455
Cowan, 2012). These findings, together with others described in 456
Section1,canbeobservedintheresultsincludedinTable4,where 457
the mean and standard deviation of the twist and torsion dis-458
tributions derived from the aforementioned rotation features are 459
shown. 460
In Fig. 5 we show snapshots of mid-ventricular slices of the 461
local rotationextractedby means ofthevorticalapproach as de-462
scribedin(10)foraHCMandaSLVHcaseaswellasforahealthy 463
volunteer.Ingeneral,septalsegmentsforHCMhaveshownhigher 464
vorticity,speciallywhencomparedtolateralsegments,whereasfor 465
Table4
TwistandtorsionparametersextractedfromtheMR-Tsequence(mean ±std)for segmentsinTable3foreachpopulation.Thenumberwithinbracesindicatesthe equationthatdefinestheparameter.
Populations HCM SLVH Control
Twistϑ(11) 10.46±2.11 9.23±2.28 7.33±2.08 Twistβ(4) 13.53±2.50 13.80±3.37 9.87±2.81 Twistφ(7) 2.73±0.53 2.71±0.64 1.25±0.072 T(5) 7.26±1.14 6.85±1.90 4.63±1.68 Elc(3) 0.02±0.003 0.022±0.01 0.011±0.006
θlc(6) 7.94±1.66 7.22±1.81 3.18±0.39
αLRl(8) 1.83±1.57 2.08±1.98 2.82±1.79
secondarycases thisbehavior canbe observed inanyofthe car- 466 diacsegments.Inhealthyvolunteerstheextractedvaluesarelower 467 comparedtoHCMpatientsindependentlyofthecardiacsegment. 468 In Fig. 6, we show color codes of the mean ± standard 469 deviation (respectively, inner and outer rings within each seg- 470 ment) of the rotation parameters over the 17-segment model 471 (Cerqueira,2002),estimatedfromboththevorticalapproachgiven 472 in(10) and thetraditional approach by (4) forthe resulting dis- 473 tributionofthedeformationvector field.Additionally,andforthe 474 sakeofcomparison,rotationparametersextractedwiththeelastic 475 registrationprocedure overMR-Candfromthedeformablemodel 476 havebeenincludedaswell inthesecond andthird rows,respec- 477
tively. 478
Studentt-tests2 have been performed to highlight differences 479
onthemeanofthevorticitymodulusandtheaforementionedro- 480 tationdistributionsoneachofthe17cardiacsegments.Eachpop- 481 ulationofthestudyhasbeencomparedwiththeothertwo,sepa- 482 ratelyforeachrotationparameter;thenumericalresultsareshown 483 inTable5andgraphicallyinFig.7bull’seyedisplay.Itisnotice- 484 able that the vorticalapproach seems to show larger differences 485 betweenpopulations compared to the traditional approach. Sep- 486 tal segments seem to bear higher discriminating capability, spe- 487 ciallywhentwistismeasured bythevorticalapproach.Addition- 488 ally,wehaveperformed(two-way)ANOVAtestsovertheϑdistri- 489 butionsextractedfromMR-CandMR-Tsequencesaswellasusing 490 the deformable model (over MR-T) for each population and car- 491 diacsegment. Significant differences(p <10−3) have beenfound 492
inthevastmajorityofthecomparisons.ϑand
β
distributionswere 493 notcomparedsincethemeasuredparametersdonotrepresentthe 494 samecomponentofthephysiologicalrotationmotion. 495Fig.5. Snapshotsonvortical-basedrotationmeasurementωzfrom(9)forHCM,SLVHandahealthyvolunteerovermid-ventricularslices(fromlefttoright).
Fig.6. RegionalstudyoftheaforementionedvorticalrotationparametersobtainedfromtheMR-CandMR-Tsequences,aswellasusingthedeformablemodeloverthe latter,forthedifferentpopulations.Traditionalrotationisalsodepictedinthelastrow.Foreachcardiacsegmenttwocolorsaredepicted,theinnershowingmean+stdand theouterformean−std.
