Standardised
cement
augmentation
of
the
PFNA
using
a
perforated
blade:
A
new
technique
and
preliminary
clinical
results.
A
prospective
multicentre
trial
C.
Kammerlander
a,*
,
F.
Gebhard
b,
C.
Meier
c,
A.
Lenich
d,
W.
Linhart
e,
B.
Clasbrummel
f,
T.
Neubauer-Gartzke
g,
M.
Garcia-Alonso
h,
T.
Pavelka
i,
M.
Blauth
aa
DepartmentofTraumaSurgeryandSportsMedicine,MedicalUniversityofInnsbruck,Innsbruck,Austria
b
DepartmentofTraumatology,Hand-,Plastic-,andReconstructiveSurgery,CenterofSurgery,CenterofMusculoskeletalResearch,UniversityofUlm,Ulm,Germany
c
DepartmentofTraumatology,StadtspitalWaid,Zu¨rich,Switzerland
dDepartmentofTraumatology,KlinikumRechtsderIsar,TechnicalUniversityofMunich,Munich,Germany e
DepartmentofOrthopedicsandTraumaSurgery,SLKKlinikenHeilbronn,Heilbronn,Germany
f
DepartmentofTraumaSurgery,ZollernalbKlinikum,Balingen,Germany
g
DepartmentofTraumaSurgery,KlinikenNordoberpfalz,Weiden,Germany
h
DepartmentofOrthopedics,HospitalUniversitarionRioHortega,Vallodolid,Spain
i
DepartmentofTraumaSurgery,MedicalUniversityofPlzen,AlejSvobody80,CZ-30460Plzen,CzechRepublic
Pertrochanteric fractures are a rising major health-care problemintheelderlyandtheiroperativestabilisationtechniques arestillunderdiscussion.Whereasthedynamichipscrewisthe standardfixationmethodforstableA1fractures,1thereisatrend to use intramedullary implants to fix unstable A2 and A3 fractures.2–7
RecentstudiesrevealedthatthePFNAisaveryeffectiveimplant for the fixation of pertrochanteric femoral fractures.7,8
Blade-related complications withthe PFNA, suchas cut-out, and cut throughwitheithermedialblademigrationintothehipjointor lateralblademigrationarereportedfrom0.6%9over2.6%8upto
3.6%.7However,severalotherimplantswhichuseascrewdesign
for thecephalicpartoftheimplant leadtocut-out ratesupto 16%.2,10,11
Acrucialpointisthatthesecatastrophicfailuresmainlytake place in severe osteoporotic bone.12 However, the
above-men-tioned studies7–9 do not only include fragility fractures and
thereforethecut-outrateintheelderlymaybeevenhigher.
ARTICLE INFO
Articlehistory: Accepted11July2011
Keywords: Hipfracture Augmentation PMMA Cementleakage PFNA Cut-out
Cementaugmentation Osteoporosis
Corticalthicknessindex Cementdistribution
SUMMARY
Pertrochantericfracturesarearisingmajor health-careproblemintheelderlyandtheiroperative stabilisationtechniquesarestillunderdiscussion.Furthermore,complicationslikecut-outarereported tobehighandimplantfailureoftenisassociatedwithpoorbonequality.ThePFNA1
withperforated blade offers apossibility for standardisedcement augmentation using a polymethylmethacrylate (PMMA)cementwhichisinjectedthroughtheperforatedbladetoenlargetheload-bearingsurfaceand to diminishthe stresses on the trabecular bone. The current prospective multicentrestudy was undertakentoevaluatethetechnicalperformanceandtheearlyclinicalresultsofthisnewdevice.
InnineEuropeanclinics,59patients(45female,meanage84.5years)sufferingfromanosteoporotic pertrochantericfracture(Arbeitsgemeinschaftfu¨rOsteosynthesefragen,AO-31)weretreatedwiththe augmentedPFNA1
.Primaryobjectiveswereassessmentofoperativeandpostoperativecomplications, whereasactivitiesofdailyliving,pain,mobilityandradiologicparameters,suchascementdistribution aroundthebladeandthecorticalthicknessindex,weresecondaryobjectives.
Themeanfollow-uptimewas4monthswhereweobservedcallushealinginallcases.Thesurgical complicationratewas3.4%withnocomplicationrelatedtothecementaugmentation.Morethan one-halfofthepatientsreachedtheirprefracturemobilitylevelwithinthestudyperiod.Ameanvolumeof 4.2mlofcementwasinjected.Wedidnotfindanycut-out,cutthrough,unexpectedblademigration, implantlooseningorimplantbreakagewithinthestudyperiod.
