M A J O R A R T I C L E
Clinical and Molecular Epidemiology of
Extended-Spectrum
b
-Lactamase–Producing
Escherichia coli
as a Cause of Nosocomial Infection or Colonization:
Implications for Control
Jesu´s Rodrı´guez-Ban˜o,1,3Maria D. Navarro,1Luisa Romero,2Miguel A. Muniain,1,3Evelio J. Perea,2,4
Ramo´n Pe´rez-Cano,1,3Jose R. Herna´ndez,4and Alvaro Pascual2,4
1Seccio´n de Enfermedades Infecciosas, Servicio de Medicina Interna, and2Servicio de Microbiologı´a, Hospital Universitario Virgen Macarena,
and3Departamento de Medicina and4Departamento de Microbiologı´a, Universidad de Sevilla, Seville, Spain
Background. Extended-spectrum b-lactamase (ESBL)–producing members of the Enterobacteriaceae family are important nosocomial pathogens.Escherichia coliproducing a specific family of ESBL (the CTX-M enzymes) are emerging worldwide. The epidemiology of these organisms as causes of nosocomial infection is poorly un-derstood. The aims of this study were to investigate the clinical and molecular epidemiology of nosocomial infection or colonization due to ESBL-producingE. coliin hospitalized patients, consider the specific types of ESBLs produced, and identify the risk factors for infection and colonization with these organisms.
Methods. All patients with nosocomial colonization and/or infection due to ESBL-producingE. coliin 2 centers (a tertiary care hospital and a geriatric care center) identified between January 2001 and May 2002 were included. A double case-control study was performed. The clonal relatedness of the isolates was studied by repetitive extragenic palindromic–polymerase chain reaction and pulsed-field gel electrophoresis. ESBLs were characterized by isoelectric focusing, polymerase chain reaction, and sequencing.
Results. Forty-seven case patients were included. CTX-M–producingE. coliwere clonally unrelated and more frequently susceptible to nonoxyimino–b-lactams. Alternately, isolates producing SHV- and TEM-type ESBL were epidemic and multidrug resistant. Urinary catheterization was a risk factor for both CTX-M–producing and SHV-TEM–producing isolates. Previous oxyimino–b-lactam use, diabetes, and ultimately fatal or nonfatal underlying diseases were independent risk factors for infection or colonization with CTX-M–producing isolates, whereas previous fluoroquinolone use was associated with infection or colonization with SHV-TEM–producing isolates.
Conclusions. The epidemiology of ESBL-producing E. coli as a cause of nosocomial infection is complex. Sporadic CTX-M–producing isolates coexisted with epidemic multidrug-resistant SHV-TEM–producing isolates. These data should be taken into account for the design of control measures.
Extended-spectrumb-lactamases (ESBLs) are plasmid-encodedb-lactamases that confer significant resistance to penicillins, narrow- and extended-spectrum cepha-losporins, and aztreonam. Organisms harboring ESBLs are also frequently resistant to aminoglycosides, tri-methoprim-sulfamethoxazole, and quinolones. ESBL-producing members of the Enterobacteriaceae family
Received 28 June 2005; accepted 23 August 2005; electronically published 29 November 2005.
Reprints or correspondence: Dr. Jesu´s Rodrı´guez-Ban˜o, Seccio´n de Enfermedades Infecciosas, Hospital Universitario Virgen Macarena, Avda Dr Fedriani 3, 41071 Seville, Spain ([email protected]).
Clinical Infectious Diseases 2006; 42:37–45
2005 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2006/4201-0006$15.00
have played a leading role among nosocomially ac-quired multidrug-resistant organisms during the past decade [1, 2]. Many outbreaks of infection caused by ESBL-producing Klebsiella pneumoniae have been re-ported all over the world [1, 2]. The risk factors for infection caused by this organism are similar to those described for other nosocomial multidrug-resistant pathogens [3].
ESBLs have been classified into different types. Ini-tially, the 2 most frequent types of ESBL were TEM types and SHV types. More recently, enzymes belonging to a different type of ESBL, such as the CTX-M type (so called because they are mainly cefotaximases), are being detected with increasing frequency, particularly in ESBL-producingEscherichia coli,which now
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
sents an emerging cause of infection in many areas of the world [4–10]. Some data suggest that the epidemiology of these emerging ESBL-producingE. coliis substantially different from that of ESBL-producingK. pneumoniae[4, 5, 9, 11]. The aims of this study were to investigate the clinical and molecular epidemiology of nosocomial infection due to ESBL-producing
E. coli in hospitalized patients, consider the specific types of ESBLs produced, and identify the risk factors for infection and colonization with these organisms.
METHODS
Study Site, Subjects, and Design
The study was performed in the 2 hospitals of the administra-tive Health Area of North Seville, Spain (the Hospital Univ-ersitario Virgen Macarena, a 950-bed teaching hospital, and the Hospital San La´zaro, a 150-bed hospital that mainly provides care for elderly patients). Intensive care is only provided in the acute care hospital. Transfer of patients between the 2 hospitals is frequent.
During the study period (January 2001–May 2002, inclusive), all patients from whom ESBL-producingE. colihad been iso-lated from any clinical sample were identified through daily review of microbiologic reports and were prospectively inves-tigated. Patients were included as cases if their samples were obtained after 48 h of hospitalization and provided that, at the time of admission to the hospital, there had been no signs or symptoms of infection potentially attributable to ESBL-pro-ducing E. coli. Patients colonized by ESBL-producing E. coli
detected only by means of surveillance samples were excluded. Case patients were included only once.