S.Sanz-Estébanezetal./MedicalImageAnalysisxxx(2018)xxx–xxx 9
JID:MEDIMA [m5G;March15,2018;18:55]
Table5
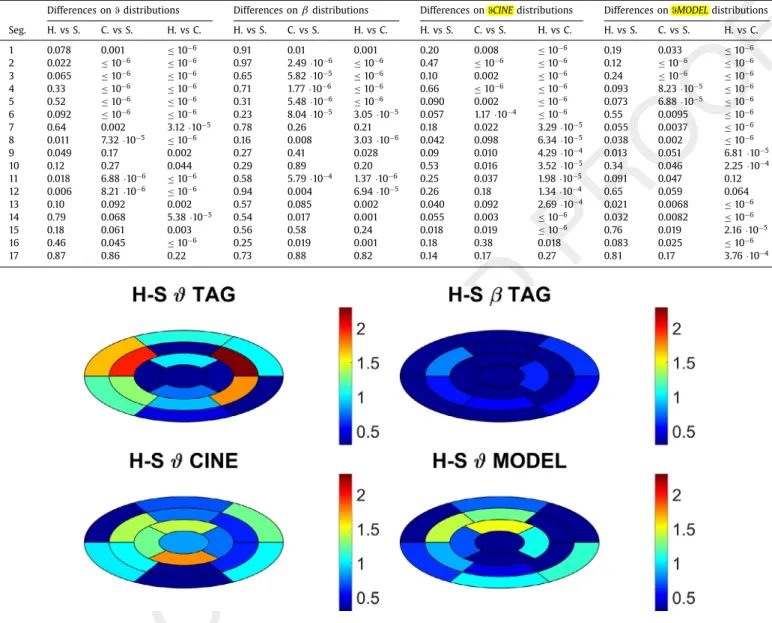
p-valuesforthecomparisonsbetweendistributions(H,SandCstandforHCM,SLVHcasesandcontrols,respectively)ofthegivenrotationparametersindexedbynumber ofsegment.Whenunspecified,MR-Tistheimagesource.SignificancelevelafterBonferronicorrectionis0.017.
Differencesonϑdistributions Differencesonβdistributions DifferencesonϑCINEdistributions DifferencesonϑMODELdistributions
Seg. H.vsS. C.vsS. H.vsC. H.vsS. C.vsS. H.vsC. H.vsS. C.vsS. H.vsC. H.vsS. C.vsS. H.vsC.
1 0.078 0.001 ≤10−6 0.91 0.01 0.001 0.20 0.008 ≤10−6 0.19 0.033 ≤10−6 2 0.022 ≤10−6 ≤10−6 0.97 2.49·10−6 ≤10−6 0.47 ≤10−6 ≤10−6 0.12 ≤10−6 ≤10−6 3 0.065 ≤10−6 ≤10−6 0.65 5.82·10−5 ≤10−6 0.10 0.002 ≤10−6 0.24 ≤10−6 ≤10−6 4 0.33 ≤10−6 ≤10−6 0.71 1.77·10−6 ≤10−6 0.66 ≤10−6 ≤10−6 0.093 8.23·10−5 ≤10−6 5 0.52 ≤10−6 ≤10−6 0.31 5.48·10−6 ≤10−6 0.090 0.002 ≤10−6 0.073 6.88·10−5 ≤10−6 6 0.092 ≤10−6 ≤10−6 0.23 8.04·10−5 3.05·10−5 0.057 1.17·10−4 ≤10−6 0.55 0.0095 ≤10−6 7 0.64 0.002 3.12·10−5 0.78 0.26 0.21 0.18 0.022 3.29·10−5 0.055 0.0037 ≤10−6 8 0.011 7.32·10−5 ≤10−6 0.16 0.008 3.03·10−6 0.042 0.098 6.34·10−5 0.038 0.002 ≤10−6 9 0.049 0.17 0.002 0.27 0.41 0.028 0.09 0.010 4.29·10−4 0.013 0.051 6.81·10−5 10 0.12 0.27 0.044 0.29 0.89 0.20 0.53 0.016 3.52·10−5 0.34 0.046 2.25·10−4 11 0.018 6.88·10−6 ≤10−6 0.58 5.79·10−4 1.37·10−6 0.25 0.037 1.98·10−5 0.091 0.047 0.12 12 0.006 8.21·10−6 ≤10−6 0.94 0.004 6.94·10−5 0.26 0.18 1.34·10−4 0.65 0.059 0.064 13 0.10 0.092 0.002 0.57 0.085 0.002 0.040 0.092 2.69·10−4 0.021 0.0068 ≤10−6 14 0.79 0.068 5.38·10−5 0.54 0.017 0.001 0.055 0.003 ≤10−6 0.032 0.0082 ≤10−6 15 0.18 0.061 0.003 0.56 0.58 0.24 0.018 0.019 ≤10−6 0.76 0.019 2.16·10−5 16 0.46 0.045 ≤10−6 0.25 0.019 0.001 0.18 0.38 0.018 0.083 0.025 ≤10−6 17 0.87 0.86 0.22 0.73 0.88 0.82 0.14 0.17 0.27 0.81 0.17 3.76·10−4
Fig.7. p-valuebull’s-eyeplotsfromintra-segmentcomparisonsbetweenprimaryHCMandSLVHpatientsforϑdistributionsobtainedwithdifferentmethodologies,aswell astraditionalrotationβdistribution.Scaleisdefinedas−log10(p-value).