Ourfindingsleadustoconcludethatthestandardisedcementaugmentationusingtheperforated blade forpertrochanteric fracturefixation enhancesthe implantanchorage within thehead–neck fragmentandleadstogoodfunctionalresults.
ß2011ElsevierLtd.Allrightsreserved.
*Correspondingauthorat:DepartmentofTraumaSurgeryandSportsMedicine, MedicalUniversityofInnsbruck,Anichstrasse35,A-6020Innsbruck,Austria. Tel.:+4351250480882.
E-mailaddress:[email protected](C.Kammerlander).
ContentslistsavailableatScienceDirect
Injury
j ou rna l h ome p a ge : w ww . e l se v i e r. co m/ l oc a te / i n j ury
Several biomechanical investigations on human cadaveric proximalfemoral fracturesshowed a higher cut-out resistance whenthe devicewasaugmented withpolymethylmethacrylate (PMMA)cement.13,14
Augmentation offixation devicesenlarges thebone–implant interfaceandleadstoahigherstabilityalsoinclinicaluse.10,15–21A
mainproblemregardingaugmentationatthehipwasthelackofa device for controlled cement placement around the implant.22
Furthermore,thediscussionaboutcement-relateddisturbanceof thebonemetabolismisongoing.13,23,24However,severalstudies
reportno damagetothecartilage orthebone itselfby cement augmentation.25–28Thecurrentprospectivemulticentrestudywas
undertakentoevaluatetheearlyclinicalresultsandthetechnical performanceofthenewstandardisedaugmentationforthePFNA blade.Toourknowledge,thisisthefirstreportonthisdevice.
Materialsandmethods
The study was performed at nine orthopaedic departments betweenOctober2009andJuly2010.Theinclusioncriteriawereas follows:pertrochantericfracture(Arbeitsgemeinschaftfu¨r Osteo-synthesefragen/Orthopaedic Trauma Association, AO/OTA 31A), age65yearsandabove,low-energytraumaandsignedinformed consent.Patientswithapathologicalfracture,anypatientswith active malignancy, organ transplantation or infection were excluded.Theethicalcommissionapprovedthestudyandevery singlepatientsignedtheinformedconsentform.Atotalnumberof 78patientshavebeenincluded.Nine(11.6%)caseswerelostto follow-up due to concurrent indisposition or weakness, which madeanadditionalevaluationimpossible.Tenpatientsdiedfor reasonsnotrelatedtothesurgicalprocedure.Theremaining59 patientswerefollowedupaccordingtothestudyprotocol.
Operativetechnique
The Proximal Femur Nail Antirotation (PFNA, Synthes1
, Switzerland)is available in foursizes (standard,small, XS and long)withrightandleftoptionsforthelongnail.Theperforated blade(Fig.1)hasthreeholesateverydeepeningofthehelix.A side-opening cannula (Fig. 2) allows for deliberate cement placement through the holes of the blade. Augmentation is performed with a high-viscosity PMMA cement (Traumacem, Synthes1
,Switzerland). Fracture reduction and implantation of thePFNAareperformedaspreviouslyreported7,9and,insteadof
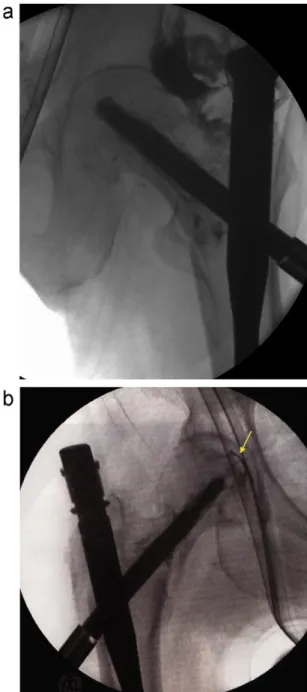
thestandard blade,theperforatedbladeis used.Itisofutmost importancetonotperforatethefemoralheadwhendrillingthek -wiretodeterminethepositionofthehelicalblade.Attheendofthe usualprocedure and before augmentation, a perforation in the jointhastobeexcludedtoavoida leakage.Therefore,the side-opening cannula is inserted into the PFNA blade and some customarywater-solublecontrastmediumisappliedwithausual syringe. If there is no contrast fluid leakage into the hip joint detected,theprocedureistobecontinued.Fig.3showsthetypical
distributionofthecontrastmedium(a)andacaseofleakage(b). Thecementismixedassuggestedbythemanufacturerandfilled intosyringeswithastandardisedset.Theside-openingcannula has to be primed with3ml of cement. The syringes are then attachedtotheside-openingcannulaandthecementisinjected under fluoroscopic control. During injection, the side-opening cannulacanberotatedtoplacethecementindifferentdirections. Afterfinishingtheinjection,thecannulahastoberemoved.The augmentation process lasts around 10–15min. Fig. 4 shows a representativecaseofstandardisedcementaugmentationofthe perforated PFNA blade in a 87-year-old lady withan unstable pertrochantericfracture.
