Effects of Ascaris lumbricoides in eosinophils, regulatory B cells and asthma severity in asthmatic patients from a helminth endemic population
47
0
0
Texto completo
(2) Content Abstract ............................................................................................................................................... 3 Introduction ........................................................................................................................................ 4 Materials and Methods ....................................................................................................................... 6 Study Population ............................................................................................................................. 6 Eligibility Criteria ............................................................................................................................. 6 Study procedures ............................................................................................................................ 7 Skin Prick Test.............................................................................................................................. 7 Assessment of lung function ....................................................................................................... 7 Serum total and allergen-specific IgE and complete blood count .............................................. 8 Stool samples and parasitological examination .......................................................................... 8 Human B cell isolation and characterization............................................................................... 9 Statistical Analysis ........................................................................................................................... 9 Main Objective .................................................................................................................................. 10 Secondary Objectives .................................................................................................................... 10 Results ............................................................................................................................................... 11 Discussion .......................................................................................................................................... 29 Conclusion ......................................................................................................................................... 34 Funding source .................................................................................................................................. 34 Conflicts of interest ........................................................................................................................... 34 Acknowledgements ........................................................................................................................... 35 REFERENCES ...................................................................................................................................... 35 Supplementary Material 1 ................................................................................................................ 39 Supplementary Material 2 ................................................................................................................ 46. 2.
(3) Abstract Background: Helminth infections can modify the immune response of the host and exert risk and protective effects on allergic diseases depending on the chronicity and intensity of the infection. Blood populations such as eosinophils and regulatory B cells have been independently associated with helminth infection and allergic diseases, with eosinophils being used as biomarkers for severity. However, the effects of helminth infections in these blood populations, and the predictive role of eosinophils in asthma severity is unclear in humans from endemic settings. Objectives: To characterize the effects of Ascaris lumbricoides infection in eosinophils, regulatory B cells and asthma severity in asthmatic patients from a helminth endemic population. Methods: In a rural community from the Colombia tropics, asthmatic patients were recruited and evaluated with a clinical questionnaire, specific and total IgE, complete blood counts, skin prick test, serial coprologicals and spirometry. Regulatory B cell subsets were evaluated in a subset of asthmatic patients and controls from the community. Results: A total of 82 patients with wheezing symptoms in the last year were recruited. Complete blood counts showed a mean eosinophil count of 654 (±SD 634) cells/uL, with 48,7% (n=40) of patients having eosinophils greater than 400 cells/uL. The frequency of active A.lumbricoides and T.trichiura infection were 46,3% (n=38) and 18,2% (n=15) respectively. In the multivariate analysis, A.lumbricoides sensitization was associated with a 6.9-fold increase in the odds of having eosinophils greater than 400 cells/uL (p=0.002) and House Dust Mite (HDM) sensitization was also associated with a 5,4-fold increase (p=0.008). Helminth infection was associated with higher log-transformed eosinophils independently of age and HDM sensitization.We found lower percentage of CD24+CD38+ B cells in asthmatic patients compared to control subjects and no significant differences between infected and uninfected patients for CD1dhighCD5+ and CD24highCD38high B cell subsets. Conclusion: In a rural community from the Colombian tropics, where helminths are endemic, sensitization to A.lumbricoides was more predictive of eosinophilia than sensitization to house dust mites. The frequency of regulatory B cell subsets was lower in asthmatic patients than in controls. Further research should evaluate larger cohorts and determine the basal level of eosinophils in this population and focus on the cellular function of regulatory B cells.. 3.
(4) Introduction. Helminths are a group of invertebrate parasites that are capable of living inside their host for a great number of years. Although thorough epidemiological studies are lacking in high income countries 1 , helminths have been considered eradicated in these countries, whereas in middle and low-income countries, theses parasites are still a significant cause of morbidity, affecting around 2 billion people, mainly children 2. Indeed, they even have been referred to as “the great neglected tropical diseases”, since their global burden of disease surpasses better-known conditions, such as malaria and tuberculosis 3. Their ubiquity in human evolution has made them a major selective force in the genetics of immune response 4. As such, the immune response to helminths can vary from immunosuppression to increase susceptibility to allergic and autoimmune diseases, depending on the chronicity and intensity of the infection, but also on host’s genetics factors and helminth species 5–8. In terms of allergic diseases, in settings where helminth infections are endemic but low intensity, these infections have been associated with asthma presentation and its severity, which could be explained by the strong Th2 response induced, but also by cross reactivity between helminth and house dust mite allergens 9,10. Indeed, a recent study conducted by our group in a rural tropical village found that ascariasis exerts risk and protective effects on asthma symptoms, depending on the severity of the infection 8,10.. 4.
(5) In non or scarcely infected populations, total IgE and blood eosinophils are associated with the Th2 response in asthmatic patients and can even be used as markers of severity 11,12. In fact, new biological therapies, such as mepolizumab, reslizumab or benralizumab, target eosinophils and their prescription is dependent on the absolute count of eosinophils for severe asthma 13,14. However, the predictive value of these biomarkers hasn´t been studied in endemic settings for Ascaris lumbricoides infections. Conversely, allergic responses are characterized by the lack of tolerance to allergen exposure, and recent efforts have demonstrated that the generation of immunoregulatory cell populations, such as regulatory T and B cells (Tregs and Bregs), is central to allergen tolerance induction 15,16. For example, in asthmatic patients, Bregs CD24hiCD27+ are reduced in number and produce less IL-10 in response to LPS, compared to healthy controls 17. In mice, helminth infections, or even its egg antigens, can also induce the generation of Bregs which in turn suppress allergic airway inflammation 18–23. So far, no information is available on the frequency of regulatory B cells in Ascaris lumbricoides endemic regions. Therefore, in this study we sought to investigate the association between eosinophils, regulatory B cells and exacerbations and indicators of asthma severity, as well as the factors that determine eosinophilia in a rural population of asthmatic patients from the Colombian tropics.. 5.
(6) Materials and Methods Study Population This study was conducted in the rural community of Santa Catalina, a small tropical farming/fishing town at the North of Colombia that includes five villages (153 km2, 12.500 inhabitants, no sewage, and low socioeconomically strata). Our group recently conducted a cross sectional survey using a validated ISAAC questionnaire to determine the prevalence of asthma and allergic rhinitis in a population-representative sample of 739 subjects selected by stratified random sampling, and parasitological evaluation by Kato Katz method in 694 patients. We found an age and gender-adjusted prevalence of asthma and rhinitis symptoms in the last year was 14.6% and 34.1%, respectively (N = 739). By stool exam, ascariasis and trichuriasis were 62.5% and 35.7%, respectively 24.. Eligibility Criteria The patients from this study were asthmatic patients recruited from the previous prevalence study, as well as patients referred from the local health centers and public high schools. Eligibility criteria were: subjects in the age range of 3 to 70 years with a clinical history of asthma exacerbations or wheezing in the previous 12 months. Eligible subjects were further interviewed and asthma diagnosis was confirmed in those with at least two respiratory. symptoms. (cough,. wheezing,. dyspnea,. and. nocturnal. cough/wheezing/dyspnea) or a history of recurrent asthma attacks. These questions were done by staff physicians following a validated questionnaire. 25. . All the participants in the. 6.
(7) study signed an informed consent. Written parental consent was obtained for participating children, for whom written assent was also obtained (Supplementary Material 1) .The study was approved by the Institutional Review Board of the Universidad de Cartagena (Cartagena, Colombia). This work was funded by the Colombian government (Colciencias, Grant 590-2013) and the University of Cartagena. The principal investigator was Dr Luis Caraballo.. Study procedures Study participants completed a protocol that included a medical and sociodemographic questionnaire, complete blood count, skin prick test, measurement of serum total and allergen-specific IgE, spirometry (in patients older than 7 years old), and two serial stool samples for parasitological examination. Skin Prick Test Skin prick test (SPT) was done in the forearm with a battery of allergen extracts including: D. pteronyssinus, Ascaris extract, histamine phosphate 10 mg/mL as positive control and allergen diluent as negative control. The test was considered positive if the mean diameter of the wheal at 15 minutes was > 3 mm. Assessment of lung function Spirometry was performed in the patient’s (>7 years old) household with a portable spirometer (Care Fusion, Vyaire Medical) following the American Thoracic Society recommendations 26. Height and weight were measured; patients were instructed to avoid use of short-acting bronchodilators for at least 12 hours before testing. The best forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) were selected for data analysis of FEV1 and FEV1/FVC ratio. To evaluate bronchodilator responsiveness (BDR), 7.
