This study therefore examined horizontal inequality in the utilization of maternal and child health care in Nigeria. The poorest women with no education were less likely to attend antenatal care and use skilled delivery compared to the wealthiest women with higher education.
Preamble
This study is focused on the estimation of horizontal inequality which implies examining the contributions of the need and the non-need variables to maternal and child health care utilization in Nigeria. The state of maternal and child health is one indicator of a society's level of development as well as an indicator of the performance of the health care system.
Statement of the Problem
Assess the determinants of utilization of maternal and child health care services in Nigeria. Access to maternal and child health care in Nigeria, especially in rural areas, is critical for uptake. However, the model provides a basis for analyzes of the determinants of health care utilization.
Therefore, the need and non-need variables are not defined in the maternal and child health care literature. The two theoretical frameworks are discussed in the context of maternal and child health care. Maternal health care (respondent's age and pregnancy status), child health care (child's age and under five).

Objectives of the Study
Justification for the Study
This study also differs from the existing studies as it examines access issues in the determinants of maternal and child health care. In terms of policy relevance, the profile of horizontal inequality in the use of maternal and child health care will reveal the main drivers of inequality.
Scope of the Study
These variables represent the common maternal characteristics that determine the use of maternal and child health care.
Organization of the Study
Maternal and Child Health Care
Antenatal Care
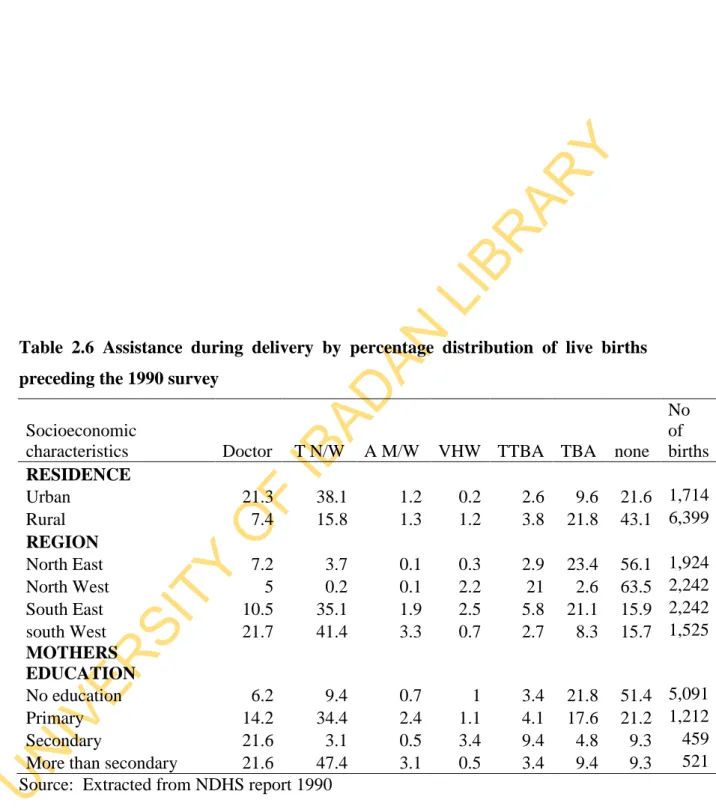
Inequality in the use of antenatal care is observed according to residence, region and educational status of women. Additionally, 54.4% of women with no education are unlikely to attend antenatal care, compared to 0.8% of women with higher education.
Skilled Delivery
In the South West, about 21.7% of women are assisted by doctors and 41.4% by trained nurses and midwives. In Table of women from the urban areas are assisted by doctors during childbirth while only 3.5% of women are assisted by doctors during childbirth in the rural areas.
Child Health Care Utilization
Immunization
The use of Bed Nets
Measure differences in utilization due to need for health care) (Need and non-need variables).

Access Issues to Maternal and Child Health Care in Nigeria
Policies and Programs for Maternal and Child Health Care in Nigeria
Recent Innovations to Improve Maternal and Child Health Care Utilisation in
In addition to the free antenatal and free immunization provided in public hospitals, there are other innovative practices that have improved the utilization of maternal and child health care. Others are non-governmental organizations such as churches, charities and philanthropists who provide free access to vaccinations for children in churches, schools and rural areas. These innovations increase the offer of maternal and child health care especially to less privileged people.