Two control groups were studied. Patients in control group 1 were randomly selected among patients who were admitted to the same hospital unit during the same quarter and had a hospital stay previous to the isolation of ESBL-producing E. colithat was at least as long as that of the corresponding case patient. Patients in control group 2 were randomly selected among patients admitted to the same type of hospital service unit (medical or surgical unit or intensive care unit) during the same quarter and from whom a non–ESBL-producing iso-late of E. coli had been recovered from any clinical sample. Control group 1 included 2 controls per case patient and con-trol group 2 included 2 concon-trols per case patient, except for 9 case patients for whom only 1 control was found.
Definitions and Variables
The type of infection was defined in accordance with Centers for Disease Control and Prevention (CDC) criteria [12]. Pa-tients who did not meet criteria for infection were considered to be colonized. The following data were collected: age; sex; underlying diseases; severity of the underlying diseases, ac-cording to the McCabe classification [13]; previous
hospitali-zations; residence in a nursing home; receipt of long-term he-modialysis; receipt of antimicrobial agents; invasive procedures; and hospitalization in an intensive care unit. The time at risk was defined as the time from admission to the hospital until the date on which E. coli was isolated for case patients and control group 2, and as the time from admission until the date of discharge or death for patients in control group 1.
Antimicrobial therapy was considered to be appropriate if at least 1 antimicrobial with in vitro activity against the isolated microorganism had been administered at the usual dose for at least 24 h. All case patients were observed until hospital dis-charge or death. The study protocol was approved by the local ethics committee.
Microbiological Studies
Bacterial isolates and susceptibility assays. The first isolate from each patient was studied. Identification was determined using the Vitek 2 system (bioMe´rieux) and API 20E strips (bioMe´rieux). ESBL production was screened and confirmed in accordance with guidelines of the NCCLS [14, 15]. The in vitro activity of antimicrobial agents was determined using a microdilution assay, in accordance with NCCLS guidelines [15].
Molecular typing. Clonal relationships between the isolates were determined by repetitive extragenic palindromic (REP)– PCR, as described elsewhere [16]. Isolates were considered to be clonally related when band patterns differed by!3 bands.
Isolates determined by REP–PCR to be clonally related were also studied by PFGE, as described elsewhere [17], usingXbaI endonuclease (Roche Applied Sciences). Interpretation of the clonal relatedness of PFGE patterns was performed as described by Tenover et al. [18].
b-Lactamase characterization. Isoelectric focusing [19, 20] and PCR were used for the preliminary characterization of
b-lactamases andb-lactamase genes, respectively. The isoelec-tric focusing ranges were correlated to TEM-, SHV-, or CTX-M–typeb-lactamases [21]. The presence ofblaTEM,blaSHV, and
blaCTX-M in each organism was studied by PCR, as described
elsewhere [22, 23]. Oligonucleotide primers designed to amplify the genes encoding the most common subgroups within the ESBL families were used [23–25].E. coliJ53 Rif-R was used as a negative control.
Amplicons were sequenced at an external center (DNA Au-tomatic Sequencing Service, Consejo Superior de Investiga-ciones Cientifı´cas, Madrid, Spain) equipped with an ABI Prism 377 sequencer (Applied Biosystems). Sequences were analyzed using the Chromas application, the Basic Local Alignment Search Tool [26], and the Traduction Multiple program [27].
Statistical Analysis
Continuous variables were compared using the Mann-Whitney
Utest. Qualitative variables were compared using the x2test
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
Table 1. Characteristics of hospitalized patients colonized or infected with extended-spectrumb-lactamase–producing Esch-erichia coli.
Characteristic
Acute care hospital (np29)
Geriatric care hospital (np18) P
Male sex 16 (55) 9 (50) .7
Age, median years (range) 70 (32–82) 81 (56–90) .002 Hospital ward
Medical service 14 (48) 18 (100) .001
Surgical service 9 (31) … …
Intensive care unit 6 (21) … …
Rapidly fatal underlying disease 5 (17) 5 (28) .4
Diabetes mellitus 13 (45) 7 (39) .6
Chronic pulmonary disease 6 (21) 2 (11) .6
Malignancy 7 (24) 3 (17) .7
Venous catheter 27 (93) 16 (89) .6
Urinary catheter 20 (69) 13 (72) 1
Surgery 8 (28) 0 .01
History of antimicrobial use 28 (97) 16 (89) .5
NOTE. Data are no. (%) of case patients, unless otherwise indicated.
Figure 1. Distribution of the 47 infecting or colonizing extended-spectrumb-lactamase–producingEscherichia coliisolates in hospitalized patients during the study period, according to genotype.
or the Fisher’s exact test, as appropriate; ORs and 95% CIs were calculated. Multivariate logistic regression analysis was performed to determine variables that were independently as-sociated with the risk of colonization or infection with ESBL-producingE. coli. Potential interactions between variables were considered. Variables were selected in a backward stepwise pro-cess. Data were analyzed using the SPSS statistical software package (SPSS).
RESULTS
During the study period, ESBL-producingE. coliwas isolated from 96 patients; 47 patients met the inclusion criteria and were included in this study. The other 49 patients were non-hospitalized and have been analyzed elsewhere [5]. During the
study period, 4.1% of allE. coliisolated from hospitalized pa-tients were ESBL producers, and only 15 ESBL-producing En-terobacteriaceae isolates were isolated from hospitalized patients.