(8) spirometry was performed before and 15 minutes after receiving 400 μg (4 puffs) of inhaled salbutamol.. Serum total and allergen-specific IgE and complete blood count Serum total IgE and specific IgE levels against B. tropicalis, D. pteronyssinus, and A. lumbricoides were determined by ImmunoCap system (Phadia100, Thermo, Sweden). A cutoff value of 0.35 kU/L was used to consider a test as positive. Atopy was defined as the presence of at least one sIgE to House Dust mite ≥0.35 kU/L irrespective of SPT results. Complete blood count was taken from 4 ml of peripheral venous blood, in an EDTA tube, and transported in 4 °C containers to Cartagena for its analysis. Parameters analyzed included Hemoglobin (g/dL), Hematocrit (%), Mean Corpuscular Volume (fL), mean corpuscular hemoglobin (pg), absolute leucocyte populations and platelets. Stool samples and parasitological examination Parasitological analyses were done using 0.85% saline solution and lugol staining; counting helminth eggs were done by the Kato Katz method using a commercial kit (Copro Kit, C&M Medical, Campinas, Brazil). The results were expressed as egg per gram of feces (e.p.g.). The presence of eggs from geohelminths or parasite visualization was considered diagnostics of active infection. Two serial stool samples were collected to improve the sensitivity of the exam, and questions regarding previous helminth expulsion were included in the questionnaire.. 8.
(9) Human B cell isolation and characterization PBMCs were isolated by Ficoll-Histopaque (Sigma Aldrich, Ref 10771) density gradient centrifugation from 30 ml of heparinized blood. Briefly, 30 mL of peripheral venous blood were extracted in heparin tubes. The samples were diluted in a 1:1:1 gradient with PBS (phosphate buffer saline) and Ficoll Histopaque for 20 minutes in 800g, then washed twice with 25 mL PBS/EDTA and then resuspended in 1 mL of RPMI (Sigma Aldrich, Ref 8758) and 1 mL of freezing medium (80% Inactivated fetal Bovine Serum, and 20% Dimethyl sulfoxide). The samples were stored in 2 mL cryovials and refrigerated at -70 °C with a Mr. Frosty™ Freezing Container (Thermo Scientific™). For Breg characterization, the cells were unfrozen in bain-marie at 38 °C ,washed twice with complete RPMI and centrifuged for 10 minutes at 300g. The cells were then washed twice with Stain Buffer (FBS) (BD, Biosciences, Ref 554657) and centrifuged at 300g for 5 minutes at 4 °C. The cells were then stained for CD5-FITC (L17F12, eBioscience), CD1d-PE (CD1d42, BD Biosciences), CD24-FITC (ML5, BD Biosciences), CD38-PECy7 (HIT2, eBioscience), CD19BV510 (SJ25C1, BD Biosciences) and CD3-APC (OKT3, eBioscience) in order to characterize Breg subsets CD24+CD38+CD19+CD3- y CD5+CD1d+CD19+CD3-. The cells were incubated for 30 minutes and then stained with 7-AAD (00-6993-50, eBioscience) for cell viability. Flow cytometry was done using FACS Aria III (BD Biosciences) and the data was analyzed with FlowJo v10.. Statistical Analysis The analyses were done using SPSS version 13.0 (Chicago, IL, USA). Frequency rates and their 95% confidence intervals (CI) were obtained with Epidat 3.1 (Xunta de Galicia, PAO/WHO). Bivariate analyses were conducted by Pearson chi-squared test (or Fisher exact 9.
(10) test when appropriate) for categorical variables and 2-tailed t tests for categorical and continuous variables. Univariate and multivariate binary logistic regression were conducted to determine predictor variables for Eosinophils > 400 cells/uL. Predictor variables in the univariate analysis included, House Dust Mite sensitization, Ascaris sensitization, Active Ascaris or Trichuris infection, helminth coinfection, allergic rhinitis, age and gender. In the multivariate analysis, significant variables at P < 0.1 were analyzed, and adjusted for age, gender and coinfection status. Log transformed eosinophils were analyzed by generalized linear model to identify the predictive value of specific IgE and helminth infection and eosinophilia, and analyzed with R statistical software.. Main Objective To characterize the effects of Ascaris lumbricoides infection in blood eosinophils, regulatory B cells and asthma severity in asthmatic patients from a helminth endemic population.. Secondary Objectives 1. Conduct a sociodemographic and clinical characterization of a sample of asthmatic patients living in the rural community of Santa Catalina 2. Evaluate the association between Ascaris lumbricoides infection and asthma exacerbations and indicators of severity in the last 12 months. 3. To determine the effect of the frequency of regulatory B cell subsets and clinical indicator of asthma severity 4. To determine the predictive value of eosinophils in asthma exacerbations and asthma severity. 5. Compare the frequency of regulatory B cell subsets between asthmatic patients and non-atopic controls.. 10.
(11) 6. To determine the association between anemia and Ascaris lumbricoides infection and egg counts.. Results Baseline characteristics of the study population are shown in Table 1. A total of 82 patients with wheezing symptoms in the last year were recruited; asthmatic adults or wheezing children were recruited for the study. Mean age was 20,2 years old (± SD 18,1), with a slight female predominance of 59,7% (n=49). In terms of allergic comorbidities, 79,2% (n=65) had allergic rhinitis and 7,3% (n=6) and atopic dermatitis. Moreover, 64.6% of patients reported at least one ER visit due to asthma exacerbations in the last 12 months and 21,9% required inpatient care in the last 12 months. Complete blood counts showed a mean eosinophil count of 654 (±SD 634) cells/uL, with 48,7% (n=40) of patients having eosinophils greater than 400 cells/uL. Mean hemoglobin levels (g/dL) were 12,21 (± 1,5); 22% (n=18) fulfilled the criteria for anemia according to the WHO standards 27. The frequency of active Ascaris infection was 46,3% (n=38) with a mean egg count of 2,726 (±13,151) eggs per gram. The frequencies of active T.trichiura and G.lamblia were lower, with 18, 2% (n=15) and 7% (n=6), respectively. In addition, almost all of the patients with active T.trichiura were also coinfected with Ascaris (n=14). In terms of IgE sensitization, A.lumbricoides, B.tropicalis and D. pteronyssinus sensitization frequencies were high, with 62,3% (n=48), 61% (n=47), and 40,3% (n=31), respectively.. 11.
(12) Association between Ascaris lumbricoides infection. and asthma exacerbations and. indicators of asthma severity. Associations between Ascaris lumbricoides infection and indicators of asthma severity, including exacerbations, are shown in Table 2. No significant associations were found among active A. lumbricoides infection, Ascaris sensitization (defined by a positive specific IgE or skin prick test result) and asthma exacerbations or indicators of asthma severity such as emergency room visit or hospitalizations in the last 12 months. However, we did find a statistically significant association between moderatesevere Ascariasis (> 4000 eggs per gram) and more than 4 ER visits in the last 12 months, and a trend towards significance with moderate-severe Ascariasis and more than 4 exacerbations in the last 12 months. Association between blood eosinophilia and asthma exacerbations and indicators of asthma severity. Since blood eosinophils and eosinophilia >400 cells/uL are predictors for asthma severity, we sought to determine if this blood cell population is still associated with asthma exacerbations in a rural population endemic for Ascaris lumbricoides, and to explore the factors that drive blood eosinophils. Eosinophils >400 cells/uL were associated with ER visits in the previous 12 months (p=0.017) (Table 3). However, when adjusted by age and gender, ER visits in the previous 12 months is no longer significant, indicating that younger patients attend more to the emergency room. No associations were found between eosinophils >75th percentile and asthma exacerbations (data not shown). Variables associated with blood eosinophils. A.lumbricoides and B.tropicalis sensitization were associated with Eosinophils >400 cells/uL (p=0.009) (Table 5), and A.lumbricoides infection and sensitization, T.trichuria infection, and coinfection with both helminths was 12.