Outcomeparameters
TheWHOPerformanceScore29wasusedtomeasurethequality
oflifebeforeandafterthefracture.Itconsistsoffivelevelsinwhich
Fig.1.Theperforatedblade.
Fig.2.Thesideopeningcannulawhichisusedtoinjectthecement.
Fig.3.Imageintensifierpicswithtypicalcontrastmediumdistribution(a)anda caseofleakageofcontrastmediumintothehipjoint(b)whichconsequently prohibitscementaugmentation.
C.Kammerlanderetal./Injury,Int.J.CareInjuredxxx(2011)xxx–xxx 2
G Model
0meansfullactivitywithoutrestrictionand4meanscompletely disabledandtotallyconfinedtobedorchair.
TheParker MobilityScore30wasused toassess thewalking
ability before the accident and at follow-up. The particular capabilitytowalkinside,walkoutsideandhavingsocialcontact isevaluatedinfourlevelswith‘‘nodifficulty,’’‘‘alone,’’‘‘withhelp fromanotherperson’’and‘‘not atall.’’Amaximum of9 points meansunlimitedwalkingability.Inaddition,theuseofawalking aid was documented for every patient before and after the accident.
Painwas assessedusing the visualanalogue scale (VAS),as previouslydescribed31andwidelyknown.TheVASwasfoundto
havegoodmeasurementpropertiesassessingpaininhipfracture patients.32
OnthepreoperativeX-rays,thefracturepatternandthecortical thickness index33 were assessed. The cortical thickness index showsa significantpositive correlationwiththeT-Scoreof the femoralneck34andwasthereforeusedtoclassifythelocalbone
qualityinourstudypopulation.Acorticalthicknessindexlower
than0.40 (lateralfilm)and0.50 (anterioposterior(ap)film)has beendescribedasathresholdforosteoporosiswhereallmeasured femorahadalocalbonemineraldensitylowerthan2.5standard deviationsbelowthepeakbonemass,whichistheWorldHealth Organization(WHO)definitionofosteoporosis.34
On the postoperative X-rays, we evaluated the quality of fracturereductionasanatomic(nodisplacement),near-anatomic (<3mmdisplacementor5–108varus/valgusand/oranteversion/ retroversion) or non-anatomic (>3mm displacement or >108
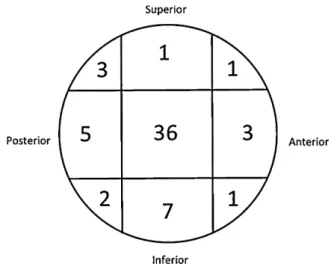
varus/valgusand/oranteversion/retroversion).6,9Furthermore,the position of the PFNA blade was evaluated and categorised, as previouslydescribed6,7bydividingthefemoralheadintosuperior,
centralandinferiorthirdsontheapradiographandintoanterior, central and posterior thirds on the lateral radiograph (Fig. 5). Cement distribution was measured in relation to the blade. Therefore, the plain X-rays in both ap and lateral view were assessedbyusingthesoftwareOsirixTM,whichallowsdrawingthe
bordersofthecementandcalculatingthesquarecentimetresof the marked area. The blade was subdivided in its middle in
longitudinaldirectiontomeasurethedistributionofcementabove andbelowthebladeaswellascentrallyintheapradiograph,in which‘centrally’meansthearea‘b’inFig.6fromthetipofthe bladetowardsthepelvisinthelongitudinaldirectionoftheblade. Measurementsinthelateralradiographwereconductedventrally, dorsallyandagaincentrallytotheblade.Theareaswerecalculated inrelationtotheareaofthefemoralhead(Fig.6).Furthermore,the amountofinjectedcementwasdocumented.Onthefollow-up X-rays,signsoffracturehealingwereassessed.Themigrationofthe blade within the head–neck fragment and the lateral blade migrationweremeasuredaspreviouslydescribed.35,36
Intra-operativecomplications includedanyunforeseenevent duringtheaugmentation,suchasperforationwiththeguidewire into the hipjoint and cement leakage. Potential postoperative complicationswerecuttingoutofthebladefromthefemoralhead, cutting through the blade centrally, any unexpected blade migration, loosening of the blade, implant breakage, infection, additionalfracture or bone-healing disturbances and anyother generalcomplicationwithinthefollow-upperiod.