Twenty-nine case patients (62%) were in the acute care hos-pital, and 18 (38%) were in the geriatric care hospital. The rate of colonization or infection was significantly higher in the ge-riatric care hospital (0.6 cases per 1000 patient-days vs. 0.06 cases per 1000 patient-days;P!.001).
The characteristics of the case patients are shown in table 1; 32% of cases occurred during the first week of hospitalization. Thirty-six patients (77%) were considered to be infected. The types of infection included the following: 15 urinary tract in-fections (42%), 13 soft-tissue inin-fections (36%; 4 pressure ulcers and 5 surgical site infections), 4 respiratory tract infections (11%), 3 cases of primary bacteremia (8%), and 1 intra-ab-dominal infection (3%). Three patients had secondary bacter-emia. Overall, 6 patients (16%) were bacteremic. Only 13 pa-tients (36%) received appropriate empirical antimicrobial therapy. Fourteen patients died (crude mortality rate, 30%). Five patients died of infection (infection-related mortality rate, 14%).
With respect to the type of ESBL, 29 isolates (62%) produced an SHV type (28 were identified by sequencing as SHV-12, and 1 was identified as SHV-2a), 27 (57%) produced a CTX-M type (26 were CTX-M-14, and 1 was CTX-M-9), and 18 (38%) produced an as yet unidentified ESBL with an isoelectric point of 6.5, which is probably a TEM type, according to the results of other experiments (data not shown), here referred to as “TEM-Q” for easier understanding of data. Twenty-four isolates (51%) produced11 ESBL, the most frequent combination
be-ing SHV-12 plus TEM-Q (14 isolates). Of the 23 isolates that produced only 1 ESBL, 16 produced CTX-M-14. Isolates pro-ducing TEM-Q clustered from January through July 2001 (14
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
Figure 2. Duration of hospital stay for 22 patients colonized or infected with extended-spectrumb-lactamase–producingEscherichia coliisolates belonging to clonally-related groups A(grey bars)and B(white bars). Theblack pointrepresents the date when the microorganism was isolated, and theasteriskindicates stay in the geriatric care hospital.
isolates) and from December 2001 through March 2002 (4 isolates).
Twenty-five different genotypes were identified by REP-PCR, including those of 4 clonally related groups (“epidemic iso-lates”; 55%) and those of 21 clonally unrelated isolates (“spo-radic isolates”; 45%). Isolates considered to be clonally related by REP-PCR were also studied by PFGE, with identical results. The distribution of cases throughout the study period according to genotypes is shown in figure 1. Clonal group A comprised 11 isolates; all of them produced SHV-12, 9 isolates also pro-duced TEM-Q, and 5 isolates also propro-duced CTX-M-14. Four of these patients were in the geriatric care hospital, and 7 were in the acute care hospital (3 patients were in the intensive care unit, 3 were in an internal medicine ward, and 1 was in a surgical ward). Clonal group B also consisted of 11 isolates: 9 produced SHV-12, 8 produced TEM-Q, 1 produced CTX-M-14, and 1 produced CTX-M-9. Eight patients were in the ge-riatric care hospital, and 3 were in the acute care hospital (2 patients were in the intensive care unit, and 1 patient was in a general surgery ward). Among the 6 patients in the intensive care unit included in the study, 5 had an epidemic isolate. The duration of hospitalization of patients colonized or infected with these 2 clonal groups is represented in figure 2. The other 2 clonal groups were constituted by 2 isolates each. Among the
21 sporadic isolates, 17 produced a CTX-M enzyme. Compared with nonepidemic isolates, epidemic isolates were more fre-quently producers of TEM- and SHV-type ESBLs (62% vs. 10% [P!.001] and 85% vs. 33% [P!.001], respectively) and less frequently producers of CTX-M types (39% vs. 81%; Pp
). Susceptibility data for the isolates are shown in table 2. .003
To investigate the epidemiology of the different types of ESBLs, 2 homogeneous groups were compared: 16 patients with isolates producing only CTX-M-14 (the “CTX-M group”) and 14 patients with isolates producing both SHV-12 and TEM-Q but not CTX-M-14 (the “SHV-TEM group”). All isolates but 1 from the CTX-M group were sporadic, whereas all isolates from the SHV-TEM group belonged to epidemic clones. Pa-tients with isolates from the CTX-M group were admitted more frequently to surgical units (37.5% vs. 0%,Pp.01), less fre-quently to the geriatric care hospital (25% vs. 78.5%; Pp
), and had diabetes more often (56.3% vs. 21.4%;
.009 Pp
), than did patients with isolates from the SHV-TEM group; .05
previous use of fluoroquinolones was less frequent among pa-tients in the CTX-M group (25% vs. 64.3%;Pp.03), whereas previous use of cefotaxime was somehow more frequent, a difference that was not statistically significant (37.5% vs. 21.4%; ). The median duration of previous hospital stay was
Pp.4
shorter among patients in the CTX-M group (14 days vs. 21
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
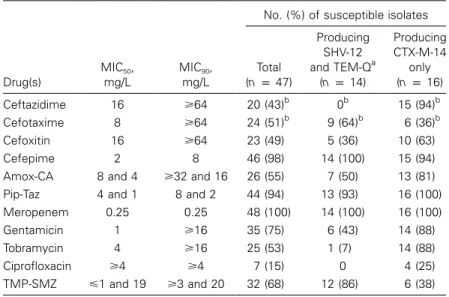
Table 2. Susceptibility data of extended-spectrum b-lactamase–producing Escherichia coliisolated from hospitalized patients.
