TítuloMotor facilitation during real time movement imitation in Parkinson’s disease: a virtual reality study
10
0
0
Texto completo
(2) rehabilitation protocol based on imitation in PD. PD patients are greatly impaired in carrying out overlearned motor programs [10] and also in performing repetitive movements [11], so we focused on a simple intransitive task: finger tapping (FT). This movement is usually imitated by the newborn [12] (therefore over-learned and stored early in motor repertoire), which is easily controllable but clearly altered in PD [11]. In line with other work in healthy subjects [5,13], this simple task allows control of the level of experience on the kind of task to be imitated [14], and clinical studies support the view that ideomotor apraxia involving intransitive movements is not present in PD [15].We therefore focused on imitation not in the classic sense of learning a new behavior, but trying to improve an impaired pattern already stored in the motor repertoire. The classic form of FT test is repetitive flexion-extension movements of the metacarpo-phalangeal joint; the test can detect arrhythmokinetic/hypokinetic alterations of movements in PD and aging [11]. Regulation of the tapping cycle during the FT is balanced between the time the finger is moving and the time the finger rests on the table. A whole set of different cyclic (motor) patterns are therefore available for a fixed tapping frequency, which includes the natural pattern. Here we investigated dopaminergic involvement in imitation of movement by evaluating PD’s ability to imitate customized finger tapping patterns and compare their ability with appropriate control subjects. Also we would like to obtain evidence for an effect of real-time movement imitation on motor execution in PD, by evaluating if some specific movement impairments in the disease can be modified during imitation, and therefore gaining grounds for devising a training protocol with the objective of inducing lasting improvements in motor execution after an imitation program. We used a Virtual Reality (VR) environment, an advantageous resource for evaluating and treating a number of pathologies [16]. It provides outcomes indistinguishable from real world in evaluating motor patterns [17] and allows presentation of motor patterns to be imitated in controlled and customized ways, not easily achievable in the real world. The VR system [17] presented a virtual avatar seated at a table, executing finger tapping movements in predefined patterns to be imitated by the subjects. Therefore we compared execution during self-paced, natural patterns with the new patterns to imitate. While the system allows presentation in 1st person (egocentric) or 3rd person perspective the 1st person perspective may offer advantages; much like children preferring a “like-me” model during imitation [13]. In basic science terms, our research hypothesis investigated the involvement of the dopaminergic system in motor imitation, by evaluating subjects in which this system is deficient. The initial step characterized natural finger tapping patterns for each subject/patient; PD vs. age-matched or young controls. These patterns were then either directly translated into VR (“Self-Paced VR ”) or modified to be imitated (“Imitation VR ”) by the different sets of subjects. Success in such an imitative action is a necessary small step towards testing VR as an environment suitable for rehabilitativework in motor system disorders. A second hypothesis predicts that during the imitation PD can use the information available (the stimulus presented e a moving hand-) to reduce some of parkinsonian motor impairments, like arrhythmokinesis. This will produce a reduction of the cycle time variability while imitating the avatar’s finger tapping movement.. 2. Methods All experimental subjects signed consent forms. The protocol conformed to the declaration of Helsinki and was approved by the Ethics Committee of the University of A Coruña (Spain) (CE-UDC 23/092009). 2.1. Participants 28 participants were recruited: 9 healthy young (HY), 9 healthy elderly (HE) and 10 non-demented idiopathic Parkinson’s Disease (PD) subjects. Because one objective of the study was to investigate the potential influence of the dopaminergic system on motor imitation, PD were evaluated in absence of dopaminergic drugs; disease severity was rated as in stages II-IV OFF of the Hoehn and Yahr scale. OFFdose was at least 12 h since their last antiparkinsonian medication intake; 24 h for slow release drugs. All PD had no history of freezing of gait, and were examined using the motor part of UPDRS scale (Supplementary Table 1). Participants were excluded if they presented any neurological disease (other than PD in the case of the patients); musculoskeletal impairment disturbing the execution of the task, not-.