Statisticalanalysis
Statistical Packagefor Social Sciences (SPSS)16.0(SPSSInc., Chicago,IL,USA)wasusedforstatisticalanalysis.Allbaselineand follow-upparametersweredescribedusingstandarddescriptive statistics.Metricscaleddataarereportedasarithmeticmeanand categoricaldataasabsolutefrequencyandpercentagedistribution. Depending on the distribution form, a t-test for independent variablesoranon-parametricMann–WhitneyUtestwasused.The Kolmogorov–Smirnov test was used to assess the distribution form.Achi-squaretestoraFisher’sexacttestwasusedtoanalyse categoricaldata.Theprobabilitylevelwassetasp<0.05.
Results
Toinvestigatetheeffectofthestandardisedcement augmen-tation,59patientswereanalysed.Meantimetofollow-upwas4 months(68–355days).ThedemographicsareshowninTable1. Associatedinjurieswerenotedintwopatients.Themajorityofthe patients sustained an unstable pertrochanteric fracture (A2/3; 74.5%).Only20.3% wereindependentlymobile(ParkerScore9) before their fracture. Mean Parker scores were 4.5 before the fractureand3.8atfollow-up.Atthefollow-up,55.3%reachedthe sameorevenabetterParkerscore.MeanVASatfollow-upwas0.9. All patients were osteoporotic, whereas the mean cortical thickness index (CTI AP) was0.47. In 33.9%, thepostoperative X-rays showedan anatomicreduction. In 57.6%, reduction was near-anatomicandnon-anatomicin8.5%.Anopenreductionwas necessary inthree cases,whereas in two casessubtrochanteric cerclage wires were used to stabilise the reduction without removal.In61%,thebladecouldbeplacedinanidealposition,that is,centre–centreofthehead(Fig.4).Therewasonepatientwitha postoperativebleedingandonewitharotationaldeformity,both necessitatingare-operation.
Theonlyintra-operativecomplicationreportedwasa perfora-tionofthek-wireintothehipjoint.Itwasdetectedbyinstillingthe contrastmedium(Fig.3(b)).Consequently,nocement augmenta-tionwasperformedinthispatient.Forthepresentedstudy,cement applicationwasratedas‘‘good’’or‘‘excellent’’in84.7%.
In two cases, the augmented PFNA was used as a salvage procedureinfailurecases.Onewasafailedgammanailwith lag-screwlooseninginanA3fracture.Inthiscase,thegammanailwas removed 6 weeks after implantation and an augmented PFNA procedure was performed without complications. Follow-up examinationafter4monthsshowedfractureunionwithoutany further problems(Fig.7). The othercase wasa malreducedA3 fracture,wherethePFNAwasinsertedatawrongentrypointand poorlypositioned.Inthissecondcase,animpendingcut-outwas intended to be avoided with thestandardised augmentation 2 weeksaftertheprimarysurgicalintervention.Unfortunately,the patientdiedafter6weeksduetoapre-existingrenalinsufficiency. Follow-up4weeksaftertherevisionsurgeryshowednofurther dislocationapartfromalateralblademigration.
A mean of 4.2ml of cement was injected and the cement distributionaroundthebladewasalmosthomogeneous(Table2).
Fig.6.ThemethodofmeasuringthecementdistributionaroundthebladeintheAP viewwhereasameansthesuperior,bthecentralandctheinferiorfractionofthe cement.
Table1
Thebaselinecharacteristicsofthestudypopulation.
All(n=59) Percent
Age,mean 84,5
Female/male 45/14 76.3/23.7
Left/right 29/30 49.2/50.8
AO31-A1 15 25.4
AO31-A2 31 52.5
AO31-A3 13 22
Hospitalisationtime,mean 12.5days Fig.5.Thepositionofthebladewithinthefemoralhead.
C.Kammerlanderetal./Injury,Int.J.CareInjuredxxx(2011)xxx–xxx 4
G Model
Only a severeosteoporosis is predictive for central(area ‘b’ in
Fig.6)cementflowtowardsthehipjoint(p<0.05).
Atfollow-up,allfracturesshowedacallusformation.Wecould notdetectanysignofosteonecrosisofthefemoralheadorlysis around the cement. According to the above-mentioned meth-od,35,36 there was no implant migration (e.g.,migration of the bladerelatedtothefemoralhead)measurableasidefromlateral blade migration. We did not find any cut-out, cut through, unexpected blade migration, implant loosening or implant breakagewithinthestudyperiod.
