Case finding or clinical investigation: In the context of intimate partner violence, this refers to the identification of women experiencing violence who present to a health facility using questions based on the presence of the condition, history and, where appropriate, examination. the patient. Vicarious trauma: defined as the transformation of the health care provider's internal experiences as a result of empathy and/.

Introduction
Target audience
Some recommendations relied partially on existing guidelines and assessed the quality of evidence in those guidelines. Where no evidence was found for a clinical or health policy recommendation, this was indicated in the evidence summary.
Summary of recommendations
- Women-centred care
- Identification and care for survivors of intimate partner violence
- Clinical care for survivors of sexual assault
- Emergency contraception
- HIV post-exposure prophylaxis
- Post-exposure prophylaxis for sexually transmitted infections 19 Women survivors of sexual assault should be offered
- Psychological interventions
- Interventions from 3 months post-trauma 28 Assess for mental health problems (symptoms of acute
- Training of health-care providers on intimate partner violence and sexual assault
- Health-care policy and provision b
- Mandatory reporting of intimate partner violence a
Training of healthcare providers in intimate partner violence and sexual assault violence and sexual assault. 30 Training at pre-qualification level in first-line support for women who have experienced intimate partner violence and sexual assault (see recommendation 1) should be provided to health professionals (especially doctors, nurses and midwives).
Background
Thus, the guidelines focus on intimate partner violence and sexual violence against women and provide health care providers with evidence-based guidance on how to better identify and respond to women who report experiencing violence. The guidelines also, for the first time, provide guidance on in-service training on intimate partner and sexual violence against women for health care providers and other members of multidisciplinary teams.
Scope of the guidelines
Responding to intimate partner violence and sexual violence against women: WHO Human Rights clinical and policy guidelines supporting the guidelines. International and regional human rights bodies have provided guidance on the contribution that health professionals can – and should – make to ensuring women's freedom from gender-based violence and ensuring an appropriate response when such violence occurs.
Identifying, appraising
Recruitment of the Guideline Development Group
Responding to Intimate Partner Violence and Sexual Violence Against Women: WHO Clinical and Policy Guidelines Prospective GDG members were selected based on their contribution to the field, as well as the need for regional diversity and area of expertise. . As a respected researcher in the field, the chair was selected for his extensive experience of guideline development methodology and chairing guideline development groups. Potential GDG members were identified, in part, by attendees at the 2009 meeting who were asked to submit a personal statement and complete the WHO Declaration of Interest form.
Declaration of interest by Guideline Development
Decision-making during the Guideline Development Group
These were recommendation 2 regarding 'universal screening' and recommendation 7 regarding advocacy/support/empowerment for intimate partner violence.). The topic reviewer and WHO staff were exempted from voting, and voting was done by WHO regional staff who were invited as consultants. In these two cases, the minority opinion is recorded in the discussion or comments in the appropriate column.
Document preparation and peer review
Evidence and recommendations
Recommendation
-Healthcare providers should work with the women, presenting options and possibilities and providing information, with the goal of developing an effective plan and setting realistic goals, but the woman should always be the one making the decisions. D). In some situations, such as emergency rooms, as much as possible should be done during the first contact, in case the woman does not return. Follow-up support, care and negotiation of safe and accessible means for follow-up consultation should be offered. e) Health care providers need to understand the gendered nature of violence against women, and the human rights dimension of the problem. f) Women with a physical or mental disability are at increased risk of intimate partner violence and sexual violence.
Identification and care for survivors
- Identification of intimate partner violence
- evidence summary
- from evidence to recommendations
- Recommendations
- Care for survivors of intimate partner violence
- Psychological/mental health interventions
- Advocacy/empowerment interventions
- mother–child interventions evidence summary
- Other interventions
There is strong evidence of a link between intimate partner violence and mental health disorders among women. What effects do interventions initiated by health care providers have for women who are survivors of intimate partner violence?”. There is insufficient evidence to recommend CBT for women who continue to experience intimate partner violence.
There was insufficient evidence to recommend a group psychological intervention for women who have experienced intimate partner violence. Responding to Intimate Partner Violence and Sexual Violence against Women: WHO Clinical and Policy Guidelines Note:. Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines Figure 1.
Clinical care for survivors of sexual
- Interventions during the first 5 days after the assault
- emergency contraception
- HIv post-exposure
- Post-exposure prophylaxis for sexually transmitted infections
- Psychological/mental health interventions
- Interventions during the first days after the assault
- Interventions up to 3 months post-trauma
- Interventions from 3 months post-trauma
- general remarks
The strength of evidence in the following recommendations is based on the best assessment of the evidence provided in the reviewed guidelines. Two of the four studies used prospective double follow-up study designs to compare HIV seroconversion among sexual assault survivors prescribed HIV PEP with sexual assault survivors not prescribed HIV PEP (Drezett , 2002; Garcia et al., 2005). A search of the scientific literature did not identify any studies examining the effects of STI PEP provided by health care providers to women survivors of sexual assault.