It consists of four sections; part one articulates the conceptual issues of equality/inequality, part two contains the theoretical literature, part three focuses on the empirical literature, while part four presents the methodological literature. Sections two, three and four are written to address theoretical, empirical and methodological issues related to the two objectives stated in chapter one.
Conceptual Literature
- Concept of Equity and Inequity
- Types of Equity in Health Care
- Definition of Need in Health Care Utilization
- Why equity in Health Care?
Studies on equity in health care delivery have a unanimous definition on the topic of horizontal equity. Allin (2006) and Ong et al (2009) define horizontal equity in health care as equal treatment of equals. Allin (2006) defines vertical equity as a situation where individuals with different health care needs are treated differently while Ong et al (2009) view vertical equity as unequal but fair access to health care for unequal need.
However, vertical capital in healthcare is used exclusively in relation to its financing and not its use. This definition refers to the use of health care and its primary outcome, which is the improvement of health.
Theoretical Literature
- Economic Theory Relating to Equity/Inequity
- The Social Welfare Theory
- Theories of Resource Distribution and Equity in Social Welfare Theory
- The Maximin Theory (Theory of Justice as Fairness)
- The Utilitarian Theory of Welfare and Equity
- Equity/Inequity Theories in Health Care Utilisation
- The Social Welfare Model for Equity in Health Care Utilisation …
- The Social Welfare Model For Inequity Analysis By Gravelle et al (2006)
- The Social Welfare Model for Equity by Fleurbaey and Schokkaet (2009)
- Theoretical Literature on the Determinants of Health Care Utilisation…
- The Grossman Model (1972)
- Other Health Care Utilisation Models
- The Andersen Model
Theories of equity in health care are concerned with health care delivery and health care utilization. The model provides a comprehensive description of welfare optimization by policy makers in the utilization of health care by each member of society. Unfair inequalities or horizontal inequality in healthcare delivery are then related to the distribution of m in the population.
All theories except Anderson's do not clearly discuss the determinants of health care utilization. This theory is also focused on the psychological aspects of health care utilization without clearly describing the determinants.
Empirical Literature
Inequity in Maternal and Child Health Care Utilisation
Bonfruer et al (2012) investigate whether healthcare use meets needs in 18 sub-Saharan countries. Wirth et al (2008) find that in some cases urban housing shows the strongest and most significant use of maternal health care. Studies of child health care use also show similar dimensions of socioeconomic inequality in child health care use.
Schellenberg et al (2003) conducted a study of inequality among the very poor in health utilization in rural southern Tanzania. Mothers of children from wealthy families were more informed about their children's health risks and, as such, take their children to health centers when they are sick than poorer women.
Determinants of Maternal and Child Health Care Utilisation
Evidence from cross-sectional studies shows that the use of maternal health care varies within and between countries (Say and Raine, 2007). Socio-economic factors in the literature are related to income and education as they influence the use of maternal and child health care services. Adamu (2011) also identifies women's educational status as a strong predictor of maternal health care utilization.
Say and Raine (2007) show differences due to socioeconomic factors in the use of maternal health care among populations within and among 23 developing countries. Similarly, Jat et al (2011) analyzes the factors influencing the utilization of maternal health care services in the state of Madhya Pradesh, India.
Methodological Literature
Measurement of Inequity in Health Care Utilisation
- Direct and Indirect Standardisation
- Direct Standardisation
- Indirect Standardisation
- The Concentration Curve
- The Concentration Index
- The Structural Model
- Empirical Studies that Apply the Various Methods of Measuring Inequity in
- How is „Need‟ and Health care Utilisation Measured in the Empirical
Therefore, a complete picture is provided by using a concentration curve to measure inequality in healthcare utilization. The concentration curve is an important tool used by most health economists to measure inequality in the use of health services. Wagstaff et al (2003) demonstrated that the concentration index of a health variable is additively decomposable to the concentration indices of the determinants of that health variable.