3.2. Classification analysis
496
Wehaveassessedthesurvivalrateofthefeatureselectionstage 497
of the classifier (recall Fig. 4). Results are shown in Table 6 for 498
thefeaturesdescribedinTable3;featuresobtainedfromboththe 499
MR-Celasticregistrationaswellasfromthespheroidaldeformable 500
modelhavealsobeenincluded.Additionally,wehavealsoincluded 501
conventional indices of cardiac motion used in clinical practice, 502
suchaswallthickening(WT)overmid-ventricularslices(seeDong
503
etal.,1994; Prasadetal.,2010 formoredetails),ejection fraction 504
(EF) and LV volume, with the latter both at ED (EDLVV) andES 505
phases(ESLVV). 506
The mostrepeated configuration of the classifier consisted of 507
FCM for stages 1 and 2.2 and SVMg for stage 2.1. The best ac-508
curacy figures were obtained when using diagonal strain ten-509
sor components on stage 1, whereas for stages 2.1 and 2.2, the 510
best feature vectorsturned out to be [E ll , TwistϑTAG , Twist
φ
] and511
[E ll ,E cc ,Twist
ϑ
TAG ,||
ω
||
],respectively.Ifwe takeinto accountnot 512onlythebestclassifierbutwealsorankperformanceandanalyze 513
the first, say,ten results,the composition of theselected feature 514
vectorsshowssome degreeofvariabilitywhichseemsvery much 515 inaccordancewiththeresultsinTable6. 516 In terms of end-to-end performance, the obtained accuracy 517 (86%)seemscomparableinclassificationfigures withotherproce- 518 dures(see Gopalakrishnan etal., 2014; Puyol-Antón et al., 2017) 519 although, in these cases, no SLVH are analyzed, so comparisons 520 havetobemadecautiously.Indisaggregatedterms,thesequential 521 classifierhasobtainedsensitivityfigureshigherthan70%foreach 522 group(specifically,81%forcontrol,72%forsecondaryhypertrophy 523 patientsand95%forprimary HCMpatients).Itisworthmention- 524 ingthatnoprimaryisclassifiedascontrolandviceversa;therefore, 525 the pipeline proposed seems a proper screening tool. Secondary 526 patientsperformanceisclearlylowerascomparedwithbothcon- 527 trolsandprimaryHCMpatients, possiblyduetoasmallersample 528 sizeaswellasthesubtledifferencestheyshow. 529 Finally, in order to assess the relative strength of the differ- 530 entmeasuresinclassification performance,wehaverun theclas- 531 sificationpipeline withdifferentfeaturessubsets. Inparticular, in 532
Table6
Survivingpercentrateofthefeaturesemployedintheclassificationprocedure(see notationinFig.4).Stage2.2isdevisedtoSLVH-to-HCMsensitivity,whilestage2.1 referstoSLVH-to-Controlsensitivity.