Drug(s)
MIC50,
mg/L
MIC90,
mg/L
No. (%) of susceptible isolates
Total (np47)
Producing SHV-12 and TEM-Qa
(np14)
Producing CTX-M-14
only (np16)
Ceftazidime 16 ⭓64 20 (43)b 0b 15 (94)b
Cefotaxime 8 ⭓64 24 (51)b 9 (64)b 6 (36)b
Cefoxitin 16 ⭓64 23 (49) 5 (36) 10 (63)
Cefepime 2 8 46 (98) 14 (100) 15 (94)
Amox-CA 8 and 4 ⭓32 and 16 26 (55) 7 (50) 13 (81)
Pip-Taz 4 and 1 8 and 2 44 (94) 13 (93) 16 (100)
Meropenem 0.25 0.25 48 (100) 14 (100) 16 (100)
Gentamicin 1 ⭓16 35 (75) 6 (43) 14 (88)
Tobramycin 4 ⭓16 25 (53) 1 (7) 14 (88)
Ciprofloxacin ⭓4 ⭓4 7 (15) 0 4 (25)
TMP-SMZ ⭐1 and 19 ⭓3 and 20 32 (68) 12 (86) 6 (38)
NOTE. Amox-CA, amoxicillin–clavulanic acid; Pip-Taz, piperacillin-tazobactam; TMP-SMZ, tri-methoprim-sulfamethoxazole.
a
Undetermined TEM-type ESBL with an isoelectric point of 6.5.
b
Isolates with an MIC of⭐8 mg/L.
days), but the difference was not statistically significant, because of the wide ranges (3 to199 days in both groups). Isolates in
the CTX-M group were more frequently susceptible to amox-icillin-clavulanic acid (81.3% vs. 50%;Pp.07), ciprofloxacin (25% vs. 0;Pp.04), gentamicin (87.5% vs. 42.9%;Pp.01), and tobramycin (87.5% vs. 7.1%;P!.001) than were isolates in the SHV-TEM group.
Results of univariate analysis of risk factors for colonization or infection due to ESBL-producing E. coliis shown in table 3. Multivariate analysis was performed for all case patients, for those with isolates in the CTX-M group, and for those with isolates in the SHV-TEM group (table 4).
DISCUSSION
ESBL-producing members of the Enterobacteriaceae family have been important causes of nosocomial infections for the past 2 decades [1, 2]. Most attention has been focused onK. pneumoniae, because traditionally it has been the most fre-quently encountered nosocomial organism that produces ESBL. Specific information about the clinical epidemiology and rel-evance of nosocomial infection with ESBL-producingE. coliis scarce, because these organisms have usually been investigated together with other ESBL-producing Enterobacteriaceae isolates [28–32] or in studies limited to investigation of their micro-biological aspects [33, 34].
The emergence of infections caused by ESBL-producingE. coli(and, particularly, isolates producing CTX-M–type ESBL) has been recently reported throughout the world [4–10]; in our region, the first CTX-M–producingE. coliwere detected in 1999
[35]. Some data suggest that the epidemiologic characteristics of these emerging ESBL-producing E. coliare different from those of ESBL-producing K. pneumoniae: the proportion of patients with community-acquired infections due toE. coliis much higher [5, 9, 11], whereas clonally related outbreaks are far less frequent. Our data confirm that, beyond its importance as a pathogen in nonhospitalized patients [5, 9], ESBL-pro-ducingE. coliis also an emerging cause of nosocomial infec-tions. Our findings also show that the epidemiologic charac-teristics of these organisms are complex and somehow different, depending on the type of ESBLs produced.
In acute care hospitals, most previously reported nosocomial infections caused by ESBL-producingE. coli were caused by clonally unrelated isolates. However, some small clonal out-breaks have been described [6, 29, 31, 33, 34, 36–38]. Sur-prisingly, 45% of the cases in our study were caused by clonally related isolates, which predominantly produced both SHV-12 and an as yet undetermined TEM-type ESBL. An epidemiologic relationship was found for many of these case patients, sup-porting the horizontal transmission of the organism. The lapses of time without cases may be indicative of an unnoticed res-ervoir, colonized patients being the most probable. Interinsti-tutional spread was probably caused by the transfer of patients between the hospitals.
The 2 major clonal outbreaks of nosocomial infection seem to have been self-limited. Contact precautions for patients col-onized with ESBL-producing E. coli were not established be-cause transmission of these isolates had not been previously noticed in our hospitals. Our study was performed in the
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
Table 3. Univariate analysis of risk factors for colonization or infection with extended-spectrumb-lactamase–producingEscherichia coliin hospitalized patients.
