I have the utmost respect for you as an oral health advocate, researcher, mentor, educator and, most importantly, as a friend. The Health Impact Pyramid informed the study on the impact of various oral health initiatives. Future public policy and programming to reduce disparities in the oral health status of vulnerable populations should be guided by The Health Impact Pyramid.
Consideration should be given to the use of mid-level oral health care and allied health care providers in alternative practice settings. Keywords: Allied health care, alternative care settings, dental caries, early childhood caries, access study framework, mid-level oral health care providers, Nova Scotia, oral health disparities, social determinants of health, health impact pyramid, vulnerable population. Oral health encompasses the health of the teeth, tissues, and orofacial system that enables facial expression, verbal communication, and chewing (CDC, 2016a).
Introduction
Current oral health policy initiatives in Nova Scotia may not address these disparities. The use of oral health care services is strongly related to the ability to pay (Ravaghi, Quinonez, & Allison, 2013a). This study confirms the negative impact on children's oral health due to the.
This award-winning program focused on school-based delivery of oral health care for children by allied dental professionals (Marchildon, 2011). Prior to the inception of this children's insurance program, Nova Scotia provided oral health care services to rural areas. The Children's Oral Health Program (COHP) is a public insurance program provided by the Nova Scotia Provincial Government and has acted as the payer of last resort since 2002 (Oral Health Advisory Group, 2015; Province of Nova Scotia Department of Health and Wellness, 2016a).
However, oral health disparities existed for vulnerable populations regardless of provider (dentist vs. dental therapist). The purpose of this study is to add to the limited knowledge on oral health of children in Nova Scotia.
Theoretical Frameworks
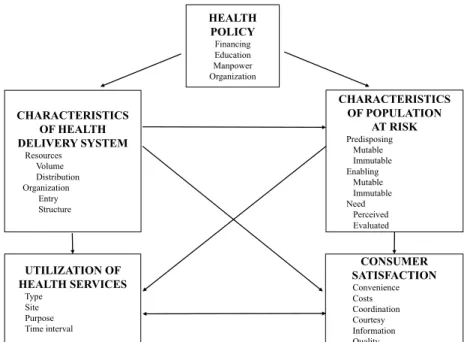
The basis of the Access Study Framework is the effect of health policy on changing access to care. Policy-led public oral health care includes direct delivery, public funding of private delivery, health promotion and fluoridation (Rowan-Legg, 2016). The province of Nova Scotia's oral health policy is largely public funding of private provision of oral health care for children.
The term characteristics of the health delivery system refers to the characteristics of the provision of health care services including resources and organization. Resources are the volume and distribution of human and tangible resources dedicated to health care. Organization refers to how resources are organized to provide health care (Aday & Andersen, 1974).
The ability of an individual or community to obtain health services is called enabling. This includes available resources, such as income and insurance, and the availability of health services in the community, such as differences in rural and urban access. The use of health services is based on several factors: type, location, purpose and time.
Time interval encompasses the process of accessing health care and the ability to continue using such services on an as-needed basis (Aday & Andersen, 1974). This element is best identified with consumers' past experiences with healthcare; and their perception of convenience, cost, coordination, politeness, information and quality. Did the health care professionals provide the information necessary to manage or treat the disease or condition?
Also, there is a dependence on individual behavior to affect health change at levels toward the top of the Health Influence Pyramid.
Method/Methodology
Additional questions were developed using the Aday and Andersen (1974) framework to meet the objectives of this study, and the specificities of oral health care in Nova Scotia and at the IWK Health Centre. Children with unmet dental needs who seek care at the IWK Dental Clinic are a subpopulation of the. To avoid coercion, mention of the gift certificate and the draw followed the participant's involvement in the study.
The eighth grade reading level was recommended by the IWK Health Center Research Ethics Board (REB). They kept records of the number of participants who were invited to participate in the study and the number of participants who agreed to participate. In addition, correspondence with members of the IWK Health Center team or research committee was documented.