Discussion
ThePFNAwasprovedtobeastableimplantforthetreatmentof proximalfemoralfractures.7–9,37Nevertheless,thereare
compli-cationssuchascuttingoutofthefemoralheadorbladeloosening reported in the literature.7–9 All these complications are cata-strophic failures for these patients due to the necessity of re-operation.Asmostofthesefracturesoccurintheelderly,these failuresareevenmoresevereduetothepatients’co-morbidities andtheirinabilitytocounterbalance,whichcomesalongwitha highperioperativemorbidityandmortality.
Thesurgicalcomplicationrateinthepresentedstudywas3.4%, withnocomplicationrelatedtothecementaugmentation.Thisis anacceptableratecomparedwithotherreportsintheliterature.8,9
Wedidnotfindanycut-outorcuttingthroughoftheblade, unexpectedblademigrationandlooseningoftheblade. Implant-related complications in proximal femoral fractures needing revision surgery, suchas a cut-out of the implant throughthe femoral head,arereportedtobeashighas16%.2,10,38,39Recent findingsdealingonlywiththePFNAreportaboutacut-outrateof 2%8and3.6%.7Wedidnotfindanycut-outorcuttingthroughofthe
blade, unexpected blade migration and loosening of the blade. Therefore,ourfindingsmakeusbelievethatanadditionalcement augmentationcanavoidacut-outinthesefractures;butithasto benotedthatourseriesispossiblytoosmalltoconcludethis.
Fig.7.(a)Thegammanailfailedinthisunstablepertrochantericfracture6weeksaftersurgery.(b)APFNAwithstandardizedcementaugmentationthroughtheperforated bladewasusedasasalvageprocedure.Thefracturehealedwithoutanyproblemwithin4months.
Table2
Thecementdistributioninallpredefineddirectionsinpercent.Therightpart showsthecorrelation(p-value)withthecorticalthicknessindexinbothstandard views.
CTIAP CTIAX
CementdistributionAP
Cranial 44.1 0.992 0.400
Caudal 43.1 0.096 0.061
Central 12.8 0.387 0.078
CementdistributionAX
Ventral 43.1 0.374 0.127
Dorsal 44.8 0.079 0.089
Postoperatively, we observed one case of a fall-related additionalfemoralfractureatthetipofthenail.Inthiscase,the shortnailwaschangedtoalongnailandboththeremovalandthe new implantation of the blade was performed without any problem. Theblade–PMMA interface brokeand there werenot more force needed to remove the blade. The new blade was inserted in the same position and there was no additional augmentationdone.Unfortunately,thepatientdied4weeksafter thesecondoperationduetomyocardialinfarction.
In ourstudy,55.3%reachedtheirprefracturefunctionallevel withinthestudyperiod.Inthiscontext,wehavetonotethatthe mean age of our study population was 84.5 years and these patientshavemanyco-morbidconditions.40–43These
co-morbid-itiesinfluencetherecoveryofthepatients41andcomparedwith
theliterature,7–9thisisasatisfyingoutcome.
AccordingtocorticalthicknessmeasurementsproposedbySah et al.,34 all our patients suffered from osteoporosis. We have
observed that the distribution of the cement was almost homogeneous.However,itwasnotpossibletoguidethecement intoapredeterminedareawiththeusedside-openingcannula.A mean amount of 4.2ml cement was used to augment the perforatedblade.Thedistributionofthecementwasinfluenced onlyincaseswithsevereosteoporosisinthewaythatwecould observeahigherfractioncentralofthetipofthebladetowardsthe hipjoint.Ithastobenoticedthatasubchondralpresenceofthe PMMAcouldpossiblyinfluencetheoverlyingcartilage.44Wedid
notfindanycorrelationwiththeamountofinjectedcementand pain or mobility at follow-up. Due to an exothermic reaction duringPMMA cementpolymerisation, itis suspected thatlocal bonedamagemaybeinduced.24Inourseries,wedidnotfindany
radiologicalsignsofbonenecrosis.Thissupportsthetheorythat thereisno thermal damagetothebone duetotheexothermic reactionofthePMMAinastandardisedaugmentationsettingwith onlya smallamountofcementinjected.26,28Themean cement
volumeof4.2mlusedinourstudywasabletoincreasestabilityin biomechanicalinvestigations.14,20,23,26However, withthis small
amountofcementdamagetotheboneisunlikely.14Inthiscontext,
ithastobementionedthatourfollow-uptimecouldbetooshort forastatementaboutbonenecrosis,asseveralauthorsreportthe timetoonsetupto3yearsafterthefracture.45,46Withinthestudy
period,allfractureswerehealedandwedidnotfindany bone-healingdisturbance.Therefore,westatethatthenewstandardised techniqueisasafemethodcomparedwithotherpublishedcement augmentationtechniques.10,16–21,47
Themainlimitationsofthis studywerethelackofacontrol group and the inclusion of stable pertrochanteric fractures. However, thefeasibility ofthe newstandardisedaugmentation wasproved.Theindicationfortheaugmentationisnotclearyet andwesupporttheopinionthatthegoodresultswiththePFNAin previousstudiesresultfromachievingagoodfracturereduction and careful implant placement.7,8,48 We think that a severe
osteoporosiscouldbeapossibleindicationbutthereareprobably moreconcomitantpatient-relatedfactorstobeconsidered.From thesocioeconomicperspectivealso,additional costshavetobe mentioned. An analysis of failure cases and a prospective, randomised trial comparing geriatric patients with unstable pertrochanteric fractures with a PFNA either with or without augmentation would probably give us more hints to find the patientsatriskandtodefinetheindicationsforaugmentation.