Features Stage2.2 Stage2.1 Stage1
Err 7 38 35
Ecc 54 24 60
Ell 49 50 37
Elc 22 11 6
||ω|| 43 25 19
TwistϑTAG 42 32 27
TwistϑCINE 7 2 13
TwistϑMODEL 15 8 7
TwistβTAG 19 16 16
TwistβCINE 8 5 4
TwistβMODEL 12 3 0
Twistφ 18 20 24
T 8 13 18
θlc 3 0 1
αLRl 7 9 10
ωzzerocross.TAG 21 13 4 ωzzerocross.CINE 2 5 2 ωzzerocross.MODEL 12 3 0 βzerocross.TAG 14 1 3 βzerocross.CINE 0 2 1 βzerocross.MODEL 3 1 0
WT 0 8 10
EF 0 6 3
EDLVV 0 0 1
ESLVV 0 2 0
clinicalindices) andwithMR-Tfeatures only. Fromthe latter,we 535
have also shown classification performance obtained discarding 536
traditionalandvorticalrotationfeatures,respectively. 537
4. Discussion
538
Therelationshipbetweenmyocardialfibrosisandlocal mechan-539
ics is important for the diagnosis and treatment of cardiomy-540
opathies(Karamitsos andNeubauer,2011). Thispapershowsthat 541
LVrotationisessentialforpropermyocardialfunction.Inourcase, 542
mostofthemeasurementsshowninTable4indicatethatLV rota-543
tioncanbe considered asa markerforcardiacdisease identifica-544
tionandmightbehelpfulforcardiomyopathyunderstanding,thus 545
providingcomplementary informationtostandard pumpfunction 546
indices. 547
The diagonal components of the strain tensor (E cc , E ll and 548
E rr ), defined in (3), have provided the highest separability be-549
tween pathologicandhealthy groups (cardiomyopathyscreening) 550
asshowninTable6;ourresultsareinaccordancewiththis find-551
ing(Saltijeraletal.,2010).Twistparameters seemtobealso valu-552
ablein thisstep, showinghigher survival ratethan shear strains 553
andtorsionparameters.Fortherefinementstepforcontrols/SLVH 554
(stage2.1inFig.4) the E cc componentinmid-ventricularareasis 555
the mostdiscriminative. Amongst the rotation-based parameters, 556
vorticitymodulus
||
ω
||
andtwistϑTAG remainthemostdiscrimina-557
tivefeatures. 558
In parallel, for the classifier stage 2.2, lower figures on the 559
globalperformanceareobtained.Besides,theselectedfeature vec-560
torpresentedonemorecomponentandtwocurl-derivedentries;it 561 consistedofacombinationoftwodiagonalstrain parameters,the 562 vorticitymodulus(9)andthetwistextractedfromthevorticalap- 563 proach(10).Extendingtheanalysistomore(thanone)high-ranked 564 features vectors, we observea greater degreeof heterogeneityas 565 well as the frequent presence of
ω
z (9). Consequently, the pro- 566 posedcurl-derivedparameters(9)–(11)haveturnedouttobepar- 567 ticularly useful for the discrimination of primary and secondary 568 casesasreflectedbysensitivityfiguresextractedfromTable7. 569 To the best of our knowledge, thisis the first study in HCM 570 patientsthatrelatesvorticityincardiacdeformationfieldswithlo- 571 cal myocardialmechanics andits abnormalities; our results sug- 572 gest that vorticity mayhelp deepen onthe underlying character- 573 isticsbehindprimary andsecondary casesofLVhypertrophy.For 574 these parameters, neither the length nor the centerof the heart 575 are needed, so no bias is introduced in their estimation; as we 576 havedescribedabove,vorticityisdirectly relatedto thedeforma- 577 tion gradient tensor and, consequently, it can be estimatedfrom 578 thesameinformationusedinthestraintensor(3)analysis.Inad- 579 dition, they show higher survival rates than techniques that use 580 fixedLVaxisandcenterrepresentations,givingrisetoamorereli- 581ableparameter. 582