Bonfruer et al (2012) measured socio-economic inequalities in health care use by means of a concentration index. Determinants unrelated to the need for health care use consist of marital status and occupational status.
Methodology on the Determinants of Maternal and Child Health Care Utilisation
- The Logit, Poison, Negative Binomial, and Two-part Model
- The Two-part Model
The logit model has been widely used to estimate the determinants of maternal and child health care utilization. The demand for healthcare depends on two decision processes; in the first stage the individual decides whether to use the health care services or not. In the second phase, the individual and the health care provider decide on the intensity of the use of the health care.
For use of healthcare services such as antenatal care, usually measured by number of visits, the use of negative binomial or poison regressions provides the appropriate method for estimations, as the number of antenatal visits is counted. The negative binomial regression model provides a better fit to health utilization than the binomial or poison models.
Lessons Learned from Literature Review and Value Additions of Reviewed
The introduction of religion into the theoretical framework to represent the role of responsibility is of additional value in this study. Others are regional analysis, variable interactions to trace the variable that have influence on the utilization pattern. The chapter consists of theoretical framework, empirical model specification, econometric techniques, data description and data sources.

Theoretical Framework
The Social Welfare Maximization Framework for Inequity Analysis
Theoretical Framework for Determinants of Health Care Utilization
- The Modified Grossman (1972) Demand for Health Care
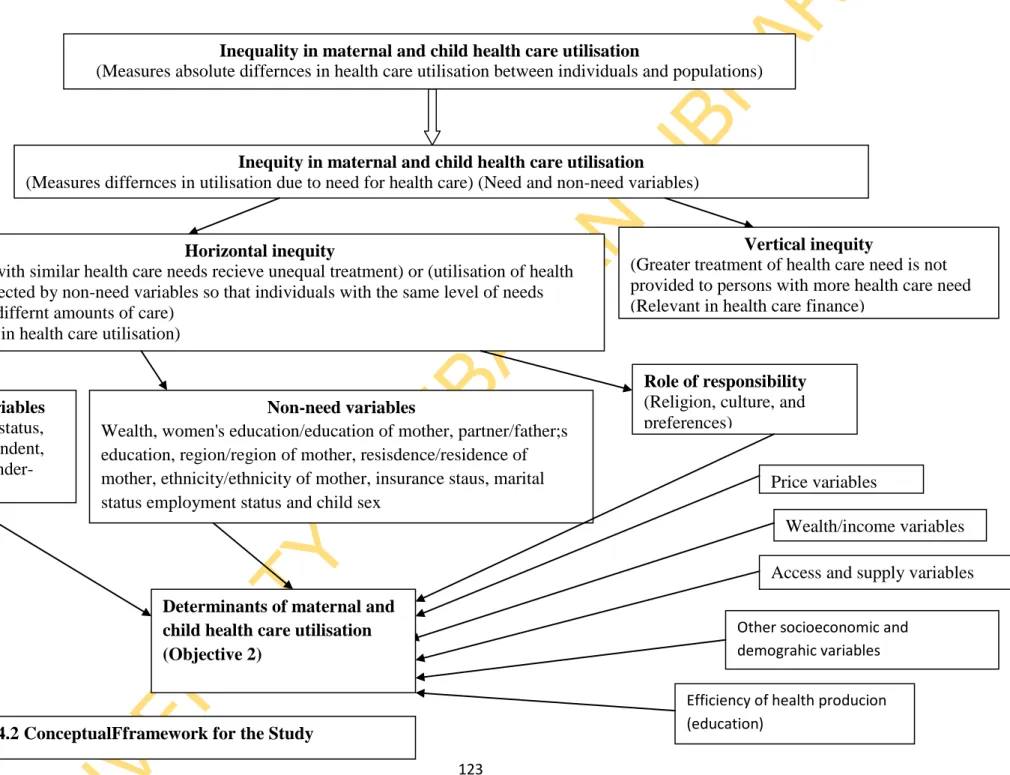
Conceptual Framework
The health services are;. antenatal care and skilled delivery, while the two child health care are; immunization and use of bed nets. The estimation of the empirical model for each of the health services is discussed in turn. The variable X stands for the non-need variables in the theoretical model that influence healthcare utilization.
