APLICACIONES CLINICAS Dr. Marcos Young R.
PSA
—HISTORIA
—Ablin en 1960 reportó la existencia de proteínas en el semen
—Hara et al, en el Japanese Journal of Legal Medicine, 1971, identifica proteína en el semen, la llama Gama seminoproteína. Investigaban una sustancia para evaluar a víctimas de violación.
—En 1973, Li y Beling, identifican y purifican ésta proteína
—En 1978, Sensabaugh, caracterizó su naturaleza semen-específica, la denominó P30.
PSA
— En 1979, Wang aísla proteína específica de tejido prostático y la llama Antígeno prostático específico (PSA o APE), luego demuestra que es inmunológicamente idéntica a las proteínas de Hara y Sensabaugh
—Papsidero desarrolla prueba serológica para su detección en 1980.
—En 1987, Stamey publica en NEJM, su uso como marcador tumoral en el ACAP
PSA
—CARACTERISTICAS
—PM: 33 kd
—Glicoproteína de 237 aa, 4 cadenas de carbohidratos y múltiples puentes disulfuros
—Miembro de kalicreínas: hK-3
—Hay kalicreínas plasmáticas y tisulares
—Serina proteasa neutra
—Actividad similar a proteasas sanguíneas envueltas en proceso de coagulación
—Rol de las proteasas en proceso de coagulación ha sido estudiado extensamente
Yousef, G. M. et al. Endocr Rev 2001;22:184-204
PSA
PSA
—CARACTERISTICAS
—Cromosoma 19 q13.4
—Secuencia reconocida y completada
— Expresión regulada y mediada por receptor
androgénico
—Actividad de substrato similar a quimotripsina
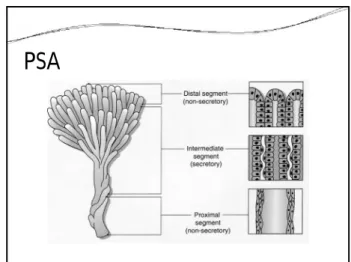
—Actúa sobre la seminogelina I, II, produciendo la licuefacción del gel espermático
PSA
PSA
The DNA and derived amino acid sequence of human prostase
Nelson P. S. et.al. PNAS;1999;96:3114-3119
©1999 by The N ational Academ y of Scienc es
Copyright ©2006 American Association for Cancer Research
Severi, G. et al. Cancer Epidemiol Biomarkers Prev 2006;15:1142-1147
Figure 2. Circulating levels of PSA by genotype (PSA gene) in 733 controls Androgen regulation of prostase expression