The color-coded results shown in Fig. 6 reveal that patients 583 withboth formsof ventricular hypertrophy presentgreater rota- 584 tion distributionsascompared withcontrolsovermostsegments 585 both forvortical(10)andtraditional (4)rotations.As forprimary 586 HCMpatients, thereisaclearincreasedrotation(in modulus)for 587 allsegments,buthighvorticityareasaremainlylocatedonseptal 588 segments. SLVHpatientsshowed asomewhat differentpatternin 589 mid-ventricular andbasal regions ofthe heart, presentinghigher 590 valuesthan controls;those valuesare not focused on septalseg- 591 ments but a slight bias to lateral segments may exist. Other re- 592 gionalanalyses havealsobeenperformedby meansof automatic 593 LVsegmentation(Baietal.,2016;Liangetal., 2015).However,the 594 presence of hypertrophic tissue and other pathologies may bias 595 thefinal parcellationofthe cardiacsegments.Forthisreason, we 596 havemadeuseofthe17-segmentmodelasaconsistentandwell- 597 established model formotion analysis(Smiseth etal., 2016). The 598 usefulness of the vortical parameters has also been reflected by 599 theimprovementshowninTable7withrespecttotraditionalro- 600 tationparameters andtheminordegradation withrespectto the 601 full-feature optionwhencurl-derivedparameters are usediniso- 602
lation. 603
OurresultsalsoindicateahigherperformanceofMR-Tformo- 604 tion estimation withrespect toMR-C; however,it is well-known 605 that HARPprocedures havesome difficultiesin correctlyestimat- 606 ing the phase in the vicinity of boundaries. In those areas, elas- 607 ticregistration procedures over MR-Cis usually more robust.For 608 thisreason,acoordinatedprocedurethatweighsbothinformation 609 sources according to position may potentially provide better fig- 610
ures. 611
Additionally,vorticalmeasures werecomparedwhenextracted 612 bothfromtheHARPmethodandbydeformingaspheroidalmodel 613 previously fit.Similar vorticityvalueswere obtainedalthoughthe 614 extracted vortical patterns from the spheroidal model showed 615
Table7
Confusionmatricesforclassificationperformancewithdifferentfeaturesubsets.Matriceshavebeennormalizedwithrespecttothetotalnumberofpatients. Eachcolumnrepresentstheinstancesinapredictedclasswhilerowsrepresenttheinstancesinanactualclass.
FullFeatureSet MR-Taggingonly Vorticalonly Traditionalonly
C S H C S H C S H C S H
C 0.236 0.064 0 0.243 0.057 0 0.24 0.06 0 0.234 0.066 0 S 0.023 0.145 0.032 0.038 0.144 0.018 0.021 0.141 0.038 0.038 0.127 0.035 H 0 0.017 0.483 0 0.025 0.475 0 0.022 0.478 0 0.023 0.477
S.Sanz-Estébanezetal./MedicalImageAnalysisxxx(2018)xxx–xxx 11
JID:MEDIMA [m5G;March15,2018;18:55]
higher spatial smoothness dueto the regularized functions used 616
todefinethedeformation,therebyreducingitsusefulnessfor clas-617
sification(seeTable6). 618
Finally, conventional global indices in HCM diagnosis (see 619
Table 1) have also been tested in the classifier. Neither of them 620
presented a very representative survival rate (even in stage 1), 621
hence, their influence on final performance does not seem rele-622
vant. 623
5. Conclusions and future lines
624
In thispaperwe haverelatedanomalies onlocalvortical pat-625
terns with the presence of fibrotic tissue by means of an im-626
age processing pipeline and a two-stage sequential classification 627
method.Localrotationparametersareestimatedbymeansofa ro-628
bustmotionandtensoranalysissothat potential biasesofglobal 629
analysesareavoided. 630