The a priori expectation of child gender as a determinant of health care utilization is unclear. The second objective is presented in two parts; bivariate and multivariate analysis of determinants of maternal and child health care utilization. Maternal and child health care utilization improved from 1990 to 2013, based on information from the data.
This section discusses results on antenatal health care and skilled provision 5.2.1.1 Profile of inequality in the use of antenatal care.
Empirical Model of Estimation
Profile of Inequity in Maternal and Child Health Care Utilisation
Determinants of Maternal andCchild Health Care Utilisation
- Determinants of Maternal Health Care Utilisation
- Determinant of Child Health Care Utilization
Description of Theoretical Model, its Empirical Application and A priori
Variable Description and Measurement
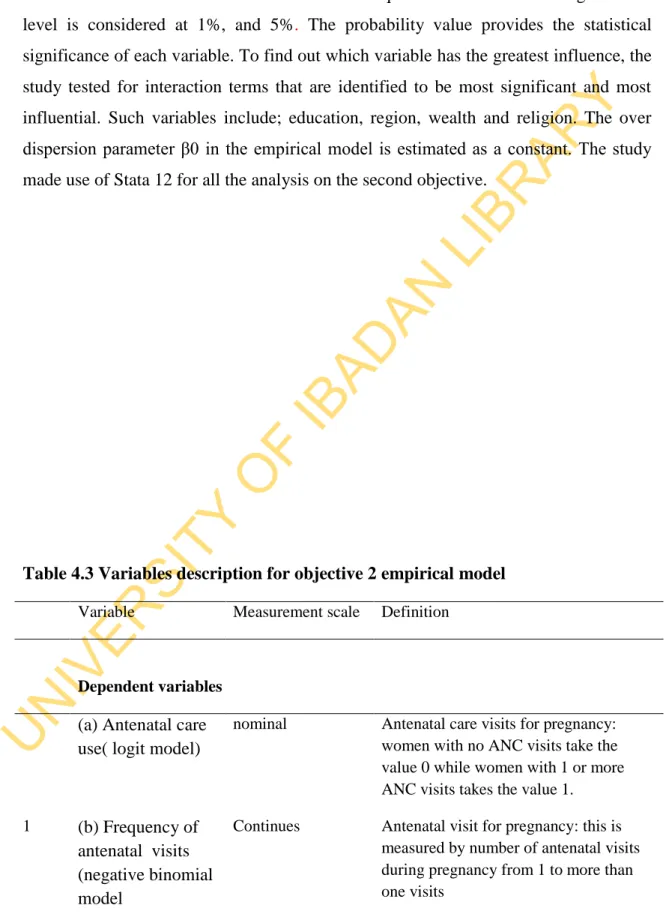
Most variables are nominally or discretely measured and require a qualitative regression modeling approach. Antenatal care use, the dependent variable, is measured in two forms to capture a two-part model. The first is the frequency of antenatal care visits, which is measured continuously; in this regard, a negative binomial model is used.
Antenatal care is measured on a nominal scale for model use and non-use of antenatal care through the logit model. North central, North East, North West, South East, South South, South West (Southwest is the reference category) 4 Residence Discrete Measured in dummies such as "Urban" and.
Data Requirement and Sources
The chapter contains the results for the analysis of the two stated objectives presented in three sub-sections. The first focuses on the descriptive statistics of all the variables used in the regression model. The second presents the results for the analysis of the first objective, while the third is for the second objective.
The result of the analysis for the first objective is presented using the concentration curves and the standardized concentration index.