(3) correctable visual deficiency, or dementia (MMSE score < 24). PD had a mean age of 67.1 yrs (_2.9, Standard Error of Mean, SEM). HY and HE were 27.3 yrs (± 2.1) and 66.2 yrs (± 2.9), respectively. All groups were screened for hand dominance through Edinburgh Handedness Inventory [18], PD were also asked about their hand dominance before the first manifestation of the disease. 2.2. Protocol Self-paced tapping in VR is known to match self-paced tapping in the real world in the groups of interest [17].We performed 3 blocks of tapping: Self-Paced REAL , Self-Paced VR , and Imitation VR ; the 3 blocks were performed at comfort, and slow-comfort rates. Subjects were asked to tap with their index finger of their dominant hand. For self paced conditions each subject was told “tap at your comfortable rate”, and “tap at your comfortable slow rate”, either in Self-Paced REAL , and Self-Paced VR while looking at their index finger. For imitation, ImitationVR, they were asked to tap imitating the avatar’s animated finger pattern, “tap imitating the movement of the finger” while looking at the index finger of the avatar. For Self-Paced REAL subjects executed the movements in the real environment, at both the comfort and slow-comfort rates (for slow-comfort conditions subjects were asked to tap at the most comfortable tapping rate slower than the natural confort pattern). Subsequently, subjects tapped at the same rates but immersed in the virtual world (Self-Paced VR ). In this condition the VR system tracked real-time the finger tapping executed by the subject and reproduced it by means of the virtual avatar adopting the same posture and position as the subject. Subjects also tapped in VR during the imitation protocol. Here they were asked to imitate the pattern animated by the avatar (Fig. 1). During Imitation VR we used each subject’s own Self-Paced REAL comfort and slow-comfort tapping-rates as the frequencies of movement to be imitated, but modifying the structure of the movement. This was done by reducing contact-time to ≈ 0 and increasing movement-time (Fig. 1c), so that the finger was moving throughout the cycle. In all VR cases, actions were observed through the head mounted display (HMD, Fig. 1). Each block of 50 tapping cycles was performed twice at Comfort and Slow-comfort tapping-rates. Imitation abilities were evaluated in VR conditions (Self-Paced VR vs. Imitation VR ); the order of presentation was randomized. Self-Paced REAL , always performed first and was used to set the avatar’s tapping frequencies for Imitation VR . 2.3. Material The tapping cycle was recorded by an event detector comprising a conductive plate and flexible conductive ring attached to each subject’s distal phalange. For PD and HE only, we recorded surface EMG activity on the extensor digitorum (SX230 electrodes, Biometrics Ltd, amplified x1000; filtered: 20-450 Hz; sampling frequency 1 KHz). One of the investigators (blind to the condition) determined the start and end of each burst off-line in MatLab (The Mathworks, Ltd). The signal was amplitude normalized, full-wave rectified and averaged using a 10 ms time window. Normalization involved dividing each point by a maximum obtained during a maximal voluntary contraction (index extension against an un-moveable load). 2.4. Variables We calculated the tapping cycle frequency (FQ, in Hz); Contact-time (ms, finger in contact with the plate); Movement-time (ms, finger moving); and Coefficient of Variation (CV, %) of tapping cycle duration. EMG power was expressed (mV, RMS (root mean squared)) for each burst, as % of SelfPace REAL EMG value..