Local rotation wassignificantlyincreased inprimary HCM pa-631
tients,speciallyintheseptum,comparedtocontrolsandsecondary 632
cases;inthelatter,vorticalabnormalitiesmayshowaslighttrend 633
to lateral segments and with values less pronounced than pri-634
maries. Thesefindings may provideimportantinformation in hy-635
pertrophic diseases to establish a differential diagnostic between 636
thesetwoclasses. 637
Classification figures, although collateral in the paper, are 638
promising;clearly,discrimination betweenprimary HCMand sec-639
ondarycasesismorechallengingthanbetweenHCMandcontrols. 640
Therefore,figures relatedtothe formerproblemhavebeenlower 641
thanthoserelatedtothelatter.Alargercohortmayletusincrease 642
this number in the near future. Classification of SLVH cases has 643
proven tobe achallengingtaskbutfigures,despite notbeing re-644
markable, are likely to improve when equalizing the number of 645
subjectsinthestudyorbyintroducingfeatures thattake into ac-646
countthepositionofvorticalpeaks. 647
Acknowledgments
648
This work was partially supported by the Spanish Ministerio 649
de Ciencia e Innovación under Research Grant TEC2013-44194-P, 650
theEuropeanRegionalDevelopmentFund(ERDF-FEDER)under Re-651
searchGrantTEC2014-57428-RandtheSpanishJuntadeCastillay 652
LeónunderGrantVA069U16. 653
References
654
Aelen,F.,Arts,T.,Sanders,D.,Thelissen,G.,Muijtjens,A.,Prinzen,F.,Reneman,R., 655
1997.Relationbetweentorsionandcross-Sectionalareachangeinthehuman 656
leftventricle.J.Biomech.30,207–212. 657
Axel,L.,Dougherty,L.,1989.MRimagingofmotionwithspatialmodulationof mag-658
netization.Radiology171(3),841–845. 659
Bai,W.,Peressutti,D.,Parisot,S.,Oktay,O.,Rajchl,M.,O’Regan,D.,Cook,S.,King,A., 660
Rueckert,D.,2016.BeyondtheAHA17-SegmentModel:Motion-Driven Parcella-661
tionoftheLeftVentricle.In:LectureNotesBioinform,9354.Springer,pp.13–20. 662
Bansala,M.,Kasliwalb,P.,2013.Howdoidoit?Speckle-trackingechocardiography. 663
IndianHeartJ.65(1),117–123. 664
Baron,B., 2008.The2006americanheartassociationclassification of cardiomy-665
opathiesisthegoldstandard.Circ.HeartFail1,72–76. 666
Bezdec, J., 1981.Pattern Recognition with Fuzzy Objective Function Algorithms. 667
PlenumPress,NewYork. 668
Buchalter,M.,Weiss,J.,Rogers,W.,Zerhouni,E.,Weisfeldt,M.,Beyar,R.,Shapiro,E., 669
1990.Noninvasivequantification ofleftventricularrotational deformationin 670
normalhumansusingmagneticresonanceimagingmyocardialtagging. Circu-671
lation81(4),1236–1244. 672
Cerqueira,M., 2002.Standardizedmyocardialsegmentationand nomenclaturefor 673
tomographicimagingoftheheart:astatementforhealthcareprofessionalsfrom 674
thecardiacimagingcommitteeofthecouncilonclinicalcardiologyofthe amer-675
icanheartassociation.Circulation105(4),539–542. 676
Cordero-Grande,L.,Merino-Caviedes,S.,Aja-Fernández,S.,Alberola-López,C.,2013. 677
Groupwiseelasticregistrationbyanewsparsity-promotingmetric:application 678
tothealignmentofcardiacmagneticresonanceperfusionimages.IEEETrans. 679
PatternAnal.Mach.Intell.35,2638–2650. 680