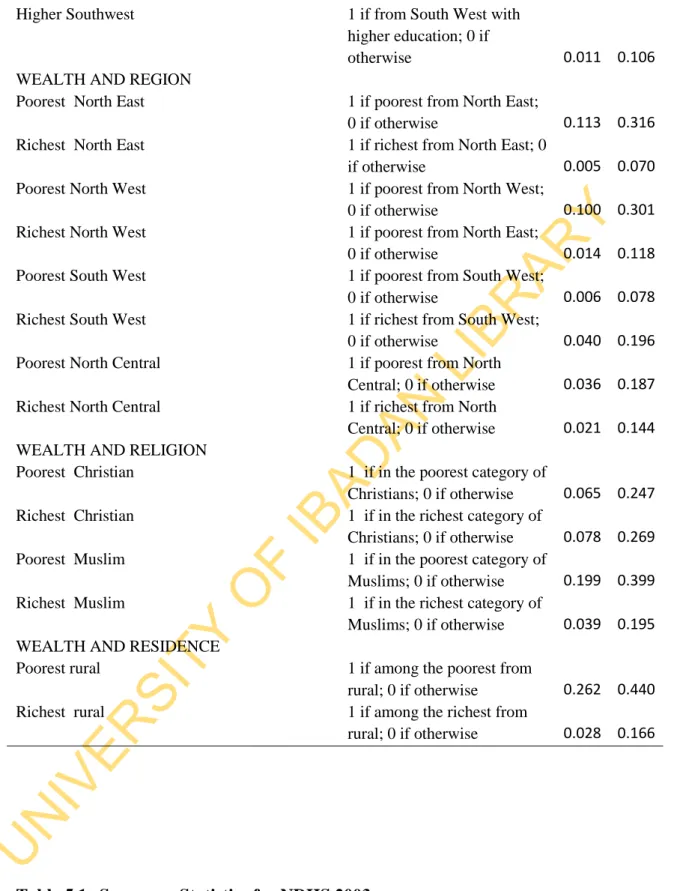
Summary and Descriptive Statistics
No education Northeast 1 if from the Northeast with no. education; 0 if otherwise Northeast Higher Education 1 if from Northeast with. No education North Central 1 if from North Central with. no education; 0 if otherwise Higher Education North Central 1 if from North Central with. No education Northwest 1 if from Northwest with no. education; 0 if otherwise Northwest Tertiary Education 1 if from Northwest with.
No education North Central 1 if from North Central with. no education; 0 if otherwise Higher Education North Central 1 if from North Central with. Without education North-East 1 if from North-East with no. education; 0 if otherwise Higher Education North-East 1 if from North-East with higher.
Profile of Inequity in Maternal and Child Health Care Utilisation
Profile of Inequity in Maternal Health Care Utilisation
- Profile of Inequity in Antenatal Care Utilisation
- Profile of Inequity in Skilled Delivery Care Utilisation
This section presents the concentration curve and horizontal inequality index results for the use of skilled delivery personnel for and 2013 in Figure 5.3. The results show that the skill supply concentration curves lie below the equality line with a positive horizontal inequality index. This implies that there is inequality in favor of the wealthy in the use of skilled delivery personnel during the four periods examined.
Similarly, need variables accounted for less than 1% of the factors driving qualified provision use for all four periods. Both health care services are used unequally in favor of the wealthy, however, the disparity in qualified provision is greater than the disparity in antenatal care when considering the results for e values.

Profile of Inequity in Child Health Care Utilisation
- Profile of Inequity in Immunisation Utilisation
- Profile of Inequity in Bed Nets Utilisation
Determinants of Maternal and Child Health Care Utilisation in Nigeria…
Bivariate Analysis of Determinants of Maternal and Child Health Care in
- Bivariate Analysis of Determinants of Antenatal Care Utilisation
- Bivariate Analysis of Skilled Delivery Utilisation in Nigeria
- Bivariate Analysis of Immunisation
- Bivariate Analysis of Bed Nets Utilisation
- Determinants of Maternal Health Care Utilisation in Nigeria
- Determinants of Child Health Care utilization
Discussion
Inequity in maternal and child health care utilisation
Determinants of Maternal and Child Health Care Utilisation in Nigeria…
Contribution to Knowledge
Conclusions
Recommendations
Limitations of the Study and Further Research
Regional Regression Results for Antenatal Care utilisation
Regional Regression Results for Skilled Delivery Utilisation