Factor
Case patients (np47)
Control group 1 (np94)
Control group 2 (np85)
Value OR (95% CI) P Value OR (95% CI) P
Age, years 68.616 62.622 … .1 67.219 … .6
Male sex 53.2 54.1 0.9 (045–1.9) .9 41.2 1.6 (0.7–3.3) .1
Underlying disease Any
Nonfatal 42.6 24.5 225 (1.0–4.8) .02 35.3 1.2 (0.5–2.5) .5
Ultimately fatal 36.2 52.1 0.5 (0.2–1.0) .07 30.6 1.4 (0.6–2.9) .3
Rapidly fatal 21.3 23.4 0.8 (0.3–2.0) .7 34.1 0.5 (0.2–1.1) .1
Diabetes mellitus 42.6 30.9 1.6 (0.8–3.4) .1 42.9 0.9 (0.4–2.0) .9
Pulmonary disease 17.0 17 1.0 (0.3–2.5) 1.0 16.7 1.0 (0.3–2.6) .9
Renal disease 12.8 3.2 4.4 (1.0–18.6) .06 10.7 1.2 (0.4–3.6) .7
Recurrent urinary tract infection 17 4.3 4.6 (1.3–16.2) .02 13.1 1.3 (0.5–3.6) .5
Malignancy 21.3 22.3 0.9 (0.4–2.1) .8 19 1.1 (0.4–2.7) .7
Duration of previous hospitalization, days 27.827 29.423 … .7 20.619 … .08
Intensive care unit stay (present or past) 21.3 14.9 1.5 (0.6–3.7) .3 9.5 2.5 (0.9–7.0) .06 Catheter use
Venous 91.5 69.1 4.7 (1.5–14.6) .003 81.2 2.4 (0.7–7.9) .1
Urinary 70.2 25.5 6.8 (3.1–14.9) !.001 41.2 3.3 (1.5–7.1) .01
Mechanical ventilation 10.6 1.1 11.1 (1.2–97.7) .01 7.1 1.5 (0.4–5.4) .6
Surgery 17.0 10.6 1.7 (0.6–4.7) .2 17.6 0.9 (0.3–2.4) .9
Antimicrobial history
Any 93.6 25.5 42.7 (12.1–150.5) !.001 50.6 14.3 (4.1–49.7) !.001
Amoxicillin–clavulanic acid 23.4 8.5 3.2 (1.2–8.8) .01 14.1 1.8 (0.7–4.6) .1
Piperacillin-tazobactam 8.5 1.1 8.6 (0.9–79.7) .04 0 … .01
Oxyimino–b-lactamsa 40.4b 10.6 5.7 (2.3–13.7) !.001 9.4 7.1 (2.8–18.0) !.001
Carbapenems 2.1 1.1 2.0 (0.1–33.0) 1.0 3.5 0.5 (0.0–5.8) 1
Fluoroquinolones 40.4 8.5 7.2 (2.8–18.4) !.001 5.9 10.8 (3.7–31.8) !.001
Aminoglycosides 8.5 2.1 4.2 (0.7–24.2) .09 3.5 2.5 (0.5–11.8) .2
NOTE. Data are % of patients or meanvalueSD, unless otherwise indicated.
a
Cefuroxime, cefotaxime, ceftriaxone, cefepime, and aztreonam.
b
In 68% of instances, the oxyimino–b-lactam was cefotaxime.
text of a very low incidence of nosocomial infection with other ESBL-producing organisms [35]; a very active nosocomial in-fection–control program, particularly for multiresistant bacteria [39], has been in place at our hospitals since 1997, and use of alcoholic hand rubs have been available in all rooms since 2000. Thus, these measures might have had some impact on the unfolding of the outbreaks.
Several data suggest that the epidemiologic characteristics of CTX-M–producing isolates are different from those of isolates producing SHV-TEM enzymes, something that had not been previously noticed. All isolates in the SHV-TEM group be-longed to the main epidemic clonal groups, whereas CTX-M isolates were clonally unrelated. Five of the 6 case-patients in the intensive care unit were infected with isolates from the SHV-TEM group; most of the nosocomial outbreaks of ESBL-pro-ducingK. pneumoniaehave been caused by TEM-producing or SHV-producing isolates and predominantly occur in high-risk
areas, such as intensive care units [2]. In addition, in our area, the proportion of cases caused by TEM- or SHV-producing isolates among hospitalized patients (38% and 62%, respec-tively) was much higher than that among nonhospitalized pa-tients during the same period (18% and 18%) [5]. Isolates from the SHV-TEM group were more resistant to antimicrobials (al-though this should be interpreted with caution because these isolates are clonally related). Finally, nonfatal underlying con-ditions were associated only with CTX-M-14–producing iso-lates. All these data are indicative of the fact that, although ESBL-producingE. colifrom the SHV-TEM group behaved as typical epidemic nosocomial pathogens [3], those from the CTX-M group did not. We hypothesize that many of the pa-tients with CTX-M-14–producing isolates had acquired the or-ganism in the community. This is supported by the fact that many CTX-M cases occurred early during hospitalization and that, in our area, most of the ESBL-producingE. coliin
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
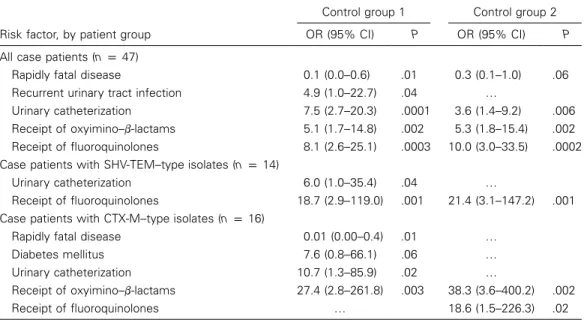
Table 4. Multivariate model of risk factors for colonizationor infection due to extended-spectrum b -lactamase–producingEscherichia coli in hospitalized patients.