Cordero-Grande,L., Royuela-del-Val, J., Sanz-Estébanez, S.,Martín-Fernández,M., 681 Alberola-López,C.,2016.Multi-Orientedwindowedharmonicphasereconstruc- 682 tionforrobustcardiacstrainimaging.Med.ImageAnal.29,1–11. 683 Cordero-Grande,L.,Sevilla,T.,Revilla,A.,Martín-Fernández,M.,Alberola-López,C., 684 2013.Assessmentofthefibroticmyocardialtissuemechanicsbyimageprocess- 685 ing.IEEECinCConf.635–638. 686 Cordero-Grande,L.,Vegas-Sánchez-Ferrero,G.,Casaseca-de-la-Higuera,P.,Alberola- 687 López,C.,2011.ImprovingharmonicphaseimagingbythewindowedFourier 688 transform.In:8thIEEEInternationalSymposiumonBiomedicalImaging:From 689 NanotoMacro.Chicago,USA,pp.520–523. 690 Cortes,C.,Vapnik,V.,1995.Support-vectornetworks.Mach.Learn.20,273–297. 691 Dhillon,A.,Sweet,W.,Popovic,Z.,Smedira,N.,Thamilarasan,M.,Lytle,B.,Tan,C., 692 Starling,R.,Lever,H.,Moravec,C.,Desai,M.,2014.Associationofnoninvasively 693 measuredleftventricular mechanicswithinvitromuscle contractileperfor- 694 mance:aprospectivestudy inhypertrophic cardiomyopathypatients. J.Am. 695 HeartAssoc.3(6),e001269. 696 Dong,S.,MacGregor,J.,Crawley,A.,McVeigh,E.,Belenkie,I.,Smith,E.,Tyberg,J., 697 Beyar,R.,1994.Leftventricularwallthicknessandregionalsystolicfunctionin 698 patientswithhypertrophiccardiomyopathy.athree-dimensionaltaggedmag- 699 neticresonanceimagingstudy.Ciculation90(3),1200–1209. 700 Fung,Y.,1965.FoundationsofSolidMechanics.Prentice-Hall,EnglewoodCliffs,NJ. 701 Gopalakrishnan,V., Menon, P., Madan, S.,2014. cMRI-BED:a novel informatics 702 frameworkforcardiacMRIbiomarkerextractionanddiscoveryappliedtope- 703 diatriccardiomyopathyclassification.In:2ndInternationalWork-Conferenceon 704 BioinformaticsandBiomedicalEngineering.Granada,Spain.14(Suppl2):S7. 705 Heermann,P.,Hedderich,D.,Paul,M.,Schulke,C.,Kroeger,J.,Baessler,B.,Wichter,T., 706 Maintz,D.,Waltenberger,J.,Heindel,W.,Bunck,A.,2014.Biventricularmyocar- 707 dialstrainanalysisinpatientswitharrhythmogenicrightventricularcardiomy- 708 opathy(ARVC)usingcardiovascularmagneticresonancefeaturetracking.J.Car- 709 diovasc.Magn.Reson.16(1),75–87. 710 Helle-Valle, T., Crosby, P., Edvardsen, T., Lyseggen, E., Amundsen, B., Smith, H., 711 Rosen, B., Lima,J., Torp, H., Ihlen, H.,Smiseth, O., 2005. New noninvasive 712 methodforassessmentofleftventricularrotation:speckletrackingechocardio- 713 graphy.Circulation112,3149–3158. 714 Ibrahim,E.,2011.Myocardialtaggingbycardiovascular magneticresonance:evo- 715 lutionoftechniquespulsesequences,analysis,algorithmsandapplications.J. 716 Cardiovasc.Magn.Reson.13,36. 717 Jeung,M.,Germain, P.,Croisille,P.,El ghannudi,S.,Roy,C., Gangi,A.,2012.My- 718 ocardialtaggingwithMRimaging:overviewofnormalandpathologicfindings. 719 RadioGraphics32,1381–1398. 720 Karamitsos,T.,Neubauer,S.,2011.Theinterplaybetweencardiacstrainandfibro- 721 sisinnon-Ischaemiccardiomyopathies:insightsfromcardiovascularmagnetic 722 resonance.Eur.J.HeartFail13,927–928. 723 Köhler,B.,Gasteiger, R.,Preim, U.,Theisel, S.,Maintz, D.,Preim, B.,2013. Semi- 724 automaticvortexextractionin4DPC-MRIcardiac bloodflow datausingline 725 predicates.IEEETrans.Vis.Comp.Graph.19(12),2773–2782. 726 Liang,X.,Garnavi,R.,Wail,S.,Liang,S.,Prassanna,P.,2015.Automaticsegmentation 727 oftheleftventricleinto17anatomicalregionsincardiacMRimaging.In:37th 728 ConfProcIEEEEngMedBiolSoc.Milan,Italy,pp.6531–6535. 729 Lorenz,C.,Pastorek,S.,Bundy,J.,2000.Delineationofnormalhumanleftventricular 730 twistthroughoutsystolebytaggedcinemagneticresonanceimaging.J.Cardio- 731 vasc.Magn.Reson.2(2),97–108. 732 Makram,A.,Khalifa,A.,El-Rewaidy, H.,Fahmy,A.,Ibrahim, E.,2015.Assessment 733 ofglobalcardiac functionfromtaggedmagneticresonanceimages.compari- 734 sonwithcineMRI.In:23rdProcIntlSocMagResonMed,Toronto,Canada,23, 735
p.4472. 736