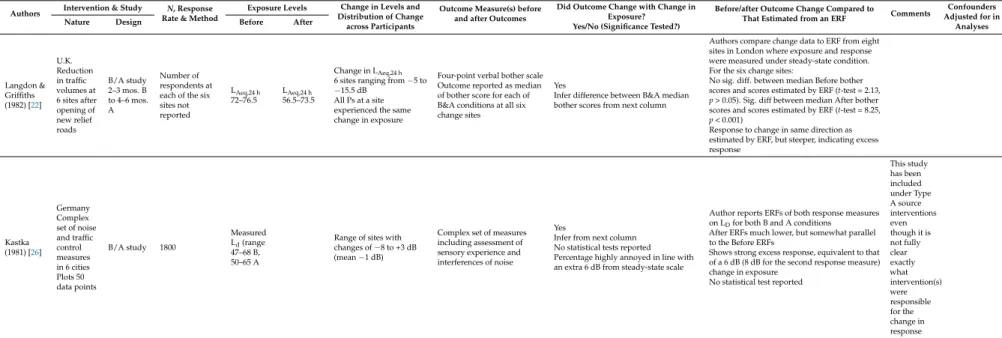
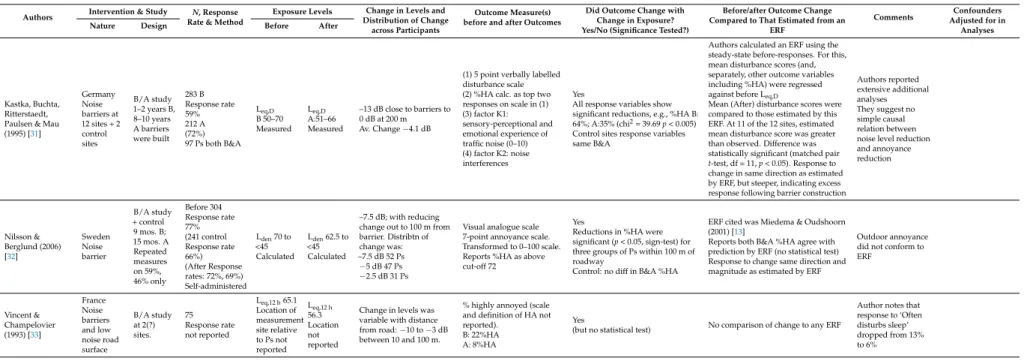
Similarly, individual studies were included that reported a change in the exposure of the population in question. We compared the magnitude of the observed change in health outcome with the magnitude of the change that would be 'predicted' based on the same change in exposure at the relevant ERF. If the observed health outcome changed in the same way as the ERF predicted change, the conclusion was that the ERF could have estimated the magnitude of the response to the intervention given the magnitude of the change in exposure.
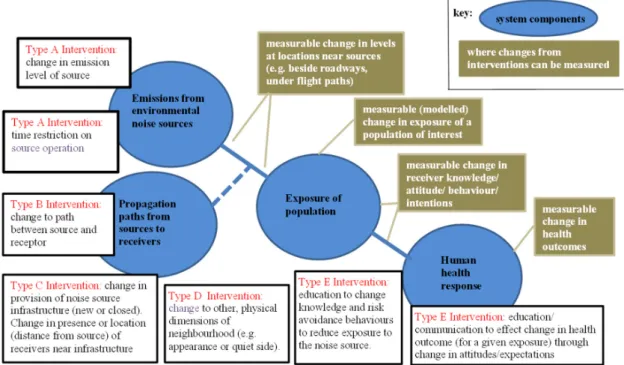
There is also an observation on the relationship of the observed change in response to that estimated by the same change in a corresponding ERF. Gender, age, education level, marital status, access to a bedroom on the quiet side of the building, and sensitivity. They are distinguished from type A interventions by the magnitude of the change in flows (eg, traffic flow on the nearest road for some participants dropped from 60,000 vehicles/day to zero).