The first manuscript 'Unmet Dental Needs Among Children and Barriers to Seeking Care' describes the background, objectives, method, results and discussion of the study. Improving access and provision of preventive oral care for very young, poor and low-income children through a new interdisciplinary partnership. Retrieved from FDI World Dental Federation: http://fdiworldental.org/oral-health/vision-2020/fdis-definition-of-oral-health.aspx.
Oral health disparities and unmet dental needs among preschoolers in Chelsea, MA: Exploring mechanisms, defining solutions. Oral health care for children in countries where dentists are used in public school programs, as opposed to those in the United States, where dentists are used in a private practice model. Nova Scotia Fluoride Mouthwash Program Ad Hoc Fluoride Mouthwash Review Committee, Report of the Criteria Subcommittee.
Effectiveness of an alternative dental workforce model on the oral health of low-income children in a school setting.
Manuscript 1
The most recent publication in a peer-reviewed journal on the oral health status of children in Nova Scotia is Ismail and Sohn (2001). The aim of this cross-sectional descriptive study is to contribute to the limited body of knowledge about children's oral health in Nova Scotia. In a recent report to the Minister of Health and Wellbeing, the Oral Health Advisory Group (2015) proposed 11 recommendations to improve the COHP.
This study focuses on the barriers to oral health care; the profile of both carer and the child seeking dental care at the Izaak Walton Killam (IWK) Health Centre; and the perception of oral health care in Nova Scotia. Difficulty in seeking oral health care for both their children and themselves was experienced by 45.8% of caregivers. The most common barriers to seeking oral health care for children were cost (17.7%), lack of cooperation by the child (16.1%) and inability for the caregiver to miss work (9.7%).
The most common barriers to healthcare providers seeking oral care on their own are cost (35.5%), no insurance, or uncertain insurance coverage (14.5%). Although the results of this study show oral health differences in a subset of children in Nova Scotia, the results of this study may not be generalizable. The evidence speaks to the need to facilitate early oral health screening, education, and intervention for children and their caregivers.
The barriers identified in this study clearly indicate that the financial burden of oral health care is a concern and a barrier to care for caregivers and their children, regardless of public insurance. The unique needs of this population must be considered in the provision of oral health services. It is clear that differences in income, education and geography affect oral health and exist among children and their caregivers in Nova Scotia.
Summary report of the results of the oral health component of the Canadian health survey 2007-2009.
Manuscript 2
This recent publication (Ismail and Sohn, 2001) in a peer-reviewed journal on the oral health status of children in the province of Nova Scotia analyzed data from a 1995-1996 cross-sectional survey of first grade children in Nova Scotia. Reduction of the inequalities in the oral health status of the socio-economically disadvantaged must be addressed. Public policy can be redirected to focus not only on reducing disparities in access to care, but also on reducing disparities in the oral health status of the socioeconomically disadvantaged.
The Health Impact Pyramid (2010) guides oral health prevention strategies to reduce oral health inequalities (Sheiham et al., 2011). Current Nova Scotia Children's Oral Health Survey research is needed to determine the impact of the COHP on improving the oral health status of a vulnerable population. Evidence suggests that direct provision of dental care, integration of oral health into primary care, and use of mid-level oral health care providers can reduce
Services provided in school and community programs can improve the oral health status of low-income children who would not otherwise receive care (CDA, 2010; Divaris et al., 2014) suggested that interprofessional collaboration with allied health care as a successful model to address socioeconomically unmet oral health care needs. Integrating oral health services into primary care facilitates screening and referral to a dental home, parent counseling, and application of fluoride varnish for vulnerable populations (Pahel et al., 2011).
Dental hygienists who provide oral health services in school settings have improved the oral health status of low-income children (Sen et al., 2013; Siegal & Richardson, 2010; Simmer-Beck et al., 2015). The dental hygienists' services improved the oral health status of low-income children who would not otherwise receive care. For many Nova Scotians, the oral health system is working well and rates of oral disease continue to decline.
Although the publicly funded, privately delivered oral health care model is failing the children most in need of preventive dental care (CAHS, 2014;. The realities of vulnerable populations and evidence-based oral health strategies are disconnected from current decision-making. Stakeholders and policy makers are encouraged to shift the perspective to an approach that offers high-impact oral health strategies to reduce oral health inequalities in vulnerable populations.