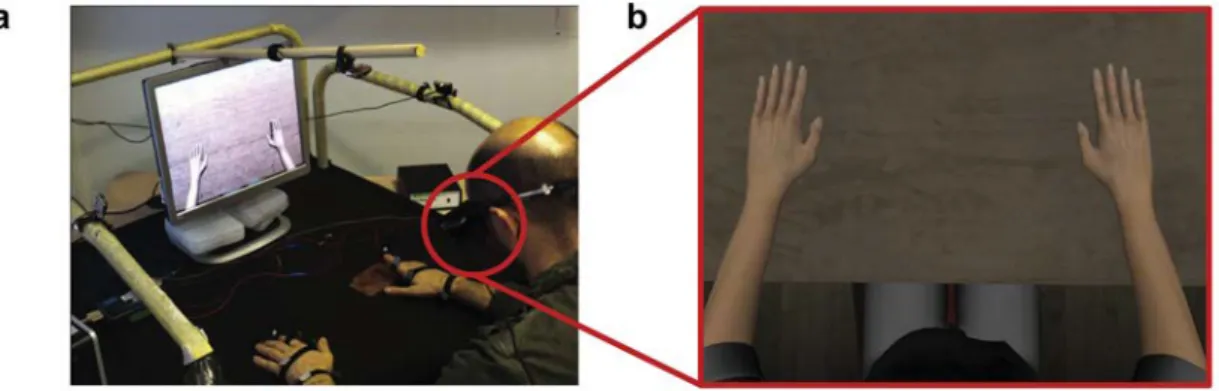
(4) 2.5. Statistical analysis 2.5.1. Preliminary analyses We characterized the tapping profile during Self-Paced REAL at comfort and slowcomfort tapping-rates. For this an ANOVA with repeated measures (2 x 3 ANOVA-RM) was performed for FQ, with factor TAPPING_RATE at two levels (comfort; slow-comfort), and GROUP at three levels (HY, HE, PD). Another 2 x 2 x 3 ANOVA-RM was performed; with an extra factor, CYCLE_PHASE with two levels (Contact-time and Movement-time, each in ms, as % of tapping cycle). In the patients group, we also evaluated any potential interaction between the tapping rate and its CV with disease severity (UPDRS motor section ). This was done for both comfort and slow-comfort rates, when not imitating in VR. For this, we calculated Pearson’s Correlation Coefficients.. Fig. 1. Virtual Reality System. a) Subjects wore a Head-Mounted Display unit (HMD) and were “immersed” in VR, showing the avatar in 1st person perspective; observing the world only through the HMD, (the PC monitor illustrated was a copy of the display for the experimenter). b) The “field of view” of the immersed subject was arranged such that their own hands were “in register” with those of the avatar. c) Normal tapping was translated from the subjects own recorded movements, left, to the VR avatar, right, showing still-frame illustrations of contact and movement components of the tapping pattern- these could be adjusted while maintaining the required frequency.. 2.5.2. Main outcomes: movement imitation and clinical relevance 2.5.2.1. Imitation abilities. The subject’s ability to imitate the motor pattern presented in VR was evaluated by a 2 x 2 x 2 x 3 ANOVA-RM; as above but adding the factor CONDITION, with two levels (Self-Paced VR ; Imitation VR ). This allowed us to evaluate changes in CYCLE-PHASE (Contact and Movement-times) between GROUPs, when the CONDITION was imitation (compared to self-pace) at confort and slow-comfort TAPPING_RATEs. 2.5.2.2. Clinical relevance: electromyographic and kinematic profile during imitation. Because PD show an impaired execution of FT, we analyzed EMG activity, CV of cycle time, and cycle time (as FQ). This would provide insight on a potential role for imitation in movement rehabilitation in PD. We use the same.
(5) 3 x 2 x 2 ANOVA-RM model for this analysis, with factors GROUP, CONDITION and TAPPING_RATE. Normality of distributions was assessed by a one-sample Kolmogórov-Smirnov test. UnivariateANOVA was used and therefore degrees of freedom were corrected with Greenhouse Coefficients (ε) in the case of sphericity violation, assessed by the Mauchly test. Significance was set at p < 0.05. In each figure, values are mean ± SEM.. 3. Results 3.1. Characterization: execution in absence of imitation 3.1.1. Self-paced tapping patterns at comfort and slow-comfort rates Participants significantly reduced their tapping rate at slowcomfort vs. comfort self-paced tapping rates, as expected (F(1,25) = 25.394 p < 0.001). At both tapping rates, however, PD tapped faster than the other two groups (F(2,25) = 5.918 p = 0.008, Fig. 2a). Unexpectedly, there was a significant difference in the pattern of slowing seen. All groups increased contact-time as tapping frequency reduced over time (Fig. 2b), but PD and HE slowed their tapping frequency by increasing both Contact and Movementtimes, maintaining the ratio of Contact and Movement time within the cycle (Fig. 2c,d) while HY Movementtimewas unaltered but Contact-time increased (Fig. 2b) a significant difference (F(2,25) = 4.740 p = 0.018). Supplementary Table 2 shows the correlation between disease severity (UPDRS motor section ) and motor execution (CV and tapping rate), at slow-comfort and comfort selfpaced rates. 