Nelson P. S. et.al. PNAS;1999;96:3114-3119
Copyright ©2001 The Endocrine Society
Yousef, G. M. et al. Endocr Rev 2001;22:184-204
COMPARACION DE ACTIVIDAD DE KALICREINAS
Emami, N. et al. J. Biol. Chem. 2008;283:19561-19569
ESQUEMA DE CASCADAS DE KALICREINAS EN SEMEN
Michael, I. P. et al. J. Biol. Chem. 2006;281:12743-12750
Human kallikrein physiology and pathobiology in the prostate
PSA
Emami, N. et al. J. Biol. Chem. 2008;283:19561-19569
Copyright © American Society of Clinical Oncology
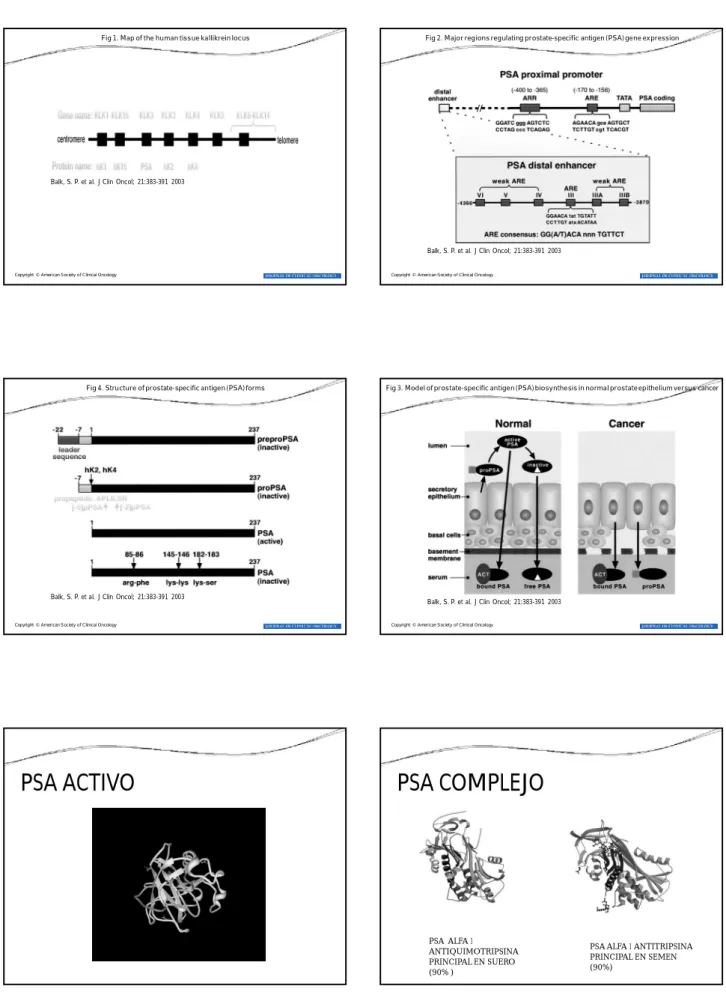
Balk, S. P. et al. J Clin Oncol; 21:383-391 2003
Fig 1. Map of the human tissue kallikrein locus
Copyright © American Society of Clinical Oncology
Balk, S. P. et al. J Clin Oncol; 21:383-391 2003
Fig 2. Major regions regulating prostate-specific antigen (PSA) gene expression
Copyright © American Society of Clinical Oncology
Balk, S. P. et al. J Clin Oncol; 21:383-391 2003
Fig 4. Structure of prostate-specific antigen (PSA) forms
Copyright © American Society of Clinical Oncology
Balk, S. P. et al. J Clin Oncol; 21:383-391 2003
Fig 3. Model of prostate-specific antigen (PSA) biosynthesis in normal prostate epithelium versus cancer
PSA ACTIVO
PSA COMPLEJO
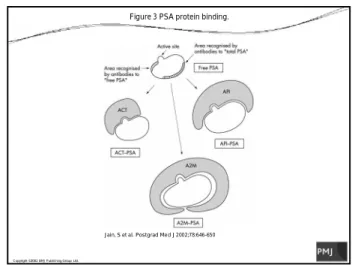
PSA ALFA 1 ANTIQUIMOTRIPSINA PRINCIPAL EN SUERO (90% )
PSA LIBRE Y ALFA 2 MACROG
PSA LIBRE
PSA CON ALFA 2 MACROGLOBULINA NO ES DETECTADA
NO EXPONE EPITOPES
Copyright ©2002 BMJ Publis hing Group Ltd.
Jain, S et al. Postgrad Med J 2002;78:646-650
Figure 3 PSA protein binding.
PSA
PSA –MARCADOR TUMORAL
—PSA—Herramienta para el diagnóstico y seguimiento de pacientes con ACAP
—ES ORGANO ESPECIFICO- NO ES CANCER ESPECIFICO
—Vida media: 2.2 a 3.2 días
—Aclaramiento después de PRR en 3 semanas
—Variabilidad entre pruebas previo a consenso:
—Estandarización
—Almacenamiento
— Límite inferior de detección actual : 0.003 ng/ml
PSA MARCADOR TUMORAL
—AFECTADO POR
—EDAD
—INFECCION
—TRAUMA
—TR VS MASAJE PROSTATICO
—MANIPULACION