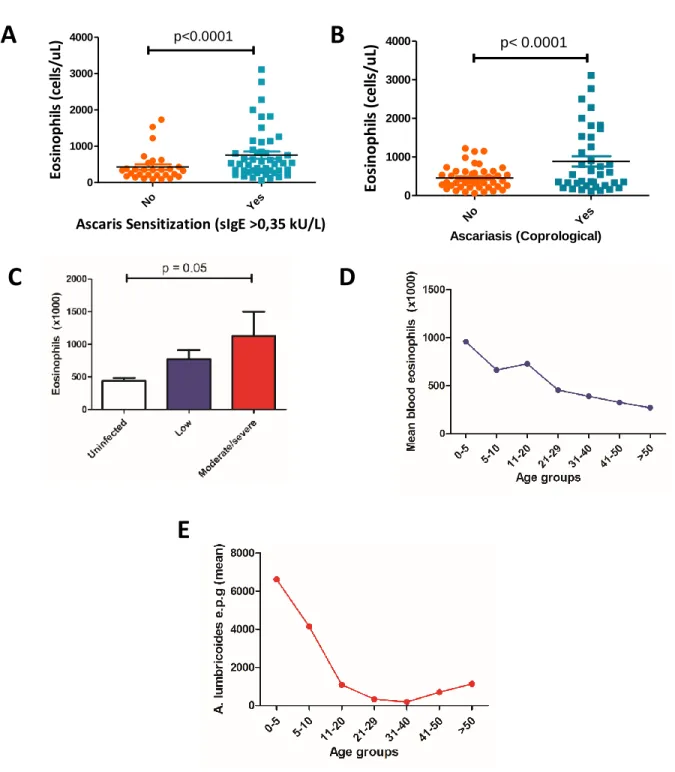
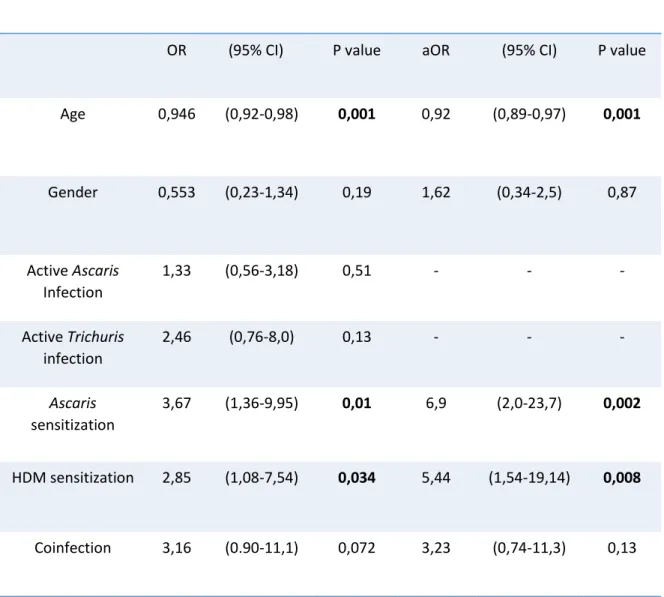
(13) significantly associated with Eosinophils greater than the 75th percentile (p <0,05) (Table 6). In addition, when eosinophils are examined as a continuous variable, both Ascaris sensitization and active infection were significantly associated with greater mean eosinophil counts (p<0,0001) (Figure 1a and 1b). Moreover, there was a dose-dependent relationship between greater parasite burdens (moderate/severe vs Low egg counts vs uninfected) and higher mean blood eosinophils (Figure 1c). Mean blood eosinophils and mean Ascaris egg counts were both highly dependent on age, as the age groups from 0-5 and 5-10 years old exhibited higher mean eosinophils (Figure 1d). Logistic regression for Eosinophils greater than 400 cells/uL and log-transformed eosinophils We conducted a univariate and multivariate logistic regression to evaluate variables associated with Eosinophils greater than 400 cells/uL. In the univariate analysis, age (OR=0,94; p=0,001), A.lumbricoides sensitization (OR=3.67; p=0,01) and HDM sensitization (OR=2,85; p=0,034 ) were significantly associated with eosinophils greater than 400 cells/uL. In the multivariate analysis, after adjustment for age and gender, A.lumbricoides sensitization was associated with a 6.9-fold increase in the odds of having eosinophils greater than 400 cells/uL (p=0.002) and HDM sensitization was also associated with a 5,4fold increase (p=0.008) (Table 7). Moreover, as a continuous variable, log-transformed eosinophil numbers were higher in A. lumbricoides infected subjects and inversely associated to age (Table 8). Adjustment by B. tropicalis specific IgE levels or D. pteronyssinus levels did not affect significance of the. 13.
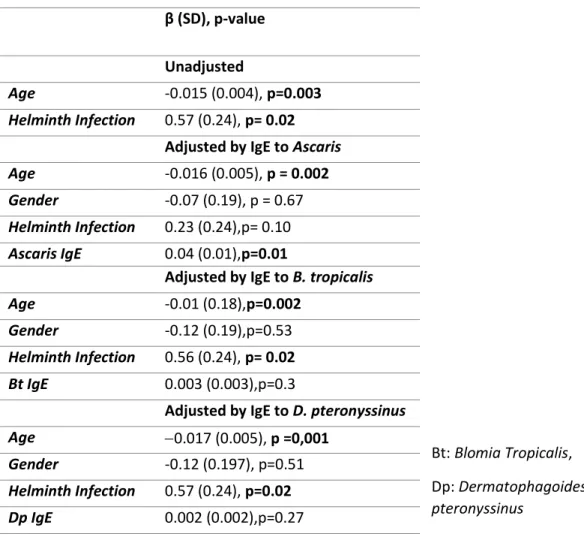
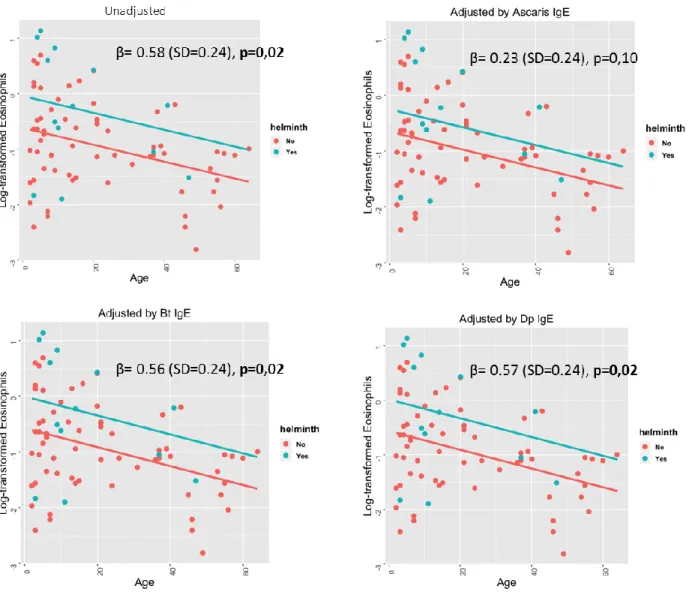
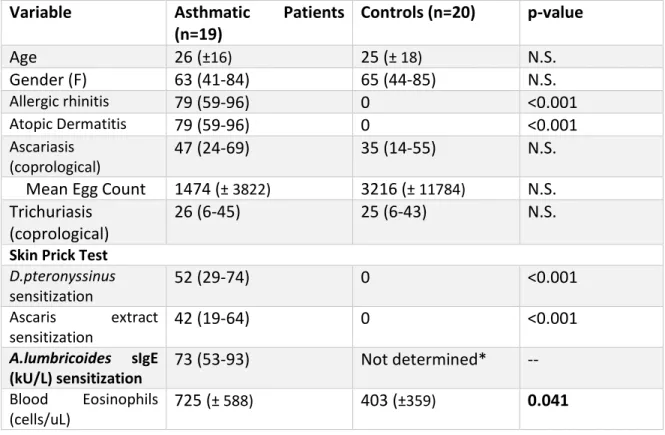
(14) relationship with helminth infection (β =0.003,SD=0.003,p=0.3; β=0.002,SD=0.002p=0.27, respectively).However, when A.lumbricoides IgE was included in the model only this variable remained as a significant predictor (β=0.04,SD=0.01,p=0.01),indicating that A.lumbricoides sensitization is more predictive of eosinophilia and helminth infection than HDM sensitization in this population (Figure 2).. Lower frequencies of CD24highCD38high B cells in asthmatic patients To investigate the frequency of the different Breg cell subsets, isolated peripheral blood mononuclear cells were stained for CD1d, CD5, CD19, CD24, CD38 and CD3. Gating examples are shown in Figure 1 and Supplementary Material 2 for the following two subsets: CD24+CD38+CD19+CD3- y CD5+CD1d+CD19+CD3-. In order to identify if the frequency of Breg cell subsets are lower in asthmatic patients, we compared Breg frequencies between 19 asthmatic patients and 20 healthy non-atopic controls matched by age and gender. These 19 asthmatic patients were selected by convenience from the entire sample of the study and matched by age and gender with other members from the community (Table 9). However asthmatic patients did have significantly more eosinophil counts than controls (p=0.041). There were no significant differences between total B cell percentages and absolute counts or between Ascaris infection and mean egg counts between groups (Table 9). Of note, there was a correlation between lower age and higher CD24highCD38high B cells (Pearson coefficient: 3.18, p-value: 0,048), and there were no significant differences according to 14.
(15) gender (data not shown). There were no significant differences between CD1d+ or CD5+ B cells between both groups (data not shown).Notably, we found significantly lower percentages of CD24highCD38high B cells in asthmatic patients compared to control subjects (average 1,3% vs 5,5%,respectively, p=0.0001). (Figure 2), while the distribution of. CD1dhighCD5+ B cells was nonsignificant between both groups (average 2,9% vs 3,5%, p= 0.06). In addition, we did not find any association between CD24highCD38high or CD1dhighCD5+ B cells with asthma exacerbations or severity criteria (ER visits, > 4 Exacerbations, Hospitalizations or episodes of severe dyspnea in the last 12 months) (data not shown). Regulatory B cell frequencies are independent of Ascaris lumbricoides infection We sought to identify if there were any differences in Bregs subsets depending on Ascaris lumbricoides infection. We did not find significant differences between infected and uninfected patients for CD1dhighCD5+ (average 2,7% vs 3,6%, respectively, p=0.055) and CD24highCD38high B cell subsets (average 3,5% vs 5,5%,respectively, p=0.28) (Figure 3). There was a trend for more regulatory CD1dhighCD5+ B cells in uninfected patients. However, when comparing CD1dhighCD5+ B cells based on Ascaris infection between asthmatic and controls separately, we did not find significant differences (data not shown), indicating that this effect may be due to more asthmatics being in the infected group and more non-asthmatics in the non-infected group. Moreover, we did not any find correlations between B cell subsets and blood eosinophil counts our sIgE to Ascaris (data not shown).. 15.