Conclusion
ThestandardisedaugmentationoftheperforatedPFNAbladeis asafeanduser-friendlytoolforpertrochantericfracturefixation.It prevents blade migration within the head–neck fragment and leads to good functional results. These impressions should be
proven by a randomised trial comparing the PFNA with and withoutaugmentation.
Conflictofinterest
Noneoftheauthorshasanyfinancialorpersonalrelationship withorganisationsthatcouldinfluencetheirworkinappropriately.
Acknowledgements
Synthesisacknowledgedfororganisationalsupport.Therewas no involvement of Synthes in study planning, data analysis, interpretationorarticlewriting.Theauthorswouldliketothank Dr.Alexander Scolaforhelpingwithdata managementand Dr. StefanieErhartforherhelpwithpreparationofthearticle.
References
1.SaudanM,LubbekeA,SadowskiC,RiandN,SternR,HoffmeyerP. Pertrochan-tericfractures:isthereanadvantagetoanintramedullarynail?Arandomized, prospective studyof206 patientscomparing thedynamichipscrewand proximalfemoralnail.JOrthopTrauma2002;16(6):386–93.
2.AnglenJO,WeinsteinJN.Nailorplatefixationofintertrochanterichipfractures: changingpatternofpractice.AreviewoftheAmericanBoardofOrthopaedic SurgeryDatabase.JBoneJointSurgAm2008;90(4):700–7.
3.AhrengartL,To¨rnkvistH,FornanderP,ThorngrenK-G,PasanenL,Wahlstro¨mP, etal.ArandomizedstudyofthecompressionhipscrewandGammanailin426 fractures.ClinOrthopRelatRes2002;(401):209–22.
4.MadsenJE,NaessL,AuneAK,AlhoA,EkelandA,StromsoeK.Dynamichipscrew with trochanteric stabilizingplate inthe treatment ofunstable proximal femoralfractures:acomparativestudywiththeGammanailandcompression hipscrew.JOrthopTrauma1998;12(4):241–8.
5.PervezH,ParkerMJ,VowlerS.Predictionoffixationfailureafterslidinghip screwfixation.Injury2004;35(10):994–8.
6.VidyadharaS,RaoSK.Oneandtwofemoralneckscrewswithintramedullary nailsforunstabletrochantericfracturesoffemurintheelderly–randomised clinicaltrial.Injury2007;38(7):806–14.
7.MereddyP,KamathS,RamakrishnanM,MalikH,DonnachieN.TheAO/ASIF proximalfemoralnailantirotation(PFNA):anewdesignforthetreatmentof unstableproximalfemoralfractures.Injury2009;40(4):428–32.
8.SimmermacherRK,LjungqvistJ,BailH,HockertzT,VochtelooAJ,OchsU,etal. Thenewproximalfemoralnailantirotation(PFNA)indailypractice:resultsofa multicentreclinicalstudy.Injury2008;39(8):932–9.
9.LiuY,TaoR,LiuF,WangY,ZhouZ,CaoY,etal.Mid-termoutcomesafter intramedullaryfixationofperitrochantericfemoralfracturesusingthenew proximalfemoralnailantirotation(PFNA).Injury2010;41(8):810–7. 10.MattssonP,LarssonS.Unstabletrochantericfracturesaugmentedwithcalcium
phosphatecement.Aprospectiverandomizedstudyusingradiostereometryto measurefracturestability.ScandJSurg2004;93(3):223–8.