12 dB Avg LAeq,24 h reduction Distribution of magnitude of change across individual P's not reported. The details of the two studies in Table 8 were reported under irritation outcomes above (Table 4). The summary details of the two studies reported in Table 9 (new tunnels removing traffic flow on surface roads) are also reported under irritation outcomes above (Table 5).
Gender, age, level of education, marital status, access to a bedroom on the quiet side of the building and sensitivity to noise. A summary of the details of one study in Table 10 (new tunnels eliminating traffic flow on surface roads) was reported under the disruption outcomes above (Table 6). The location of the living room is more important than the location of the bedroom (not consistent with other studies).
Evidence: Aircraft Noise
The changes at Zurich were mainly related to changes in the number of flights in the shoulder hours: early morning and late evening. In all three studies, there was evidence that the changes in noise exposure, due to the flight path changes, resulted in changes in irritation outcomes and that these observed changes were statistically significant. Regarding the strength of association between the change in exposure and the change in irritation responses, all intervention studies showed that the response was of some magnitude, at least as estimated by a constant ERF for irritation.
Further, they all provide evidence that the change in response was an over-response to the change - both for reduced and increased exposures in one study, and for increased exposures in the other two. An interesting development in intervention studies was the inclusion (in both the Amsterdam and Zurich studies) of both level and change in level as exposure variables for participants, for modeling the effects of change. Evidence of overresponse was tested statistically in the Amsterdam study and presented graphically in the other two studies.
The Amsterdam study provided evidence on the persistence of over-response – it is still present three years after the intervention – albeit with an unexplained temporary reduction from the fourth panel survey. The range of interference change in this indicator was -12 dB to +12 dB, but between -3 dB and +3 dB for ~70% of the 394 Ps who experienced interference. Descriptively demonstrated that Ps that experienced an increase through the intervention exhibited a fairly strong excess response.
Part of the Health Impact Assessment Schiphol Airport program Excessive response was not explained by non-acoustic factors. The author notes excess response in the +7 dB range only - but it is also present in the +3 dB range. Response to change in the same direction as estimated by ERF, but steeper, indicating excessive response.
In both studies (Table 14), there was evidence that changes in noise exposure due to flight path changes resulted in changes in sleep disturbance scores. In the Amsterdam study, it was also demonstrated that the response was in the same direction and of a magnitude as assessed by a steady-state ERF for sleep disturbance for Amsterdam derived from pre-intervention responses. As in the three aircraft noise studies in Table 13, the intervention in this study (Table 15) involved flight path rearrangements resulting from the opening of a new airport and the closing of another.
Evidence: Rail Noise
There was a parallel survey in the same area that experimentally manipulated the information given to Ps about noise attenuation. However, the author suggests that concerns are less where Ps have been given information compared to where information has not been given.

Discussion
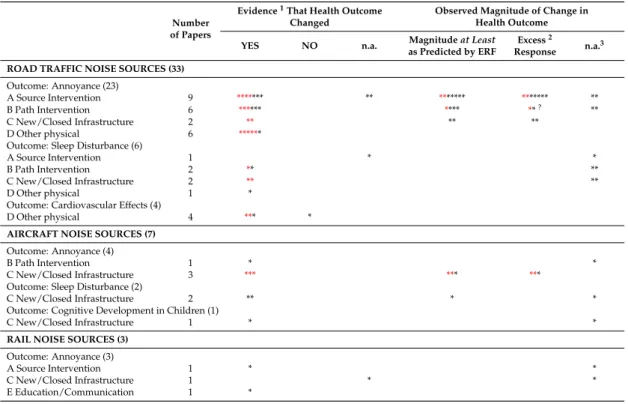
Summary of evidence from the individual studies on the effect of the intervention on health outcomes. Findings interpreted by original, or current, authors based on data/tables/plots in the original study.1 Note that the evidence is indirect for Intervention Type D (Other Physical).2 Excess response occurs where the overall difference between those observed before and after results are greater than the magnitude of the change in response estimated from an ERF, for a given change in exposure. In addition, the context surrounding the intervention should be considered, such as attitudes towards politics and the party carrying out the measures, expectations of the effectiveness of the intervention and satisfaction with the housing area.