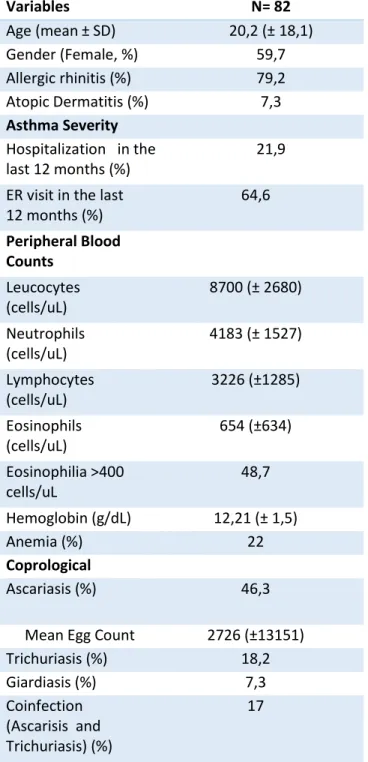
(16) Table 1. Baseline characteristics of the study population (n=82). Variables Age (mean ± SD) Gender (Female, %) Allergic rhinitis (%) Atopic Dermatitis (%) Asthma Severity Hospitalization in the last 12 months (%) ER visit in the last 12 months (%). N= 82 20,2 (± 18,1) 59,7 79,2 7,3 21,9 64,6. Peripheral Blood Counts Leucocytes (cells/uL). 8700 (± 2680). Neutrophils (cells/uL). 4183 (± 1527). Lymphocytes (cells/uL). 3226 (±1285). Eosinophils (cells/uL). 654 (±634). Eosinophilia >400 cells/uL. 48,7. Hemoglobin (g/dL) Anemia (%) Coprological Ascariasis (%). 12,21 (± 1,5) 22. Mean Egg Count Trichuriasis (%) Giardiasis (%) Coinfection (Ascarisis and Trichuriasis) (%). 2726 (±13151) 18,2 7,3 17. 46,3. 16.
(17) Variables Specific IgE D. pteronyssinus sIgE (kU/L). N= 82. 12,95 (±35,3). Sensitization (%) B. tropicalis sIgE (kU/L). 40,3 10,4 (±24,4). Sensitization (%) A.lumbricoides sIgE (kU/L). 61 2,4 (±5,1). Sensitization (%) Total IgE (kU/L) Skin Prick Test D. pteronyssinus sensitization (%). 62,3 1981 (±11409). Ascaris extract sensitization (%) Spirometry FEV 1 (%) FEV1/FVC (%). 35. 14,4. 78,6 (±17,07) 84 (±13.5). Geometric mean and standard deviation of mean are reported in parenthesis. 17.
(18) Table 2. Association between Ascaris lumbricoides infection and asthma exacerbations and severity criteria.. Variables. Positive Ascaris Infection. Positive IgE to Ascaris Ascaris Sensitization (Immunocap) (Skin Prick Test). Highly infected. Yes. No. Yes. No. Yes. >4000 epg. (Coprological) Yes. No. No. > 4 Exacerbations. 18 (47) 25 (57). 10 (46). 32 (59). 6 (50). 37 (53). 6 (86) 37 (49). >4 ER visits in the last 12 months. 8 (21). 3 (14). 13 (24). 1 (8). 16 (23). 4 (57) 13 (17). ER visit in the last 12 months. 23 (61) 30 (68). 13 (59) 35 (65). 8 (67). 45 (64). 4 (57) 49 (65). Hospitalization in the last 12 months. 9 (23). 2 (9). 2 (17). 16 (23). 3 (42) 15 (20). 9 (20). 9 (21). 14 (26). Chi Square test. n(%).Numbers in bold are statistically significant at P < 0.05. 18.
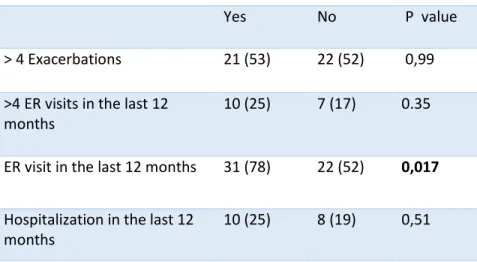
(19) Table 3. Association between blood eosinophilia and asthma exacerbations and indicators of asthma severity Variables. Eosinophils > 400 cells/ul Yes. No. P value. > 4 Exacerbations. 21 (53). 22 (52). 0,99. >4 ER visits in the last 12 months. 10 (25). 7 (17). 0.35. ER visit in the last 12 months. 31 (78). 22 (52). 0,017. Hospitalization in the last 12 months. 10 (25). 8 (19). 0,51. Chi Square test. N (%). Table 4. Adjusted logistic regression for Eosinophils > 400 cells/uL and ER visits in the last 12 months.. Variables. Eosinophils > 400 cells/ul aOR. (95% CI). P value. Age. 0.95. 0,92-0.98. 0.005. Gender. 0.79. 0.28-2.2. 0.78. ER visit in the last 12 months. 2.17. 0.74-6.3. 0.15. 19.
(20) Table 5. Association between Ascaris and Trichuris infection, atopy and blood eosinophils greater than 400 cells/uL. Variables. Eosinophils > 400 cells/uL Yes. No. P value. Ascaris infection. 20 (50). 18 (43). 0,517. Ascaris Sensitization (Immunocap). 28 (78). 20 (54). 0,009. Trichuriasis (Coprological). 10 (25). 5 (12). 0,125. Coinfection. 10 (25). 4 (9). 0,063. Ascaris SPT. 4 (10). 8 (19). 0.247. B. tropicalis sensitization. 27 (49). 20 (75). 0.019. D. pteronyssinus sensitization. 18 (50). 13 (31). 0.102. Chi Square test .N(%). 20.
(21) Table 6. Association between Ascaris and Trichuris infection, atopy and blood eosinophils greater than the 75th percentile. Variables. Eosinophils > 75th percentile Yes. No. P value. Ascariasis (Coprological). 15 (71). 23 (37). 0,008. Ascaris Sensitization (Immunocap). 16 (84). 32 (55). 0,023. Trichuriasis (Coprological). 8 (38). 7 (11). 0,006. Coinfection. 8 (38). 6 (10). 0,003. Ascaris sensitization (SPT). 2 (9,5). 10 (16). 0.44. B. tropicalis sensitization. 15 (79). 32 (55). 0.065. D. pteronyssinus sensitization. 7 (37). 24 (41). 0.72. Chi Square test. N (%). 21.
(22) 2000 1000 0. Ye s. 3000 2000 1000 0. N. o. N. p< 0.0001. 4000. Ascaris Sensitization (sIgE >0,35 kU/L). C. Ye s. 3000. Eosinophils (cells/uL). B. p<0.0001. 4000. o. A. Eosinophils (cells/uL). Figure 1. Variables associated with blood eosinophils. A) Mean eosinophil counts according to Ascaris sensitization B) Mean eosinophil counts according to active Ascaris infection C) Mean eosinophil counts according to infection severity D) Mean eosinophil counts according to age groups E) Mean Ascaris e.p.g according to age groups. Ascariasis (Coprological). D. E. 22.
(23) Table 7. Eosinophils greater than 400 cells/uL and helminth infection and sensitization: multivariate logistic regression analysis. Univariate Analysis*. OR. (95% CI). Multivariate Analysis**. P value. aOR. (95% CI). P value. Age. 0,946. (0,92-0,98). 0,001. 0,92. (0,89-0,97). 0,001. Gender. 0,553. (0,23-1,34). 0,19. 1,62. (0,34-2,5). 0,87. Active Ascaris Infection. 1,33. (0,56-3,18). 0,51. -. -. -. Active Trichuris infection. 2,46. (0,76-8,0). 0,13. -. -. -. Ascaris sensitization. 3,67. (1,36-9,95). 0,01. 6,9. (2,0-23,7). 0,002. HDM sensitization. 2,85. (1,08-7,54). 0,034. 5,44. (1,54-19,14). 0,008. Coinfection. 3,16. (0.90-11,1). 0,072. 3,23. (0,74-11,3). 0,13. * Only variables with p value < 0,1 were accounted for in the multivariable analysis **Adjusted for age, gender and coinfection status HDM: House dust mite. 23.