Risk factor, by patient group
Control group 1 Control group 2
OR (95% CI) P OR (95% CI) P
All case patients (np47)
Rapidly fatal disease 0.1 (0.0–0.6) .01 0.3 (0.1–1.0) .06
Recurrent urinary tract infection 4.9 (1.0–22.7) .04 …
Urinary catheterization 7.5 (2.7–20.3) .0001 3.6 (1.4–9.2) .006
Receipt of oxyimino–b-lactams 5.1 (1.7–14.8) .002 5.3 (1.8–15.4) .002 Receipt of fluoroquinolones 8.1 (2.6–25.1) .0003 10.0 (3.0–33.5) .0002 Case patients with SHV-TEM–type isolates (np14)
Urinary catheterization 6.0 (1.0–35.4) .04 …
Receipt of fluoroquinolones 18.7 (2.9–119.0) .001 21.4 (3.1–147.2) .001 Case patients with CTX-M–type isolates (np16)
Rapidly fatal disease 0.01 (0.00–0.4) .01 …
Diabetes mellitus 7.6 (0.8–66.1) .06 …
Urinary catheterization 10.7 (1.3–85.9) .02 …
Receipt of oxyimino–b-lactams 27.4 (2.8–261.8) .003 38.3 (3.6–400.2) .002
Receipt of fluoroquinolones … 18.6 (1.5–226.3) .02
NOTE. Duration of previous hospital stay was included in all models.
hospitalized patients are clonally unrelated and produce an ESBL from the 9 group (a group comprising CTX-M-14, among others ESBLs) [5]; in fact, we have recently used sequencing techniques to characterized them as CTX-M-14 iso-lates (Velasco C, Romer L, Rodriguez-Ban´o J, et al., unpublished data).
The information provided by the double case-control study is complementary; comparison with control group 2 overes-timated the risk associated with previous antimicrobial use [40], but avoided common risk factors for infection caused by E. coli found in the analysis performed with control group 1. Urinary catheterization and previous administration of oxyi-mino–b-lactams or fluoroquinolones were independent risk factors for infection with ESBL-producingE. coli. The results of the multivariate models for specific types of ESBLs provide additional data that suggest differences in the epidemiologic characteristics of epidemic SHV-TEM and sporadic CTX-M isolates. Oxyimino–b-lactams, of which cefotaxime was the most frequently used, were related to CTX-M–producing iso-lates, traducing the cefotaximase activity of these enzymes, whereas fluoroquinolones use was associated with the cipro-floxacin-resistant SHV-TEM–producing isolates.
Our results provided further evidence of the importance of combining clinical and molecular epidemiologic data in the investigation of resistant pathogens and may have implications for the design of control programs for these organisms [41, 42]. Contact precautions, active surveillance in high-risk areas, and decrease of oxyimino–b-lactam consumption, as recom-mended by Paterson and Yu [1], should be performed when epidemic TEM-SHV–producingE. coliare detected; reduction
in fluoroquinolone use should also be considered. Some phe-notypic features of these isolates (e.g., a ceftazidime MIC greater than the cefotaxime MIC and resistance to other antimicro-bials) might be used as a preliminary epidemiologic marker, although some types of CTX-M ESBLs have been described to efficiently hydrolyze ceftazidime [43]. Alternately, sporadic CTX-M-producingE. colirepresent a new challenge for infec-tion control, because some small clonal nosocomial outbreaks have been described and because the spread of genetic elements carrying theblaCTX-Mgenes is a threat. If most of these cases
are imported from the community, the implementation of con-tact precautions for the cases detected by analysis of clinical samples might be useless, because many other colonized pa-tients will remain undetected. Active surveillance of coloniza-tion involving all patients admitted to the hospital is imprac-tical; targeted surveillance involving high-risk patients could be an option, but risk factors for colonization at admission have not been investigated. Also, more studies focused on the epi-demiologic behavior of these organisms and the mobile genetic elements harboring the CTX-M enzymes within hospitals are needed. Thus, the control measures that should be imple-mented for these organisms remain unclear. Meanwhile, strict application of hand hygiene, adequate use of gloves, and ju-dicious use of oxyimino–b-lactams (particularly cefotaxime) are mandatory, and because molecular epidemiologic analyses or techniques for ESBL characterization are not widely avail-able, continuous surveillance based on clinical epidemiology data and susceptibility patterns of the isolates is necessary to promptly recognize possible outbreaks.
Our study has some limitations. We did not perform active
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
surveillance to detect colonized patients. This approach is de-sirable, but it proved to be impractical in our situation, because the case patients were from many different wards. Also, trans-mission of plasmids containing the ESBLs between isolates should also be studied. Characterization of the plasmids con-taining the ESBLs is in progress.
In conclusion, our data indicate that the epidemiology of nosocomial infection with ESBL-producingE. coliin hospital-ized patients is complex; outbreaks of infection caused by iso-lates producing TEM and SHV types of ESBL similar to those caused by ESBL-producingK. pneumoniaeand clonally unre-lated isolates producing CTX-M enzymes may coexist. These data should be considered for control purposes. Also, ESBL-producingE. colishould be considered in the etiology of nos-ocomial infections in patients with risk factors.