—HPB
—MEDICAMENTOS: FINASTERIDE, OTROS
—MASA CORPORAL
PSA Y OBESIDAD
PSA MARCADOR TUMORAL
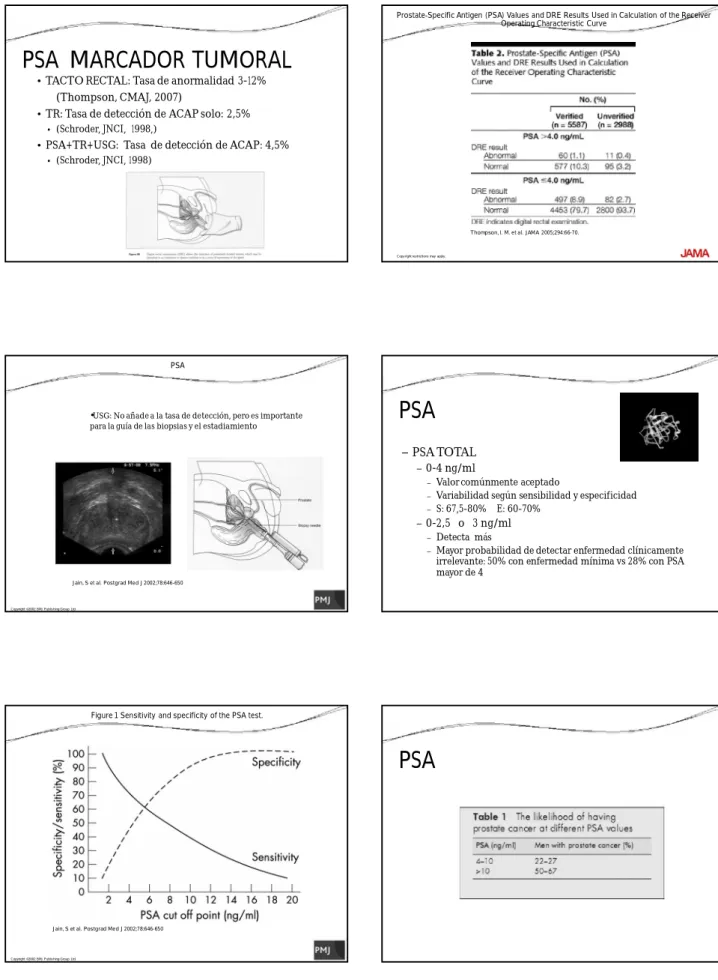
• TACTO RECTAL: Tasa de anormalidad 3-12% (Thompson, CMAJ, 2007)
• TR: Tasa de detección de ACAP solo: 2,5%
• (Schroder, JNCI, 1998,)
• PSA+TR+USG: Tasa de detección de ACAP: 4,5%
• (Schroder, JNCI, 1998)
Copy right rest rictions may apply .
Thompson, I. M. et al. JAMA 2005;294:66-70.
Prostate-Specific Antigen (PSA) Values and DRE Results Used in Calculation of the Receiver Operating Characteristic Curve
Copyright ©2002 BMJ Publis hing Group Ltd.
Jain, S et al. Postgrad Med J 2002;78:646-650
PSA
•USG: No añade a la tasa de detección, pero es importante
para la guía de las biopsias y el estadiamiento
PSA
—PSA TOTAL
—0-4 ng/ml
—Valor comúnmente aceptado
—Variabilidad según sensibilidad y especificidad
—S: 67,5-80% E: 60-70%
—0-2,5 o 3 ng/ml
—Detecta más
—Mayor probabilidad de detectar enfermedad clínicamente irrelevante: 50% con enfermedad mínima vs 28% con PSA mayor de 4
Copyright ©2002 BMJ Publis hing Group Ltd.
Jain, S et al. Postgrad Med J 2002;78:646-650
Figure 1 Sensitivity and specificity of the PSA test.
Copy right rest rictions may apply .
Thompson, I. M. et al. JAMA 2005;294:66-70.
Receiver Operating Characteristic Curve for Prostate-Specific Antigen (PSA)
PSA
—DERIVADAS DE PSA: “PSA KINETICS FACTORS ” OR
“PSA DYNAMICS” —PSA SEGÚN EDAD
—VELOCIDAD DEL PSA
—DENSIDAD DEL PSA, DENSIDAD DEL PSA EN ZT
—PSA LIBRE, PSA COMPLEJO
—TIEMPO DE DOBLAJE DEL PSA (PSA DT)
PSA-RANGOS POR EDAD
VELOCIDAD DEL PSA
CARTER(1992): CAMBIO DE 0,75 NG/ML/AÑO S: 72% E: 95%
DENSIDAD DEL PSA
BENSON (1992):
PSA/ VOL DE PROSTATA POR USG VALOR DE 0.15
PSA LIBRE
—Mayor valor con PSA entre 4 y 10
—Relación de Libre/Total
—No tiene utilidad en el estadiamiento
PSA DT
PSA DT
PSA DT
PSA DT
PSA
PSA
—PSA DT Y PSA V MAS DE 2 ng/ml/año:
SEGUIMIENTO, D´Amico
—DERIVADAS DEL PSA: MAYOR UTILIDAD EN EL
¿Aliado o Villano?