3.2. Main outcomes: motor imitation and clinical relevance 3.2.1. Dopaminergic deficiency has no effect on imitating motor patterns Having defined tapping profiles at self-paced Comfort and Slow-Comfort rates, the subject’s ability to imitate was evaluated by examining how they adapt their tapping when asked to imitate the avatar’s animated pattern, a pattern showing a continuously moving finger at the appropriate frequencies. The main finding is that PD were clearly able to imitate this change in finger tapping pattern successfully, at both tapping rates. The way they adapted their execution to the finger movement to be imitated was not significantly different to HE or HY subjects (F(2,25) = 1.954 p = 0.163). All groups successfully modified their tapping pattern when imitating by reducing contact-time and increasing movement-time (F(1,25) = 9.658 p = 0.005); the effect was significantly greater, however, at the SlowComfort rate (F(1,25) = 5.246 p = 0.031; Fig. 3ab, Fig. 4a). When the tapping frequency was analyzed, unsurprisingly, all groups tapped slower during the slow condition (F(1,25) = 36.235 p < 0.001), regardless of whether this was during Selfpaced VR or Imitation VR (F(1,25) = 0.820 p = 0.374). Interestingly, the tapping frequency during Self-paced VR and Imitation VR was not significantly different at each rate, Comfort or Slow-comfort (F(1,25) = 1.932 p = 0.177; see Figs. 3c and 4b). This means that the change in tapping pattern observed during imitation was not influenced by a change in tapping frequency. 3.2.2. Clinical relevance: inter-tap variability and EMG power during imitation As expected, variability was different between groups (F(2,25) = 5.731 p = 0.009), and PD was larger than HE or HY (p = 0.033 and p = 0.003 respectively). However, Imitation VR induced a change in CV which depended upon the tapping-rate. Slow-Comfort rate CV was significantly reduced during Imitation VR (F(1,25) = 6.131 p = 0.020, see Fig. 4c). This reduction in CV when imitating at slow rates was observed in all groups (F(2,25) = 1.461 p = 0.251). Further, comparing PD with HE, the power of the EMG was increased during Imitation VR (F(1,17) = 28.870 p< 0.001), though to a different extent in both groups (F(1,17) = 5.443 p = 0.032). At Slow both PD and HE increased their myoelectric activity (p = 0.007); such effect was only significant at Comfort for theHE (p<0.001; Fig. 4d-f)..
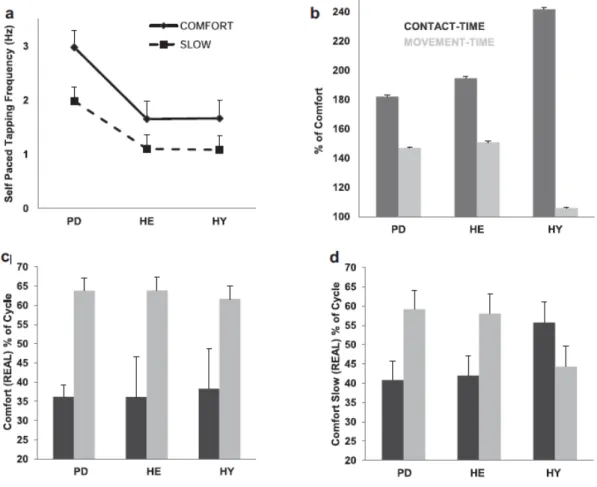
(6) Fig. 2. Tapping pattern characterization. a) Tapping rates were significantly reduced when subjects were instructed to use slow comfort tapping-rate e slow-comfort vs. Confort (F(1,25) = 25.394 p < 0.001), though PD tapped significantly faster than the other groups (F(2,25) = 5.918 p = 0.008). b) In relation to Comfort (100%), this reduction in the tapping rate was due to increased contact time (p = 0.001 PD & HE; p = 0.018 HY). Movement time was unchanged by HY; PD & HE’s movement times significantly increased (p = 0.007). c,d) The proportion of movement and contact times within the cycles was similar in all groups at Comfort and Slow (~40% contact and ~60% movement time), except for HY at Slow.. 4. Discussion We present two main results. Firstly, successful imitation by our PD suggests that dopaminergic systems known to be damaged are not involved in imitation of simple motor patterns within the subject’s motor repertoire. Secondly, despite the fact that a high temporal variability of movements and lower recruitment efficiency are well known features of PD and aging, these subjects increased the power of their myoelectric activity during imitation, and reduced variability in imitated movements at slower tapping rates. 4.1. Imitation and dopaminergic system Since one objective of the studywas to understand the role of the DAergic system in imitation in the task proposed, we evaluated PD OFF-dose. It can be approached by comparing subjects with pathologic vs. physiologic DAergic systems (HE and HY). This way the DAergic role in imitation is better understood if comparing PD OFFdose to healthy subjects rather than to PD ON-dose, because ONdose PD do not actually have a normal, functional DAergic system, despite the DA replacement, which sometimes leads to motor manifestations like dyskinesias. However, considering the reduction in the CV observed in our healthy subjects, it is likely than a putative therapeutic effect of imitation might be also present in ON-dose PD..