Acknowledgments
Financial support. REIPI (Spanish Network for Research in Infectious Diseases), Instituto de Salud Carlos III, Ministerio de Salud y Consumo (C03/ 14); and Asociacio´n Sanitaria Virgen Macarena (fellowship to M.D.N.).
Potential conflicts of interest. All authors: no conflicts.
References
1. Paterson DL, Yu VL. Extended-spectrumb-lactamases: a call for im-proved detection and control. Clin Infect Dis1999; 29:1419–22. 2. Bradford PA. Extended-spectrum b-lactamases in the 21st century:
characterization, epidemiology, and detection of this important resis-tance threat. Clin Microbiol Rev2001; 14:933–51.
3. Safdar N, Maki DG. The commonality of risk factors for nosocomial colonization and infection with antimicrobial-resistantStaphylococcus aureus, Enterococcus, gram-negative bacilli,Clostridium difficile, and
Candida. Ann Intern Med2002; 136:834–44.
4. Bou G, Cartelle M, Tomas M, et al. Identification and broad dissem-ination of the CTX-M-14 b-lactamase in different Escherichia coli
strains in the northwest area of Spain. J Clin Microbiol2002; 40:4030–6. 5. Rodrı´guez-Ban˜o J, Navarro MD, Romero L, et al. Epidemiology and clinical features of extended-spectrumb-lactamase–producing Esche-richia coli in non-hospitalized patients. J Clin Microbiol 2004; 42: 1089–94.
6. Eckert C, Gautier V, Saladin-Allard M, et al. Dissemination of CTX-M-typeb-lactamases among clinical isolates of Enterobacteriaceae in Paris, France. Antimicrob Agents Chemother2004; 48:1249–55. 7. Ma L, Ishii Y, Chang FY, Yamaguchi K, Ho M, Siu LK. CTX-M-14, a
plasmid-mediated CTX-M type extended-spectrumb-lactamase iso-lated from Escherichia coli. Antimicrob Agents Chemother2002; 46: 1985–8.
8. Quinteros M, Radice M, Gardella N, et al. Extended-spectrumb -lac-tamases in Enterobacteriaceae in Buenos Aires, Argentina, public hos-pitals. Antimicrob Agents Chemother2003; 47:2864–7.
9. Pitout JD, Hanson ND, Church DL, Laupland KB. Population-based laboratory surveillance forEscherichia coli–producing extended-spec-trum b-lactamases: importance of community isolates withblaCTX-M
genes. Clin Infect Dis2004; 38:1736–41.
10. Moland ES, Black JA, Hossain A, Hanson ND, Thomson KS, Pottu-marthy S. Discovery of CTX-M–like extended-spectrumb-lactamases inEscherichia coliisolates from five US states. Antimicrob Agents Che-mother2003; 47:2382–3.
11. Herna´ndez JR, Pascual A, Canton R, Martı´nez-Martı´nez L.Escherichia coliyKlebsiella pneumoniaeproductores deb-lactamasas de espectro extendido en hospitales espan˜oles (proyecto GEIH-BLEE 2000). Grupo
de Estudio de Infeccio´n Hospitalaria (GEIH). Enferm Infecc Microbiol Clin2003; 21:77–82.
12. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC defi-nitions for nosocomial infections. Am J Infect Control1988; 16:128–40. 13. McCabe WR, Jackson GG. Gram-negative bacteremia I: etiology and
ecology. Arch Intern Med1962; 110:847–55.
14. NCCLS. Methods for dilution antimicrobial susceptibility tests for bac-teria that grow aerobically: fifth edition. NCCLS document M7-A5. Wayne, PA: NCCLS,2002.
15. NCCLS. Performance standards for antimicrobial susceptibility testing, twelfth informational supplement. NCCLS document M100-S12. Wayne, PA: NCCLS,2002.
16. Vila J, Marcos MA, Jime´nez de Anta MT. A comparative study of different PCR-based DNA fingerprinting techniques for typing of the
Acinetobacter calcoaceticus-A. baumanniicomplex. J Med Microbiol 1996; 44:482–9.
17. Barret TJ, Lior H, Green JH, et al. Laboratory investigation of a mul-tistate food-borne outbreak of Escherichia coli O157:H7 by using pulsed-field gel electrophoresis and phage typing. J Clin Microbiol 1994; 32:3013–7.
18. Tenover FC, Arbeit RD, Goering RV, et al. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol1995; 33:2233–9. 19. Matthew M, Harris AM, Marshall MJ, Ross GW. The use of analytical
isoelectric focusing for detection and identification ofb-lactamases. J Gen Microbiol1975; 88:169–78.
20. Bush K, Singer SB. Effective cooling allows sonication to be used for liberation ofb-lactamases from gram-negative bacteria. J Antimicrob Chemother1989; 24:82–4.
21. Jacoby J, Bush K. Amino acid sequences for TEM, SHV, and OXA extended-spectrum and inhibitor resistantb-lactamases [cited 2005 15 June]. Available at: http://www.lahey.org/studies/webt.htm. Accessed 15 June 2005.
22. Coque TM, Oliver A, Perez-Diaz JC, Baquero F, Canton R. Genes enconding TEM-4, SHV-2, and CTX-M-10 extended-spectrumb -lac-tamases are carried by multipleKlebsiella pneumoniaeclones in a single hospital (Madrid, 1989 to 2000). Antimicrob Agents Chemother 2002; 46:500–10.