(24) Table 8. Log transformed eosinophils and specific IgE sensitization: adjusted linear regression β (SD), p-value Unadjusted Age. -0.015 (0.004), p=0.003. Helminth Infection. 0.57 (0.24), p= 0.02 Adjusted by IgE to Ascaris. Age. -0.016 (0.005), p = 0.002. Gender. -0.07 (0.19), p = 0.67. Helminth Infection. 0.23 (0.24),p= 0.10. Ascaris IgE. 0.04 (0.01),p=0.01 Adjusted by IgE to B. tropicalis. Age. -0.01 (0.18),p=0.002. Gender. -0.12 (0.19),p=0.53. Helminth Infection. 0.56 (0.24), p= 0.02. Bt IgE. 0.003 (0.003),p=0.3 Adjusted by IgE to D. pteronyssinus. Age. 0.017 (0.005), p =0,001. Gender. -0.12 (0.197), p=0.51. Helminth Infection. 0.57 (0.24), p=0.02. Dp IgE. 0.002 (0.002),p=0.27. Bt: Blomia Tropicalis, Dp: Dermatophagoides pteronyssinus. 24.
(25) Figure 2. Log transformed eosinophils and specific IgE sensitization: adjusted linear regression. Bt: Blomia Tropicalis, Dp: Dermatophagoides pteronyssinus. 25.
(26) Table 9. Subsample of Asthmatic patients and Healthy Controls Characteristics. Variable Age Gender (F) Allergic rhinitis Atopic Dermatitis Ascariasis (coprological). Mean Egg Count Trichuriasis (coprological) Skin Prick Test D.pteronyssinus sensitization Ascaris extract sensitization A.lumbricoides sIgE (kU/L) sensitization Blood Eosinophils (cells/uL). Asthmatic (n=19) 26 (±16) 63 (41-84) 79 (59-96) 79 (59-96) 47 (24-69). Patients Controls (n=20). p-value. 25 (± 18) 65 (44-85) 0 0 35 (14-55). N.S. N.S. <0.001 <0.001 N.S.. 1474 (± 3822) 26 (6-45). 3216 (± 11784) 25 (6-43). N.S. N.S.. 52 (29-74). 0. <0.001. 42 (19-64). 0. <0.001. 73 (53-93). Not determined*. --. 725 (± 588). 403 (±359). 0.041. Geometric mean and standard deviation of mean in parenthesis are reported. Frequency rates (%) for categorical variables are shown. Their 95% confident intervals are shown in parenthesis. *A.lumbricoides sIgE was not measured in control patients.. 26.
(27) Figure 3. Frequency of regulatory B cell subsets in peripheral blood from patients with allergic asthma and controls. A representative gating example is depicted on the left for each Breg cell subset, showing one matched healthy and asthmatic patient donor pair. (A) CD24hiCD38hi B cells (B) CD1dhiCD5+ B cells. Horizontal bars represent medians and standard errors of the mean.. 27.
(28) Figure 4. Frequency of regulatory B cell subsets in peripheral blood from A.lumbricoides. infected and uninfected individuals. (A) CD24hiCD38hi B cells (B) CD1dhiCD5+ B cells Horizontal bars represent medians and standard errors of the mean.. 28.
(29) Discussion This study was conducted in the community of Santa Catalina, a poor tropical community with scarce access to water sanitation services and high burden of helminthiasis and asthma 24.. In this community, we have previously shown that ascariasis exerts protective and risk. effects of on asthma, depending on the intensity of the infection 24. In this context, active infection or exposure to helminths may influence the predictive value of immunological biomarkers in asthma and its severity. To our knowledge, no information is available regarding the predictive value of eosinophils for asthma severity in helminth endemic populations. In high income countries, where helminths are not considered endemic, studies have determined that peripheral blood eosinophils are predictive of asthma severity. In an United Kingdom cohort of 130 248 patients with asthma blood eosinophil counts greater than 400 cells per μL, as compared with 400 cells per μL or less, eosinophilia was associated with a greater rate of asthma exacerbations (RR 1,42; 95% CI 1,36–1,47) and lower odds of achieving asthma control over the subsequent year (OR 0·74, 95% CI 0·72–0·77) 28. In US adults with persistent asthma, eosinophil count > 400/mm3 in 2010 was a risk factor for asthma exacerbations in 2011 (adjusted rate ratio 1.31 [95% CI, 1.07-1.60]; P = .009) and excessive short acting b2-agonist use (adjusted risk ratio 1.17 [95% CI, 1.03-1.1.33]; P= .015). 29. In another prospective study. of 271 US patients with severe uncontrolled asthma, a blood eosinophil cutoff point of greater than or equal to 400 cells/uL, was a risk factor in the outcome year in adjusted analyses for 2 or more asthma exacerbations (risk ratio, 1.55; 95% CI, 1.02-2.35; P =.04) and any asthma emergency department visit or hospitalization (risk ratio, 2.29; 95% CI, 1.1629.
(30) 4.55; P =.02) 30. In our study, eosinophils >400 cells/uL were associated with ER visits and inpatient or outpatient care in the previous 12 months (p=0.017) in an unadjusted analysis. However, this association loses significance when comparing severity criteria and eosinophils > 75th percentile, which could be explained by the strong association of helminth infection/sensitization and eosinophilia. Indeed, active Ascariasis, Trichuriasis, Ascaris sensitization, and coinfection were all significantly associated with Eosinophils > 75th. Moreover, in the multivariate analysis for eosinophilia > 400 cell/uL, only Ascaris sensitization remained significantly associated (OR= 6,9; 95% CI: 2,0-23,7; p=0.002). Thus, we argue that Ascaris lumbricoides exposure/infection is more determinant of eosinophilia than asthmatic status in this rural endemic population. Eosinophilia is considered to be a central mechanism in the host response against helminths. However, the influence of eosinophils in helminth infections is complex, and their role is highly dependent on the models of worm/host infection studied. 31.. For example, their function is dependent on. whether it is a primary or secondary infection, or intestinal vs non-intestinal infection 31. More importantly, there is a considerable scarcity of evidence in the effects of helminths in eosinophils in humans. 32.. One such study is the one by Alcântara-Neves et al. 33. , who. investigated the effects of single and co-infections with intestinal parasites (A. lumbricoides and T. trichiura) and Toxocara spp. on the following total blood eosinophils and found that the number of helminth infections was positively and statistically associated with eosinophilia at >4 and >10% in a dose-dependent manner. Our results also indicate that helminth infection and coinfection are associated with eosinophilia; however, our study used absolute numbers of eosinophils, which we believe are more appropriate for. 30.
(31) comparison between studies because eosinophilia is clinically defined in absolute numbers 34,35.. In our cohort, 48,7% (n=40) of patients had a blood eosinophil count greater than 400. cells/uL (Mean= 654, Median=390) . Conversely, in patients > 18 years old, 32, 4% (n=11) had a blood eosinophil count > 400 cell per uL. (Mean=446, Median= 340). Thus, in this population, a blood eosinophil count > 400 cell per uL might not be accurate to predict severity or to include these patients for therapy with biological agents using this criteria. More research needs to be done involving larger cohorts in order to determine possible cut off points for eosinophilia and asthma severity in populations heavily exposed to helminths. In this study, we found that A.lumbricoides sensitization is more predictive of eosinophilia than house dust mite sensitization, with eosinophils analyzed as a dichotomized variable (eosinophils > 400 cells/uL) and as a log-transformed continuous variable. This could have important clinical implications, since eosinophilia in asthmatic patients has always been associated with the atopic status of the patient, but in helminth endemic populations this blood population may be more driven by helminth exposure and infection. In a similar study, Hunninghake et al. found that sensitization to Ascaris lumbricoides is associated with increased total serum IgE and eosinophils in peripheral blood and asthma severity in 439 children from a population with low prevalence of helminthiasis in Costa Rica. 36,. which. correlates with our previous findings that A.lumbricoides sensitization is a risk factor for asthma in both urban. 37. and rural settings 24 , and is associated with increased odds of. suffering severe dyspnea episodes and ER attendance 36. In our study, Ascaris sensitization was not associated with asthma severity perhaps due to lack of power or because of the elevated percentage of Ascaris sensitization in our cohort (62,3%). 31.
(32) In this population we also sought to investigate if the frequency of regulatory B cells is different between asthmatic and non-asthmatic patients in a helminth endemic region. Interestingly, we found lower percentage of CD24 highCD38high B cells in asthmatic patients compared to control subjects. Few studies have studied this cell population in human asthmatic patients. Van der Vlugt 38 et al found higher CD24 highCD38high B cells and lower CD24CD27 B cells in asthmatic patients compared to controls. However, there was only a diminished IL-10 response in CD24hiCD27+ B cells from AA patients compared to controls upon LPS stimulation. Conversely, Luo J et al found that the percentages of CD19⁺ CD24 highCD38high. Bregs were significantly lower in allergic rhinitis patients than in healthy. individuals (P<0.05). Lower numbers of regulatory B cells in allergic patients would support the hypothesis that allergic patients are deficient in regulatory B cells and thus lack regulatory mechanisms that lead to allergen intolerance. For example, the induction of regulatory cells has proven to be an essential component in immunotherapy, the leading treatment to promote allergen tolerance. 16.. However, in autoimmune disorders, such as. systemic lupus erythematosus , studies have shown that regulatory B cells tend to be similar in these patients compared to healthy controls, but they are functionally impaired, producing less IL-10 and lacking suppressive capacity. 39.. Thus, further studies in allergic. patients should focus on the functionality of regulatory B cells, and to explore IL-10, IL-35 and TGF-b and other immunosuppressive molecules, and its capacity to regulate other cell populations. On the other hand, studies investigating the frequency and functionality of Bregs in helminth infected humans are also scarce. Van der glut et al collected PBMC from 20 32.