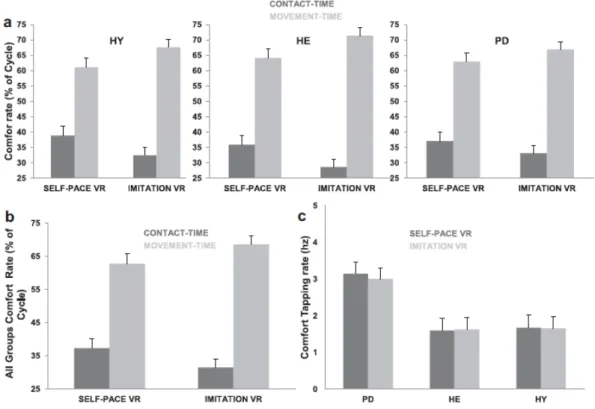
(7) Fig. 3. Imitation at Comfort rate. a) There was no significant difference between groups’ behavior when imitating (F(2,25) = 1.561 p = 0.230). b) All groups reduced the proportion of the cycle in contact time while imitating (pooling the three groups; p = 0.004). c) Tapping frequency during Self-paced VR and Imitation VR was not significantly different at each rate.. 4.2. Mechanism for improving motor control Instability in finger tapping frequency is a known feature in both PD and aging [11], associated with disruption to stride and gait patterns [19] and falling [20]. Sensory cueing is a well-studied strategy used in order to induce sensorimotor synchronization, leading to movement facilitation, chiefly in PD [4,21]. Its physiological basis seems to be an apparently decreased involvement of the BG-SMA loop, which is known to be altered in the disease, if movements are executed in presence of rhythms [22,23]. However, while reduction in the variability of the movements has been reported using auditory sensorimotor integration [21], this seems to be less effective if temporal visual cues are presented [21]. The difference here is that by using imitation of an observed moving hand, rather than an abstract “temporal pattern stimulus”, PD might become less dependent on the BG-AMS loop or learn to compensate for the deficit by means of the involvement of the mirror neuron system (MNS) [24]. These neurons respond both during observation and execution of appropriate motor actions, including digit movements [5], and studies involving imitation of simple finger extension presented in 3rd person perspective also show the involvement of mirror structures [5]. Our study utilized a 1st person perspective, instead of the 3rd person perspective [5]. While “natural” imitation, by definition, uses a 3rd person perspective, it is known than imitation of a 1st person perspective shares networks involved in the 3rd person perspective, though with a larger involvement of the somatosensory cortex [13]. This might involve the sense of “agency” [25], and was the reason for our choice in this study. Also, a “like-me” model of imitation seems to be preferred during childhood development [26] e a common example is learning to dance, where a teacher adopts a 1st person “role model” position. It is not then surprising that the reduction in the temporal variability of the pattern during imitation was observed at comfort-slow rate, since comfort rate is likely to be more “locked” within the motor repertoire and therefore less adaptable. Interestingly, the pattern we presented might be not the better to reduce variability in finger tapping (for that purpose a pattern with a stable and similar contact-time and movement-time to the natural tapping pattern would be required), though it allowed a proper characterization of imitation capabilities. Remarkably, the tapping frequency was not changed by the.