11.Mattsson P,LarssonS.Stabilityofinternallyfixedfemoralneck fractures augmentedwithresorbablecement.Aprospectiverandomizedstudyusing radiostereometry.ScandJSurg2003;92(3):215–9.
12.BonnaireF,WeberA,Bo¨slO,EckhardtC,SchwiegerK,LinkeB.‘‘Cuttingout’’bei pertrochanta¨renFrakturen–einProblemderOsteoporose?DerUnfallchirurg 2007;110(5):425–32.
13.StoffelKK,LeysT,DamenN,NichollsRL,KusterMS.Anewtechniqueforcement augmentationoftheslidinghipscrewinproximalfemurfractures.ClinBiomech (BristolAvon)2008;23(1):45–51.
14.vonderLindenP,GisepA,BonerV,WindolfM,AppeltA,SuhmN.Biomechanical evaluationofanewaugmentationmethodforenhancedscrewfixationin osteoporoticproximalfemoralfractures.JOrthopRes2006;24(12):2230–7. 15.SzpalskiM,DescampsP-Y,HayezJ-P,RaadE,GunzburgR,KellerTS,etal.
Preventionofhiplagscrewcut-outbycementaugmentation:descriptionofa newtechniqueandpreliminaryclinicalresults.JOrthopTrauma2004;18(1): 34–40.
16.Dall’OcaC,MalutaT,MoscoloA,LaviniF,BartolozziP.Cementaugmentationof intertrochanteric fractures stabilised with intramedullary nailing. Injury 2010;41(11):1150–5.
17.HarringtonKD.Theuseofmethylmethacrylateasanadjunctintheinternal fixationofunstablecomminutedintertrochantericfracturesinosteoporotic patients.JBoneJointSurgAm1975;57(6):744–50.
18.SchatzkerJ,Ha’eriGB,ChapmanM.Methylmethacrylateasanadjunctinthe internalfixationofintertrochantericfracturesofthefemur.JTrauma1978;18(10): 732–5.
19.MuhrG,TscherneH,ThomasR.Comminutedtrochantericfemoralfracturesin geriatricpatients:theresultsof231casestreatedwithinternalfixationand acryliccement.ClinOrthopRelatRes1979;(138):41–4.
20.MattssonP,AlbertsA,DahlbergG,SohlmanM,HyldahlHC,LarssonS. Resorb-ablecementfortheaugmentationofinternally-fixedunstabletrochanteric fractures.Aprospective,randomisedmulticentrestudy.JBoneJointSurgBr 2005;87(9):1203–9.
C.Kammerlanderetal./Injury,Int.J.CareInjuredxxx(2011)xxx–xxx 6
G Model
21.BartucciEJ,GonzalezMH,CoopermanDR,FreedbergHI,BarmadaR,LarosGS. Theeffectofadjunctivemethylmethacrylateonfailuresoffixationandfunction inpatientswithintertrochantericfracturesandosteoporosis.JBoneJointSurg Am1985;67(7):1094–107.
22.KammerlanderC,BlauthM,RothT.Re:cementaugmentationof intertrochan-tericfracturesstabilisedwithintramedullary,inpress.
23.LindnerT,KanakarisNK,MarxB,CockbainA,KontakisG, GiannoudisPV. Fracturesofthehipandosteoporosis:theroleofbonesubstitutes.JBoneJoint SurgBr2009;91(3):294–303.
24.HeiniPF,FranzT,FankhauserC,GasserB,GanzR.Femoroplasty-augmentation ofmechanicalpropertiesintheosteoporoticproximalfemur:abiomechanical investigationofPMMAreinforcementincadaverbones.ClinBiomech(Bristol Avon)2004;19(5):506–12.
25.vonSteyernFV,KristianssonI,JonssonK,MannfolkP,HeinegardD,RydholmA. Giant-celltumouroftheknee:theconditionofthecartilageaftertreatmentby curettageandcementing.JBoneJointSurgBr2007;89(3):361–5.
26.BonerV,KuhnP,MendelT,GisepA.TemperatureevaluationduringPMMA screwaugmentationinosteoporoticbone–aninvitrostudyabouttheriskof thermalnecrosisinhumanfemoralheads.JBiomedMaterResBApplBiomater 2009;90(2):842–8.
27.UnsalM,TetikC,ErolB,CabukogluC.Theinjectionofacrylicbonecement preventsbone collapsein the intercalarbones lacking bonysupport: an experimental sheep semilunar bone model. Acta Orthop Traumatol Turc 2003;37(1):63–9.