(33) Gabonese children that were either S. haematobium positive or negative and found significantly higher percentages of CD1dhigh B cells in infected children compared to uninfected children 18. In addition, after six months of treatment with praziquantel, CD1dhigh percentages were reduced to levels comparable to the uninfected control group. In another study by the same group with S. haematobium infected and uninfected Gabonese young adults, B cells from S. haematobium infected donors expressed cytoplasmic interleukin 10 (IL-10) and membrane-bound latency-associated peptide/transforming growth factor β1, compared with uninfected donors, only the percentage of CD1dhi B cells within the IL-10producing B-cell population significantly increased during infection, suggesting that only this B cell subset is increased during S. haematobium infection 40.Moreover, the percentage of Breg subsets did not correlate with helminth burden 40. In our group of subjects, there was a trend for more CD1dhighCD5+ cells in uninfected patients; this may be due to higher infection and egg burdens in asthmatic patients who in turn have lower frequency of regulatory B cells. However, the function and IL-10 expression should be investigated to determine if Ascaris lumbricoides can also induce functional regulatory B cells in humans.. Limitations Limitations of this study include its observational nature, and its relative small sample. In addition, we did not assess the use of beta agonist or oral corticosteroids, or treatment adherence, which could potentially modify basal eosinophils. In terms of selection bias, we 33.
(34) cannot rule out that patients with eosinophilia were more likely to be selected. Conversely, we cannot exclude confounding by other common helminth infections, such as Toxocara spp. Moreover, regulatory B cells were only analyzed in terms of frequency, and as we have stated, these B cells may not differ in frequency but may be functionally impaired. We also only assessed two regulatory B cell subsets, and there may be other subsets influenced by allergic disease or helminth infection status.. Conclusion In a rural community from the Colombian tropics, where helminths are endemic, sensitization to A.lumbricoides was more predictive of eosinophilia than sensitization to house dust mites. The frequency of regulatory B cell subsets was lower in asthmatic patients than controls. Further research should evaluate larger cohorts and determine the basal level of eosinophils in this population, and focus on the cellular function of regulatory B cells.. Funding source This work was funded by the Colombian government (Colciencias, Grant 590-2013) and the University of Cartagena.. Conflicts of interest The authors declare that they do not have conflicts of interest.. 34.
(35) Acknowledgements The authors thank the municipal authorities and community of Santa Catalina for their willingness to participate in the study.. REFERENCES 1.. Starr MC, Montgomery SP. Soil-transmitted Helminthiasis in the United States: a systematic review--1940-2010. Am J Trop Med Hyg. 2011;85(4):680-684. doi:10.4269/ajtmh.2011.110214.. 2.. Pullan RL, Smith JL, Jasrasaria R, Brooker SJ. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit Vectors. 2014;7(1):37. doi:10.1186/1756-3305-7-37.. 3.. Hotez PJ, Brindley PJ, Bethony JM, King CH, Pearce EJ, Jacobson J. Helminth infections: the great neglected tropical diseases. J Clin Invest. 2008;118(4):1311-1321. doi:10.1172/JCI34261.. 4.. Fumagalli M, Pozzoli U, Cagliani R, et al. Parasites represent a major selective force for interleukin genes and shape the genetic predisposition to autoimmune conditions. J Exp Med. 2009;206(6):1395-1408. doi:10.1084/jem.20082779.. 5.. Chico ME, Vaca MG, Rodriguez A, Cooper PJ. Soil-transmitted helminth parasites and allergy: observations from Ecuador. Parasite Immunol. 2018:e12590. doi:10.1111/pim.12590.. 6.. Wammes LJ, Mpairwe H, Elliott AM, Yazdanbakhsh M. Helminth therapy or elimination: Epidemiological, immunological, and clinical considerations. Lancet Infect Dis. 2014;14(11):1150-1162. doi:10.1016/S1473-3099(14)70771-6.. 7.. Zakzuk J. Inmunorregulación inducida por helmintos: una actualización. IATREIA. 2016;29(2):182-193. doi:10.17533/udea.iatreia.v29n2a07.. 8.. Caraballo L, Acevedo N, Zakzuk J. Ascariasis as a model to study the helminth/allergy relationships. Parasite Immunol. November 2018:e12595. doi:10.1111/pim.12595.. 9.. Caraballo L, Zakzuk J, Lee BW, et al. Particularities of allergy in the Tropics. World Allergy Organ J. 2016;9(1):20. doi:10.1186/s40413-016-0110-7.. 35.
(36) 10.. Caraballo L. The tropics, helminth infections and hygiene hypotheses. Expert Rev Clin Immunol. 2018;14(2):99-102. doi:10.1080/1744666X.2018.1424543.. 11.. Lambrecht BN, Hammad H. The immunology of asthma. Nat Immunol. 2015;16(1):45-56. doi:10.1038/ni.3049.. 12.. Kim H, Ellis AK, Fischer D, et al. Asthma biomarkers in the age of biologics. Allergy, Asthma Clin Immunol. 2017;13(1):48. doi:10.1186/s13223-017-0219-4.. 13.. McCracken JL, Tripple JW, Calhoun WJ. Biologic therapy in the management of asthma. Curr Opin Allergy Clin Immunol. 2016;16(4):375-382. doi:10.1097/ACI.0000000000000284.. 14.. Walsh GM. Mepolizumab-based therapy in asthma. Curr Opin Allergy Clin Immunol. 2015;15(4):392-396. doi:10.1097/ACI.0000000000000183.. 15.. Palomares O, Akdis M, Martín-Fontecha M, Akdis CA. Mechanisms of immune regulation in allergic diseases: the role of regulatory T and B cells. Immunol Rev. 2017;278(1):219-236. doi:10.1111/imr.12555.. 16.. van de Veen W, Stanic B, Wirz OF, Jansen K, Globinska A, Akdis M. Role of regulatory B cells in immune tolerance to allergens and beyond. J Allergy Clin Immunol. 2016;138(3):654-665. doi:10.1016/j.jaci.2016.07.006.. 17.. van der Vlugt LEPM, Mlejnek E, Ozir-Fazalalikhan A, et al. CD24(hi)CD27(+) B cells from patients with allergic asthma have impaired regulatory activity in response to lipopolysaccharide. Clin Exp Allergy. 2014;44(4):517-528. doi:10.1111/cea.12238.. 18.. van der Vlugt LEPM, Labuda LA, Ozir-Fazalalikhan A, et al. Schistosomes Induce Regulatory Features in Human and Mouse CD1dhi B Cells: Inhibition of Allergic Inflammation by IL-10 and Regulatory T Cells. Bozza PT, ed. PLoS One. 2012;7(2):e30883. doi:10.1371/journal.pone.0030883.. 19.. Obieglo K, Schuijs MJ, Ozir-Fazalalikhan A, et al. Isolated Schistosoma mansoni eggs prevent allergic airway inflammation. Parasite Immunol. 2018;40(10):e12579. doi:10.1111/pim.12579.. 20.. van der Vlugt LEPM, Obieglo K, Ozir-Fazalalikhan A, Sparwasser T, Haeberlein S, Smits HH. Schistosome-induced pulmonary B cells inhibit allergic airway inflammation and display a reduced Th2-driving function. Int J Parasitol. 2017;47(9):545-554. doi:10.1016/j.ijpara.2017.02.002.. 21.. Smits HH, Hammad H, van Nimwegen M, et al. Protective effect of Schistosoma mansoni infection on allergic airway inflammation depends on the intensity and chronicity of infection. J Allergy Clin Immunol. 2007;120(4):932-940. doi:10.1016/j.jaci.2007.06.009.. 22.. van der Vlugt LEPM, Labuda LA, Ozir-Fazalalikhan A, et al. Schistosomes Induce Regulatory Features in Human and Mouse CD1dhi B Cells: Inhibition of Allergic Inflammation by IL-10 and Regulatory T Cells. Bozza PT, ed. PLoS One. 2012;7(2):e30883. doi:10.1371/journal.pone.0030883.. 23.. Smits HH, Hammad H, van Nimwegen M, et al. Protective effect of Schistosoma mansoni infection on allergic airway inflammation depends on the intensity and chronicity of infection. J Allergy Clin Immunol. 2007;120(4):932-940. doi:10.1016/j.jaci.2007.06.009.. 36.