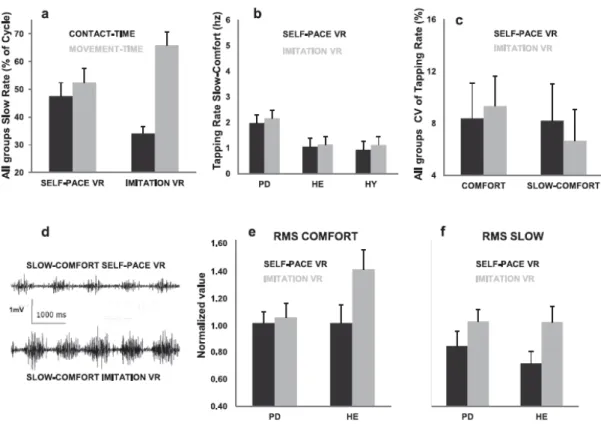
(8) process of imitating (Imitating RV vs. Selfpace RV ; either at comfort or slow-comfort rates) ruling out an effect of tapping-rate drift on outcomes. From a clinical point of view increased EMG power in the extensor digitorum muscle when imitating is important, since impairment in the pattern of muscle activation is a reported feature in PD [2]. Therefore, this suggests that a rehabilitation program based on imitation might be useful to induce central adaptations leading to lessening of symptoms of the disease.. Fig. 4. Imitation at Slow rate (a,b), and effect of imitation on stability of movement (c), and on motor recruitment (d-f). a) Group responses while imitating at slow-comfort rate were not significantly different (F(2,25) = 2.200 p = 0.132), suggesting that Parkinsonian-induced dopaminergic deficiency did not affect performance in the task. All subjects adapted their finger movement in response to observing the continuously moving finger pattern by significantly reducing their contact times (p = 0.004). b) Imitation did not induce significant changes in the slow tapping rates of the different groups. c) At Comfort rate none of the groups significantly changed the temporal stability of the movement when imitating. However, at slow rate imitation lead to a significant reduction in the variability of movement (F(1,25) = 6.131 p = 0.020), an effect which was also not different for the Groups (F(2,25) = 1.461 p = 0.251). d) shows a representative EMG-recording in a subject (PD) tapping at Slow comfort either during Self-pace VR (upper trace), or Imitation VR (lower trace). e) The EMG power (expressed in relation to RMS-Self-Paced REAL ) was increased during imitating in the HE (p = 0.001) at comfort rate; f) at slow rates, however, imitation induced also greater EMG power (p = 0.007) in both PD and HE.. 4.3. Motor control adaptation underlying slowing finger tappingrate in different groups At both rates PD had faster tapping rates than the healthy groups, reflecting the PD tendency to hasten their rhythmic movements [19]. We have also described how different subjects slowed their self-paced tapping-rate. HE and PD increased both movement and contact-times, on the other hand HY kept constant movement time, but increased contact-time. PD and aging are associated with impairment in rhythm formation [11], thus increasing movement-time might be a compensatory mechanism mediated by a greater involvement of cerebellum [27] (considered a comparator of current movement vs. movement intent), to be less dependent on the BG, and allowing better rhythm maintenance..
(9) 5. Conclusion The dopaminergic system seems not to have a key role during imitation of motor patterns available in PD subject’s motor repertoire. Improvement in motor control observed in subjects suggests a possible use for imitation protocols oriented to rehabilitate motor patterns impaired in aging and PD. Further research is needed in order to know if imitation training for several days leads to off-line motor adaptation in patients’ motor control.. Conflict of interest The authors assent that there are no conflicts of interest.. Acknowledgment No specific regulations. These may be published on line at the discretion of the editor.. Appendix A. Supplementary data Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.parkreldis.2013.08.005.. References [1] Rizzolatti G, Fabbri-Destro M, Cattaneo L. Mirror neurons and their clinical relevance. Nat Clin Pract Neurol 2009;5:24-34. [2] Hallett M, Khoshbin S. A physiological mechanism of bradykinesia. Brain 1980;103:301-14. [3] Asmus F, Huber H, Gasser T, Schols L. Kick and rush: paradoxical kinesia in Parkinson disease. Neurology 2008;71:695. [4] Arias P, Cudeiro J. Effect of rhythmic auditory stimulation on gait in Parkinsonian patients with and without freezing of gait. PLoS One 2010;5:e9675. [5] Iacoboni M, Woods RP, Brass M, Bekkering H, Mazziotta JC, Rizzolatti G. Cortical mechanisms of human imitation. Science 