28.WelchRD,BerryBH,CrawfordK,ZhangH,ZobitzM,BronsonD,etal.Subchondral defectsincaprinefemoraaugmentedwithinsitusettinghydroxyapatitecement, polymethylmethacrylate,orautogenousbonegraft:biomechanicaland histo-morphologicalanalysisaftertwo-years.JOrthopRes2002;20(3):464–72. 29.OkenMM,CreechRH,TormeyDC,HortonJ,DavisTE,McFaddenET,etal.
ToxicityandresponsecriteriaoftheEasternCooperativeOncologyGroup.AmJ ClinOncol1982;5(6):649–55.
30.ParkerMJ,PalmerCR.Anewmobilityscoreforpredictingmortalityafterhip fracture.JBoneJointSurgBr1993;75(5):797–8.
31.CarlssonAM.Assessmentofchronic pain.I. Aspectsofthereliabilityand validityofthevisualanaloguescale.Pain1983;16(1):87–101.
32.BryantDM,SandersDW,ColesCP,PetrisorBA,JerayKJ,LaflammeGY.Selection of outcome measures for patients with hip fracture. J Orthop Trauma 2009;23(6):434–41.
33.DorrLD,FaugereMC,MackelAM,GruenTA,BognarB,MallucheHH.Structural andcellularassessmentofbonequalityofproximalfemur.Bone1993;14(3): 231–42.
34.SahAP,ThornhillTS,LeboffMS,GlowackiJ.Correlationofplainradiographic indices ofthe hipwith quantitativebonemineraldensity. Osteoporos Int 2007;18(8):1119–26.
35.WatanabeY,MinamiG,TakeshitaH,FujiiT,TakaiS,HirasawaY.Migrationof thelagscrewwithinthefemoralhead:acomparisonoftheintramedullaryhip screwandtheGammaAsia-Pacificnail.JOrthopTrauma2002;16(2):104–7. 36.GardnerMJ,BriggsSM,KopjarB,HelfetDL,LorichDG.Radiographicoutcomes
ofintertrochanterichipfracturestreatedwiththetrochantericfixationnail. Injury2007;38(10):1189–96.
37.Lenich A,Vester H,Nerlich M,MayrE, StockleU, Fuchtmeier B. Clinical comparisonofthesecondandthirdgenerationofintramedullarydevicesfor trochantericfracturesofthehip–bladevsscrew.Injury2010;41(12):1292–6. 38.ParkerMJ.Valgusreductionoftrochantericfractures.Injury1993;24(5):313–6. 39.SimpsonAH,VartyK,DoddCA.Slidinghipscrews:modesoffailure.Injury
1989;20(4):227–31.
40.DoneganDJ,GayAN,BaldwinK,MoralesEE,EsterhaiJrJL,MehtaS.Useof medicalcomorbiditiestopredictcomplicationsafterhipfracturesurgeryinthe elderly.JBoneJointSurgAm2010;92(4):807–13.
41.RocheJJ,WennRT,SahotaO,MoranCG.Effectofcomorbiditiesand postopera-tivecomplicationsonmortalityafterhipfractureinelderlypeople:prospective observationalcohortstudy.BMJ2005;331(7529):1374.
42.KammerlanderC,RothT,FriedmanSM,SuhmN,LugerTJ, Kammerlander-KnauerU,etal.Ortho-geriatricservice–aliteraturereviewcomparingdifferent models.OsteoporosInt2010;21(Suppl.4):S637–46.
43.RothT,KammerlanderC,GoschM,LugerTJ,BlauthM.Outcomeingeriatric fracturepatientsandhowitcanbeimproved.OsteoporosInt2010;21(Suppl. 4):S615–9.
44.HisatomeT,YasunagaY,IkutaY,FujimotoY.Effectsonarticularcartilageof subchondralreplacementwith polymethylmethacrylateandcalcium phos-phatecement.JBiomedMaterRes2002;59(3):490–8.
45.BarnesR,BrownJT,GardenRS,NicollEA.Subcapitalfracturesofthefemur.A prospectivereview.JBoneJointSurgBr1976;58(1):2–24.
46.LoizouCL,ParkerMJ.Avascularnecrosisafterinternalfixationofintracapsular hipfractures;astudyoftheoutcomefor1023patients.Injury2009;40(11): 1143–6.
47.Szpalski M,Descamps PY,Hayez JP,RaadE, GunzburgR, KellerTS,et al. Preventionofhiplagscrewcut-outbycementaugmentation:descriptionof anewtechniqueandpreliminaryclinicalresults.JOrthopTrauma2004;18(1): 34–40.