(37) 24.. Zakzuk J, Casadiego S, Mercado A, Alvis-Guzman N, Caraballo L. Ascaris lumbricoides infection induces both, reduction and increase of asthma symptoms in a rural community. Acta Trop. 2018;187:1-4. doi:10.1016/j.actatropica.2018.07.016.. 25.. Dennis RJ, Caraballo L, García E, et al. Prevalence of asthma and other allergic conditions in Colombia 2009–2010: a cross-sectional study. BMC Pulm Med. 2012;12(1):17. doi:10.1186/1471-2466-12-17.. 26.. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319-338. doi:10.1183/09031936.05.00034805.. 27.. World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. https://www.who.int/vmnis/indicators/haemoglobin.pdf. Accessed November 27, 2018.. 28.. Price DB, Rigazio A, Campbell JD, et al. Blood eosinophil count and prospective annual asthma disease burden: A UK cohort study. Lancet Respir Med. 2015;3(11):849-858. doi:10.1016/S2213-2600(15)00367-7.. 29.. Zeiger RS, Schatz M, Li Q, Chen W, Khatry DB. High Blood Eosinophil Count Is a Risk Factor for Future Asthma Exacerbations in Adult Persistent Asthma. J Allergy Clin Immunol Pract. 2014;2(6):741-750.e4. doi:10.1016/j.jaip.2014.06.005.. 30.. Zeiger RS, Schatz M, Dalal AA, et al. Blood Eosinophil Count and Outcomes in Severe Uncontrolled Asthma: A Prospective Study. J Allergy Clin Immunol Pract. 2017;5(1):144153.e8. doi:10.1016/j.jaip.2016.07.015.. 31.. Huang L, Appleton JA. Eosinophils in Helminth Infection: Defenders and Dupes. Trends Parasitol. 2016;32(10):798-807. doi:10.1016/j.pt.2016.05.004.. 32.. Klion AD, Nutman TB. The role of eosinophils in host defense against helminth parasites. J Allergy Clin Immunol. 2004;113(1):30-37. doi:10.1016/j.jaci.2003.10.050.. 33.. Alcântara-Neves NM, de S G Britto G, Veiga RV, et al. Effects of helminth co-infections on atopy, asthma and cytokine production in children living in a poor urban area in Latin America. BMC Res Notes. 2014;7:817. doi:10.1186/1756-0500-7-817.. 34.. O’Sullivan JA, Bochner BS. Eosinophils and eosinophil-associated diseases: An update. J Allergy Clin Immunol. 2017:1-13. doi:10.1016/j.jaci.2017.09.022.. 35.. Rosenberg HF, Dyer KD, Foster PS. Eosinophils: Changing perspectives in health and disease. Nat Rev Immunol. 2013;13(1):9-22. doi:10.1038/nri3341.. 36.. Buendía E, Zakzuk J, Mercado D, Alvarez A, Caraballo L. The IgE response to Ascaris molecular components is associated with clinical indicators of asthma severity. World Allergy Organ J. 2015;8(1):1-11. doi:10.1186/s40413-015-0058-z.. 37.. Ahumada V, García E, Dennis R, et al. IgE responses to Ascaris and mite tropomyosins are risk factors for asthma. Clin Exp Allergy. 2015;45(7):1189-1200. doi:10.1111/cea.12513.. 38.. van der Vlugt LEPM, Mlejnek E, Ozir-Fazalalikhan A, et al. CD24 hi CD27 + B cells from patients with allergic asthma have impaired regulatory activity in response to lipopolysaccharide. Clin Exp Allergy. 2014;44(4):517-528. doi:10.1111/cea.12238.. 37.
(38) 39.. Blair PA, Noreña LY, Flores-Borja F, et al. CD19+CD24hiCD38hi B Cells Exhibit Regulatory Capacity in Healthy Individuals but Are Functionally Impaired in Systemic Lupus Erythematosus Patients. Immunity. 2010;32(1):129-140. doi:10.1016/j.immuni.2009.11.009.. 40.. Van Der Vlugt LEPM, Zinsou JF, Ozir-Fazalalikhan A, et al. Interleukin 10 (IL-10)-producing CD1dhi regulatory B cells from Schistosoma haematobium-infected individuals induce IL-10positive T cells and suppress effector T-cell cytokines. J Infect Dis. 2014;210(8):1207-1216. doi:10.1093/infdis/jiu257.. 38.
(39) Supplementary Material 1. Informed Consents. CONSENTIMIENTO INFORMADO PARA TOMA DE MUESTRAS A ADULTOS. Título del proyecto: ASCARIASIS, TRATAMIENTO ANTI-HELMÍNTICO Y SUS EFECTOS SOBRE LA RESPUESTA INMUNE DE TIPO ALÉRGICA EN UNA POBLACIÓN RURAL DE BOLIVAR Sub-proyecto: Prevalencia de las Enfermedades alérgicas y Parasitosis Intestinal en Santa Catalina, Bolívar. Investigadores: Luis Caraballo, Josefina Zakzuk y Nelson Alvis. La Universidad de Cartagena lo invita a que participe en la sección del proyecto denominada: Prevalencia de las Enfermedades alérgicas y Parasitosis Intestinal en Santa Catalina, Bolívar, el cual no tiene ningún costo para ustedes diferente a su tiempo. Su decisión de participar es voluntaria. Por favor, lea este formulario de consentimiento cuidadosamente, y haga cuantas preguntas considere. Aún si ahora usted decide participar podrá abandonar el estudio en cualquier momento si así lo desea.. Este estudio es una investigación de tipo observacional que se realizará por profesionales investigadores de la Universidad de Cartagena. Antes de ser realizado, el estudio cuenta con el aval y aprobación del comité de Ética de Universidad de Cartagena. Su objetivo es conocer cuál es la prevalencia de las enfermedades alérgicas en Santa Catalina y su relación con las parasitosis intestinales. La información recogida será muy útil, pues es representativa de la zona rural de la Costa Atlántica.. Se harán preguntas, que se consignarán por escrito en un formulario, indagando sobre síntomas de enfermedades alérgicas, condiciones de vida, hábitos, características de la vivienda, antecedentes personales y familiares. Toda esta información será incorporada a la base de datos del estudio, cuyo carácter es confidencial y que solo será empleada con fines de investigación biomédica o epidemiológica. Se le pedirán en días diferentes dos muestras consecutivas de heces con el fin de determinar la presencia de parásitos intestinales. Estas serán recogidas en su hogar por el mismo médico o el personal de apoyo contratado para la ejecución del proyecto. Los resultados del examen se le darán a conocer de manera oportuna, así como el tratamiento que. 39.
(40) deba tomar en caso de necesitarlo, lo cual será responsabilidad suya si lo sigue o no. Los investigadores no se comprometen a suministrarle el medicamento que necesite.. Es probable que sea seleccionado a una segunda fase del estudio, donde por limitaciones económicas solo se incluirá a un grupo representativo de las personas encuestadas. Al participante de la segunda fase se le tomará una muestra de sangre por punción venosa a nivel del antebrazo. La punción será realizada por una persona entrenada, con material desechable y adecuadas condiciones de limpieza. También se le harán algunas preguntas para completar un cuestionario. La muestra de sangre será marcada con un código especial del estudio. La punción venosa representa un riego muy bajo y como única consecuencia podría resultar un pequeño hematoma (morado) o infección en el sitio donde penetra la aguja. En caso de presentarse alguna complicación con la punción venosa, el Instituto de Investigaciones Inmunológicas de la Universidad de Cartagena cubrirá la atención de esta complicación. Se le realizarán pruebas cutáneas de alergias, las cuales son una herramienta diagnóstica bastante confiable que no produce molestias salvo el prurito que aparece si la persona es alérgica. En este caso también se le formará una pequeña roncha que desaparecerá en dos horas. Esta prueba se utiliza en todos los países para el diagnóstico de alergias y se ha utilizado en otros estudios como este sin reportarse efectos adversos.. ¿De qué manera se protege mi privacidad?. Los datos de este estudio serán publicados. El nombre o cualquier forma de identificación de Usted no serán utilizados sin su expresa autorización. La información consignada en la historia clínica podrá ser utilizada por el investigador para el estudio. Esta información puede incluir el nombre, fecha de nacimiento, la dirección, el número de teléfono y la historia médica suya. Se utilizará un código que lo identifica y que solo conocerán los investigadores.. Usted puede hablar con los investigadores en cualquier momento y hacer cualquier pregunta que tenga en relación con el estudio.. A los investigadores: la Doctora Josefina Zakzuk, el Doctor Luis Caraballo y el Doctor Nelson Alvis los puede encontrar en los siguientes teléfonos: 6698491 y 3215412280 o por correo electrónico: [email protected], [email protected] y [email protected].. 40.