1999;286:2526-8 [6] Vogt S, Buccino G, Wohlschlager AM, Canessa N, Shah NJ, Zilles K, et al. Prefrontal involvement in imitation learning of hand actions: effects of practice and expertise. Neuroimage 2007;37:1371-83. [7] Alegre M, Rodriguez-Oroz MC, Valencia M, Perez-Alcazar M, Guridi J, Iriarte J, et al. Changes in subthalamic activity during movement observation in Parkinson’s disease: is the mirror system mirrored in the basal ganglia? Clin Neurophysiol 2010;121:414-25. [8] Benecke R, Rothwell JC, Dick JP, Day BL, Marsden CD. Simple and complex movements off and on treatment in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry 1987;50:296-303. [9] Bradley VA, Welch JL, Dick DJ. Visuospatial working memory in Parkinson’s disease. J Neurol Neurosurg Psychiatry 1989;52:1228-35. [10] Jahanshahi M, Jenkins H, Brown RG, Marsden CD, Passingham RE, Brooks DJ. Self-initiated versus externally triggered movements .1. An investigation using measurement of regional cerebral blood flow with PET and movementrelated potentials in normal and Parkinson’s disease subjects e reply. Brain 1996;119:1046-8. [11] Shimoyama I, Ninchoji T, Uemura K. The finger-tapping test. A quantitative analysis. Arch Neurol 1990;47:681-4. [12] Meltzoff AN, Moore MK. Imitation of facial and manual gestures by human neonates. Science 1977;198:75-8. [13] Jackson PL, Meltzoff AN, Decety J. Neural circuits involved in imitation and perspective-taking. Neuroimage 2006;31:429-39..
(10) [14] Calvo-Merino B, Glaser DE, Grezes J, Passingham RE, Haggard P. Action observation and acquired motor skills: an FMRI study with expert dancers. Cereb Cortex 2005;15:1243-9. [15] Leiguarda RC, Pramstaller PP, Merello M, Starkstein S, Lees AJ, Marsden CD. Apraxia in Parkinson’s disease, progressive supranuclear palsy, multiple system atrophy and neuroleptic-induced parkinsonism. Brain 1997;120(Pt 1):75-90. [16] Riva G. Applications of virtual environments in medicine. Methods Inf Med 2003;42:524-34. [17] Arias P, Robles-García V, Sanmartin G, Flores J, Cudeiro J. Virtual reality as a tool for evaluation of repetitive rhythmic movements in elderly and Parkinson’s disease patients. PLoS One 2012;7:e30021. [18] Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 1971;9:97-113. [19] Nakamura R, Nagasaki H, Narabayashi H. Disturbances of rhythm formation in patients with Parkinson’s disease: part I. Characteristics of tapping response to the periodic signals. Percept Mot Skills 1978;46(1):63-75. [20] Schaafsma JD, Giladi N, Balash Y, Bartels AL, Gurevich T, Hausdorff JM. Gait dynamics in Parkinson’s disease: relationship to parkinsonian features, falls and response to levodopa. J Neurol Sci 2003;212:47-53. [21] Arias P, Cudeiro J. Effects of rhythmic sensory stimulation (auditory, visual) on gait in Parkinson’s disease patients. Exp Brain Res 2008;186:589-601. [22] Del Olmo M, Arias P, Furio MC, Pozo MA, Cudeiro J. Evaluation of the effect of training using auditory stimulation on rhythmic movement in parkinsonian patients e a combined motor and F-18 -FDG PET study. Parkinsonism Relat Disord 2006;12:155-64. [23] Cunnington R, Iansek R, Bradshaw JL, Phillips JG. Movement-related potentials in Parkinson’s disease. Presence and predictability of temporal and spatial cues. Brain 1995;118(Pt 4):935-50. [24] Gallese V, Fadiga L, Fogassi L, Rizzolatti G. Action recognition in the premotor cortex. Brain 1996;119(Pt 2):593-609. [25] Nahab FB, Kundu P, Gallea C, Kakareka J, Pursley R, Pohida T, et al. The neural processes underlying selfagency. Cereb Cortex 2011;21:48-55. [26] Meltzoff AN, Decety J. What imitation tells us about social cognition: a rapprochement between developmental psychology and cognitive neuroscience. Philos Trans R Soc Lond B Biol Sci 2003;358:491-500. [27] Rascol O, Sabatini U, Fabre N, Brefel C, Loubinoux I, Celsis P, et al. The ipsilateral cerebellar hemisphere is overactive during hand movements in akinetic parkinsonian patients. Brain 1997;120(Pt 1):103-10..
(11)
Figure
Documento similar