Almost all entries in Table 19 were before-and-after studies, with identification of the magnitude of change in outcome determined by the timing of the post-intervention follow-up study. Although the evidence is sparse and scattered, the consistent conclusion is that the latter follow-up studies showed no difference in the results of these studies immediately after the intervention - with no reduction in the size of the effect, including excess response, if it was present. Excess response occurs where the total difference between the pre-result and the post-results is greater than the magnitude of the change in response estimated from an ERF for the given change in exposure.
This study found that: 'Evidence of the magnitude and persistence of the change effect over time. Currently, many assessments appear to be adjuncts to interventions rather than an integral part of interventions. The effect of an intervention on the exposure of defined populations needs to be assessed and its effect on the health outcomes of the same populations – not just changes in noise levels resulting from the intervention.
We recognize the difficulty of doing so in many intervention studies, but precise specification of the change in exposure for individuals or subgroups is desirable. Partly to further this, we suggest that there are advantages to following the approach used in two of the individual aircraft noise studies [47,48] of reporting both the noise exposure before the intervention and the change in noise exposure as a result of the intervention, by study participants, and by using both parts in the analysis. While many intervention studies use a before-and-after design, there is generally insufficient consideration that the change in human response to a step change in exposure may have a different time course than the change in exposure.
In reporting the evidence for overresponse (in annoyance outcomes) above, we noted that overresponse occurs when the magnitude of the observed change in outcomes exceeds that 'predicted' by the ERF, regardless of whether the observed prognosis and post-outcomes are themselves on the ERF curve. In addition, there are a range of system-wide issues that need to be considered in future evaluations of the health outcomes of transport noise interventions. We list them here, largely without comment, except to point out that few of these issues have been raised in any of the papers examined in the systematic review.
Conclusions
The minimum magnitude of change in disorder outcomes due to interventions can be predicted using an appropriate exposure-response function (ERF). Furthermore, in most of these studies, the magnitude of change in response to the intervention indicated a change effect—an excess of response over and above the level effect predicted using the ERF. Following the approach [ 45 , 46 ], reporting the pre-intervention noise exposure and the change in noise exposure due to the intervention of the study participants, has advantages and uses both in the analyses.
The results of the studies we have available about other physical interventions were obtained mainly through indirect evidence (comparison of results under different conditions, rather than before-after designs). The environmental noise intervention studies included in this review focused on changes in the site of the interventions. We have shown that there are a number of system-wide factors that must also be considered in any comprehensive assessment of the human health effects of any particular environmental noise intervention.
It was delivered as part of the evidence base for the Environmental Noise Guidelines for the European Region. In Proceedings of the Congress and Conference INTER-NOISE and NOISE-CON, San Francisco, CA, USA, 9–12 August 2015. In Proceedings of the Congress and Conference INTER-NOISE and NOISE-CON, Innsbruck, Austria, 15-18 September 2013.
In Proceedings of the INTER-NOISE and NOISE-CON Congress and Conference, Honolulu, HI, USA, 3-6. December 2006. In Proceedings of the 6th International Congress on Noise as a Public Health Problem, Noise &. A full-scale intervention example of the quiet side concept in a residential area exposed to road traffic noise: Effects on the perceived sound environment and general nuisance.
In Proceedings of the 29th International Congress and Exposition on Noise Control Engineering, Nice, France, 27–30 August 2000; pp. Road Traffic Noise and Annoyance: A Quantification of the Effect of Quiet Side Exposure in Residential. Int. Exposure modifiers of the relationships of transport noise with high blood pressure and noise annoyance.J.