PSA
PSA
PSA
PSA –TUMORES EN PANAMA
AMBOS SEXOS
PSA-MORTALIDAD-AMBOS SEXOS
PSA-MORTALIDAD HOMBRES
PSA
PSA
PSA
0 50 100 150
Eastern Asia South Central AsiaNorthern Africa South-Eastern AsiaWestern Asia Eastern Africa Eastern EuropeWestern Africa Middle AfricaWorld Central America Southern EuropeSouthern Africa South AmericaCaribbean Northern EuropeWestern Europe Australia/New ZealandNorthern America
Rate per 100,000 Incidence Mortality
Figure 2.2: Age-standardised* incidence and mortality rates for prostate cancer by world regions, 2002 estimates
PSA
0 100 200 300 400 500 600 700 800 9001 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 CASOS CASOS 1993
PSA
PSA
0 50 100 150 200 250 300 3501 2 3 4 5 6 7 8 9 10 11 12 13 14 1516 17 18 192021 2223 DEF DEF
PSA
0 100 200 300 400 500 600 700 800 9001 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 CASOS VS DEFUNCIONES
DEF CASOS
PSA
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.81 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 LETALIDAD
LETALIDAD
PSA
—CANCER DE PROSTATA
—ENIGMA EPIDEMIOLOGICO
—SOBREDETECCION VS DX TEMPRANO
—Sobredetección: habilidad de una prueba de screening de identificar una condición qu de otra manera hubiese permanecido indolente y no causar morbilidad en el paciente . Evidentemente va ligado al SOBRETRATAMIENTO
—Riesgo de padecer cáncer de próstata en la vida: 16%
—(Ryes 2008)
—Riesgo de muerte por cáncer de próstata: 3,4%
PSA
PSA
Copyright ©2009 American Cancer Society
From Brawley, O. W. et al. CA Cancer J Clin 2009;59:264-273.
FIGURE 3 Proportion of Cancers Fulfilling Histologic Criteria for Clinical Significance and Incurability by Prostate-specific Antigen (PSA) Level at Diagnosis
PSA
Copyright ©2009 American Cancer Society
From Brawley, O. W. et al. CA Cancer J Clin 2009;59:264-273.
FIGURE 2 Risk of Prostate Cancer and Risk of High-grade Disease by Prostate-specific Antigen (PSA) Level (Based on the Placebo Group of the Prostate Cancer Prevention Trial)
PSA
PSA
PSA
PSA
PSA
PSA
PSA
PSA
PSA
PSA
PSA
PSA
PSA
PSA
Cáncer de próstata tiene historia natural larga: requiere seguimiento de gran población en un período prolongado
PSA
PSA
PSA
0 100 200 300 400 500 600 700 800 900
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 CASOS VS DEFUNCIONES
DEF CASOS
PSA-P. RADICAL.
CSS.CHMDRAAM.2009
ENERO 13
FEBRERO 5
MARZO 19
ABRIL 13
MAYO 13
JUNIO 16 6m 79
JULIO 15 7m 84
1985-1990 6a 13
1991-1994 4a 32
1994-1996 3a 45
PSA
PSA
PSA
PSA Y DETECCION
TEMPRANA-RECOMENDACIONES AUA 2009
— DEBE OFRECERSE PSA Y TR
— UNA VARIEDAD DE FACTORES AFECTAN LOS NIVELES DE PSA
— UNA BIOPSIA DE PROSTATA CONFIRMA LA PRESENCIA DE CANCER
— EL NIVEL DE PSA EN SANGRE PREDICE LA EXTENSION DE LA ENFERMEDAD
— LA DECISION DE PSA DEBE SER INDIVIDUALIZADA — DEBE INFORMARSE AL PTE. DE LOS RIESGOS Y BENEFICIOS — PSA DEBE OFRECERSE A MAYORES DE 40 AÑOS O MAS O
AQUELLOS PTES. QUE LO SOLICITEN
— EN CASO DE SER POSITIVA LA BIOPSIA, DEBE DISCUTIRSE TODAS LAS OPCIONES DE TRATAMIENTO
PSA Y MAS DE 75 AÑOS
PSA
—http://deb.uthscsa.edu/URORiskCalc/Pages/calcs.jsp
PSA
PSA
—PSA TIENE FUNCIONES EN REPRODUCCION MASCULINA
—PSA ES ORGANOESPECIFICO, NO CANCER ESPECIFICO
—DEBE INFORMARSE AL PACIENTE
—USO EN DETECCION TEMPRANA ES DE DEBATE EN SALUD PUBLICA.
—USO EN PTES. MENORES DE 75 AÑOS, CON EXPECTATIVA DE VIDA DE MAS DE 10 AÑOS