Comparison of the CDC and FIGO guidelines on this topic revealed that they are in general agreement. A search of the scientific literature identified nine studies that examined the effects of mental health interventions delivered by health care providers to women survivors of sexual assault, with one of these studies meeting all criteria of the PICOT question (Echeburua et al., 1996) and eight of these studies (Rothbaum, 1997; . Since many sexual assault survivors have these types of problems, the generalizability of the findings of these studies to the larger population of sexual assault survivors may be open to were questioned.
Training of health-care providers on intimate
- evidence summary
- training interventions for intimate partner violence
- training interventions for sexual assault
- from evidence to recommendations
- Recommendations
- general remarks
Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidance Figure 2.32 Training for healthcare providers on intimate partner violence and sexual violence should cover various aspects of responding to intimate partner violence and sexual violence (e.g. safety assessment and planning, communication and clinical skills, documentation and provision of referral pathways). The GDG agreed that training of health care providers in intimate partner violence and sexual violence should be added to the primary education curriculum and at least offered in the form of continuing education for those health care providers most likely to work with women come into contact.
30 Health care providers (especially doctors, nurses and midwives) should be provided with pre-qualified training as the first line of support for women who have experienced intimate partner violence and sexual assault (see recommendation 1). Responding to intimate partner violence and sexual violence against women: clinical and policy guidelines WHO Notes. 33 Intimate partner violence and sexual assault training should be included in the same program, given the overlap between the two topics and the limited resources available to train health care providers on these issues.
Health-care policy and provision
- evidence summary
- from evidence to recommendations
- Recommendations
- general remarks
Training should include clinical screening and care for intimate partner violence and sexual assault, as well as attention to cultural competence, gender equality and human rights considerations. In general, there is a lack of robust evaluations of the effectiveness of health system interventions for intimate partner violence and sexual assault. Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines in health care settings, only four studies (Derhammer et al., 2000; Crandall et al., 2003; Kim et al. ., 2009; Sampsel et al., 2009; al., 2009) were identified that focused on this.
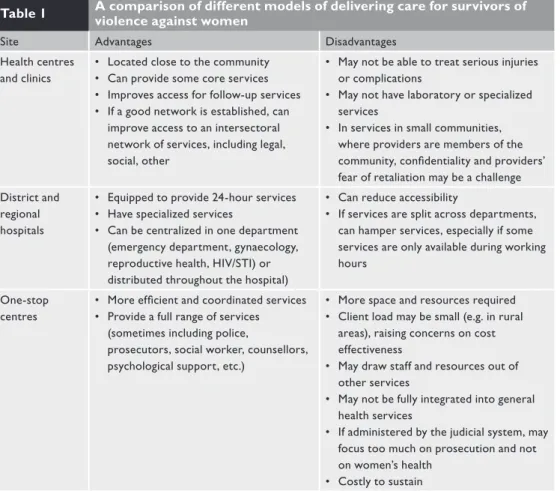
Which sectors of the health care system (eg, emergency department, primary care, antenatal care or other sexual and reproductive health services, HIV counseling and testing) are better sites for interventions for women experiencing intimate partner violence or sexual violence. 34 Care for women who experience violence in intimate relationships and sexual assault should, as far as possible, be integrated into existing health services rather than as an independent offer (see box 3). Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines 35 A country needs multiple models of care for survivors of intimate partner violence and sexual assault at different levels of the health system (see Table 1, p. 37 ). .
Mandatory reporting of intimate partner
- evidence summary
- from evidence to recommendations
- Recommendations
- general remark
Quality of evidence: Very low Strength of recommendation: Strong 36 A healthcare provider (nurse, doctor or equivalent) who is trained in gender-sensitive treatment of sexual abuse and. If a restraining order/protection is in place and the partner is present at the health visit, the relevant authorities must be called. The evidence does not support mandatory reporting of intimate partner violence to the police because it may affect women's autonomy and decision-making.1 While some women recognize that there may be some benefit to taking legal action on their behalf, this does not appear to be the preference for abused women.
37 Mandatory reporting of intimate partner violence to the police by the healthcare provider is not recommended. However, healthcare providers should offer to report the incident to the appropriate authorities (including the police) if the woman wishes to do so and is aware of her rights. 38 Child abuse and life-threatening incidents must be reported by the healthcare provider to the relevant authorities, if there is a legal obligation to do so. A).
Research implications
Research gaps based on guideline questions
A randomized controlled trial to test whether or not treating Trichomonas would increase adherence to other drugs would provide useful information.
Dissemination and implementation of the guidelines
Guideline dissemination
Guideline implementation
Monitoring and evaluating
Updating of the guidelines
Annexes
Responding to intimate partner violence and sexual violence against women: clinical and policy guidance from WHO, World Health Organization. Increasing discussions about intimate partner violence in prenatal care using video doctors and health care providers: a randomized controlled trial. Reducing maternal intimate partner violence after childbirth: A randomized controlled trial of the Hawaii Healthy Start Home Visitation Program.
Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines Lieberman AF, Van HP, Ippen CG. The effects of expressive writing on pain, depression, and posttraumatic stress disorder symptoms in intimate partner violence survivors. Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines II.
Peer reviewers
List of full reviews and evidence tables
The standardized criteria used in evaluating the evidence and the GRADE tables are not included in this document. A list of separate documents is provided below (available on request from [email protected]).
WHO clinical and policy guidelines