23. Oliver A, Perez-Diaz JC, Coque TM, Baquero F, Canton R. Nucleotide sequence and characterization of a novel cefotaxime-hydrolyzingb -lac-tamase (CTX-M-10). Antimicrob Agents Chemother2001; 45:616–20. 24. Rasheed JK, Jay C, Metchock B, et al. Evolution of extended-spectrum
b-lactam resistance (SHV-8) in a strain ofEscherichia coliduring mul-tiple episodes of bacteremia. Antimicrob Agents Chemother1997; 41: 647–53.
25. Simarro E, Navarro F, Ruiz J, Miri E, Gomez J, Mirellis B.Salmonella entericaserovar Virchow with CTX-M–likeb-lactamase in Spain. J Clin Microbiol2000; 38:4676–8.
26. National Institutes of Health. Basic local alignment search tool (BLAST). Available at: http://www.ncbi.nlm.nih.gov/BLAST. Accessed 15 June 2005.
27. Infobiogen. Traduction multiple. Available at: http://www.infobiogen .fr/services/analyseq/cgi-bin. Accessed 15 June 2005.
28. D‘Agata E, Venkataraman L, DeGirolami P, Weigel L, Samore M, Ten-over F. The molecular and clinical epidemiology of Enterobacteriaceae-producing extended-spectrumb-lactamase in a tertiary care hospital. J Infect1998; 36:279–85.
29. Wiener J, Quinn JP, Bradford PA, et al. Multiple antibiotic-resistant
Klebsiella and Escherichia coli in nursing homes. JAMA1999; 281: 517–23.
30. Lucet JC, Decre´ D, Fichelle A, et al. Control of a prolonged outbreak of extended-spectrumb-lactamase–producing Enterobacteriaceae in a University Hospital. Clin Infect Dis1999; 29:1411–8.
31. Lautenbach E, Patel JB, Bilker WB, Edelstein PH, Fishman NO. Ex-tended-spectrumb-lactamase-producingEscherichia coliandKlebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes. Clin Infect Dis2001; 32:1162–71.
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/
32. Bisson G, Fishman NO, Patel JB, Edelstein PH, Lautenbach E. Ex-tended-spectrumb-lactamase–producingEscherichia coliandKlebsiella
species: risk factors for colonization and impact of antimicrobial for-mulary interventions on colonization prevalence. Infect Control Hosp Epidemiol2002; 23:254–50.
33. Yagi T, Kurokawa H, Senda K, et al. Nosocomial spread of cephem-resistantEscherichia colistrains carrying multiple Toho-1–likeb -lac-tamase genes. Antimicrob Agents Chemother1997; 41:2606–11. 34. Palucha A, Mikiewicz B, Gniadkowski M. Diversification ofEscherichia
coliexpressing an SHV-type extended-spectrumb-lactamase (ESBL) during a hospital outbreak: emergence of an ESBL-hyperproducing strain resistant to expanded-spectrum cephalosporins. Antimicrob Agents Chemother1999; 43:393–6.
35. Romero L, Lo´pez L, Rodrı´guez-Ban˜o J, Herna´ndez JR, Martı´nez-Mar-tı´nez L, Pascual A. Long-term study of the frequency of ESBL-pro-ducingEscherichia coliandKlebsiella pneumoniaeisolates. Clin Micro-biol Infect2005; 11:625–31.
36. Paterson DL, Singh N, Ribs JD, Squier C, Rihs BL, Muder RR. Control of outbreak of infection due to extended-spectrum b-lactamase– producingEscherichia coliin a liver transplantation unit. Clin Infect Dis2001; 33:126–8.
37. Mulvey MR, Bryce E, Boyd D, et al. Amber class A extended-spectrum b-lactamase–producingEscherichia coliandKlebsiellaspp. in Canadian hospitals. Antimicrob Agents Chemother2004; 48:1204–14.
38. Fang H, Lundberg C, Olsson-Liljequist B, et al. Molecular epidemio-logic analysis ofEscherichia coliisolates producing extended-spectrum b-lactamases for identification of nosocomial outbreaks in Stockholm, Sweden. J Clin Microbiol2004; 42:5917–20.
39. Rodrı´guez-Ban˜o J, Pascual A, Muniain MA, et al. Description of en-demic multidrug-resistantAcinetobacter baumanniiand efficacy of a control program [abstract 1725]. In: Program and abstracts of the 40th Interscience Conference on Antimicrobial Agents and Chemotherapy (Toronto, Canada). Washington, DC: American Society for Microbi-ology,2000:428.
40. Harris AD, Karchmer TB, Carmeli Y, Samore SH. Methodological prin-ciples of case-control studies that analyzed risk factors for antibiotic resistance: a systematic review. Clin Infect Dis2001; 32:1055–61. 41. McDonald LC, Jarvis WR. Linking antimicrobial use to nosocomial
infections: the role of a combined laboratory-epidemiology approach. Ann Intern Med1998; 129:245–7
42. Paterson DL. Looking for risk factors for the acquisition of antibiotic resistance: a 21st-century approach. Clin Infect Dis2002; 34:1564–7. 43. Poirel L, Naas T, Le Thomas I, Karim A, Bingen E, Nordmann P.
CTX-M–type extended-spectrumb-lactamase that hydrolyzes ceftazidime through a single amino acid substitution in the omega loop. Antimicrob Agents Chemother2001; 45:3355–61.
at IFAPA on March 14, 2012
http://cid.oxfordjournals.org/