(41) Me ha sido dada la oportunidad de hacer todas las preguntas y éstas han sido respondidas. Me han dado una copia de este consentimiento informado. Firmo como manifestación de voluntad y aprobación para participar en este estudio:. Nombre del Voluntario. No del Documento de Identidad. Testigo No. 1. Fecha. Testigo No. 2. Nombre:. Nombre:. C.C. No.. C.C. No.. Dirección. Relación con el voluntario. Dirección. Relación con el voluntario. Fecha. Fecha. Firma del Investigador que administra en consentimiento Fecha. 41.
(42) CONSENTIMIENTO INFORMADO PARA TOMA DE MUESTRAS A MENOR. Título del proyecto: ASCARIASIS, TRATAMIENTO ANTI-HELMÍNTICO Y SUS EFECTOS SOBRE LA RESPUESTA INMUNE DE TIPO ALÉRGICA EN UNA POBLACIÓN RURAL DE BOLIVAR Sub-proyecto: Prevalencia de las Enfermedades alérgicas y Parasitosis Intestinal en Santa Catalina, Bolívar. Investigadores: Luis Caraballo, Josefina Zakzuk y Nelson Alvis. La Universidad de Cartagena invita a su hijo a que participe en la sección del proyecto denominada: Prevalencia de las Enfermedades alérgicas y Parasitosis Intestinal en Santa Catalina, Bolívar, el cual no tiene ningún costo para ustedes diferente a su tiempo. Su decisión de que su hijo/hija participe en este estudio es voluntaria. Por favor, lea este formulario de consentimiento cuidadosamente, y haga cuantas preguntas considere. Aún si usted decide que su hijo/a participe, él/ella podrá abandonar el estudio en cualquier momento si así lo desea.. Este estudio es una investigación de tipo observacional que se realizará por profesionales investigadores de la Universidad de Cartagena. Antes de ser realizado, el estudio cuenta con el aval y aprobación del comité de Ética de Universidad de Cartagena. Su objetivo es conocer cuál es la prevalencia de las enfermedades alérgicas en Santa Catalina y su relación con las parasitosis intestinales. La información recogida será muy útil, pues es representativa de la zona rural de la Costa Atlántica.. Se harán preguntas, que se consignarán por escrito en un formulario, indagando sobre síntomas de enfermedades alérgicas, condiciones de vida, hábitos, características de la vivienda, antecedentes personales y familiares. Toda esta información será incorporada a la base de datos del estudio, cuyo carácter es confidencial y que solo será empleada con fines de investigación biomédica o epidemiológica. De su hijo (a) o apoderado se obtendrán en días diferentes dos muestras consecutivas de heces con el fin de determinar la presencia de parásitos intestinales.. 42.
(43) Estas serán recogidas en su hogar por el mismo médico o el personal de apoyo contratado para la ejecución del proyecto. Los resultados del examen se le darán a conocer de manera oportuna, así como el tratamiento que deba tomar su hijo o custodio en caso de necesitarlo, lo cual será responsabilidad suya si lo sigue o no. Los investigadores no se comprometen a suministrarle el medicamento que necesite.. Es probable que su hijo sea seleccionado a una segunda fase del estudio, donde por limitaciones económicas, solo se incluirá a un grupo representativo de las personas encuestadas. A quien participe en la segunda fase se le tomará una muestra de sangre por punción venosa a nivel del antebrazo. La punción será realizada por una persona entrenada, con material desechable y adecuadas condiciones de limpieza. También se le harán algunas preguntas para completar un cuestionario. La muestra de sangre será marcada con un código especial del estudio. La punción venosa representa un riesgo muy bajo y como única consecuencia podría resultar un pequeño hematoma (morado) o infección en el sitio donde penetra la aguja. En caso de presentarse alguna complicación con la punción venosa, el Instituto de Investigaciones Inmunológicas de la Universidad de Cartagena cubrirá la atención de esta complicación. Se le realizarán pruebas cutáneas de alergias, las cuales son una herramienta diagnóstica bastante confiable que no produce molestias salvo el prurito que aparece si la persona es alérgica. En este caso también se le formará una pequeña roncha que desaparecerá en dos horas. Esta prueba se utiliza en todos los países para el diagnóstico de alergias incluyendo niños y se ha utilizado en otros estudios como este sin reportarse efectos adversos.. ¿De qué manera se protegerá la privacidad de mi hijo(a)?. Los datos de este estudio serán publicados. El nombre o cualquier forma de identificación de su hijo o apoderado no serán utilizados sin su expresa autorización. La información consignada en la historia clínica de su hijo o apoderado podrá ser utilizada por el investigador para el estudio. Esta información puede incluir el nombre, fecha de nacimiento, la dirección, el número de teléfono, la historia médica de su hijo(a). Se utilizará un código que identifica a su hijo que solo conocerán los investigadores.. Me ha sido dada la oportunidad de hacer todas las preguntas y éstas han sido respondidas. Me han dado una copia de este consentimiento informado.. Usted puede hablar con los investigadores en cualquier momento y hacer cualquier pregunta que tenga en relación con el estudio. Los investigadores no tendrán ningún tipo de compensación económica por este estudio.. 43.
(44) Los investigadores: A la Doctora Josefina Zakzuk, el Doctor Luis Caraballo y el Doctor Nelson Alvis los puede encontrar en los siguientes teléfonos: 6698491 y 3215412280 o por correo electrónico: [email protected], [email protected] y [email protected].. Estoy de acuerdo con la participación de mi hijo o apoderado en el estudio: Nombre del Voluntario No del Documento de Identidad. Fecha. Firma del Padre o Tutor Nombre: C.C. No.. C.C. No.. Fecha. Fecha. Testigo No. 1. Testigo No. 2. Nombre:. C.C.. No.. Dirección. Firma de la madre o tutor Nombre:. _. Nombre:. C.C. No.. Dirección. Relación con el voluntario Relación con el voluntario. Fecha Fecha. Firma del Investigador que administra en consentimiento Fecha. 44.
(45) FORMATO DE ASENTIMIENTO DEL MENOR. Título del proyecto: ASCARIASIS, TRATAMIENTO ANTI-HELMÍNTICO Y SUS EFECTOS SOBRE LA RESPUESTA INMUNE DE TIPO ALÉRGICA EN UNA POBLACIÓN RURAL DE BOLIVAR Sub-proyecto: Prevalencia de las Enfermedades alérgicas y Parasitosis Intestinal en Santa Catalina, Bolívar Investigadores: Luis Caraballo, Nelson Alvis y Josefina Zakzuk A mí se me ha pedido participar en esta investigación. Los Dres. Josefina Zakzuk y Luis Caraballo en persona u otro médico del estudio me han explicado en qué consiste esta investigación. Este estudio se está llevando a cabo para conocer que tan frecuente son el asma, las alergias y la infección por parásitos en Santa Catalina, y si los dos problemas tienen alguna relación. Se te recogerán dos muestras de heces para saber si tienes parásitos. Es probable que se te invite a participar en una segunda fase del estudio para tomarte una muestra de sangre, la cual es de un riesgo bajo y como única consecuencia podría resultar un hematoma o morado o infección en el sitio de punción. También para realizarte pruebas cutáneas de alergia, un examen no doloroso que se hace en la piel y que puede ocasionarte picazón en el lugar del cuerpo donde te las hagan. Esta sensación no durará más de 30 minutos. Este estudio puede que no tenga beneficios directos para ti, pero será de gran ayuda para las próximas generaciones, ya que nos permitirá conocer la gravedad de estas enfermedades en tu comunidad. No es obligatorio que participes en este estudio si no lo deseas, aunque tus padres digan que sí. Puedes hacer cualquier pregunta sobre este estudio en cualquier momento, así como negarte a seguir participando cuando lo desees. Los datos de este estudio serán publicados. El nombre o cualquier forma de identificación no serán utilizados sin su expresa autorización.. La información consignada en tu historia clínica podrá ser utilizada por los investigadores para el estudio.. Nombre del Voluntario. 45.
(46) Supplementary Material 2. Gating Strategy. 46.
(47) 47.
(48)
Figure


+7

Documento similar
The expansionary monetary policy measures have had a negative impact on net interest margins both via the reduction in interest rates and –less powerfully- the flattening of the
Jointly estimate this entry game with several outcome equations (fees/rates, credit limits) for bank accounts, credit cards and lines of credit. Use simulation methods to
In our sample, 2890 deals were issued by less reputable underwriters (i.e. a weighted syndication underwriting reputation share below the share of the 7 th largest underwriter
Prevalence and severity of dental fluorosis in a Mexican community with above-optimal fluoride concentration in drinking water.. The severity in dental fluorosis in children
The Dwellers in the Garden of Allah 109... The Dwellers in the Garden of Allah
This study examined the presence of neurodevelopmental regression and its effects on the clinical manifestations and the severity of autism spectrum disorder (ASD) in a group
Exosomes released by eosinophils are able to alter several functions associated with asthmatic pathology on both eosinophils themselves and structural lung cells, such as small
Figure 5.5: Difference in the EADS a) for pristine and b) for photooxidized KP115:PCBM thin films. Figure 5.6: Charge transients KP115:PCBM solar cells a) at different
