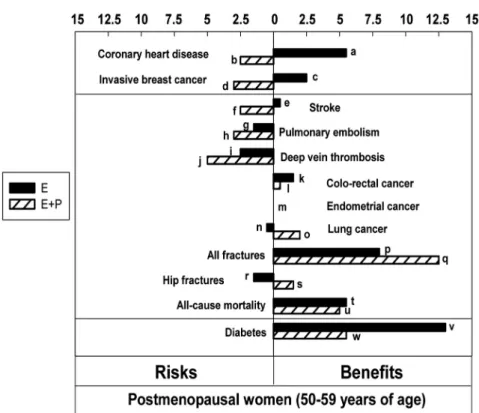
This guideline covers the entire spectrum of therapies to alleviate the most common and bothersome symptoms of menopause (Figure 1). Detailed management of the transition to early menopause, primary ovarian insufficiency, and prevention of osteoporosis and fractures is beyond the current scope.) The choice of therapy is ideally based on the available evidence of safety and efficacy and is generally a shared decision involving the patient and the provider. In summary, the risk of breast cancer from estrogen alone taken for 5 years appears to be small. In women aged 50 to 59 years in the WHI, the excess risk of invasive breast cancer during the intervention phase persisted 7 years after stopping EPT, with 4.5 excess cases/.
Combined EPT. The WHI trial found an association between EPT and GVT and pulmonary embolism (PE) in women aged 50 to 59 years (44). Metabolic syndrome. Metabolic syndrome (MetS) is associated with an increased risk of cardiovascular events and breast and colon cancer (146). The approximately 2-fold increased risk of VTE (both GVT and PE) with oral MHT is similar in low-, intermediate-, and high-risk women (149, 150).
There are no clear criteria for recommending (or avoiding) MHT based on a woman's breast cancer risk. Vasomotor symptoms. The number and severity of moderate to severe VMS were significantly reduced after 12 weeks; the frequency of hot flashes was reduced by 74% compared to 51% with placebo, and the severity of hot flashes was reduced by up to 54%. Breasts. The incidence of breast pain and tenderness was similar between CEE/BZA and placebo (185–187) and lower than CEE/MPA.
Breast and colon cancer. The incidence of breast tenderness is low (approximately) and neither mammographic density nor invasive breast cancer was in-.

Nonhormonal therapies for VMS
Depending on the severity of symptoms, women may choose to restart MHT, perhaps at a lower dose, or seek relief with non-hormonal therapy. However, bisphosphonates remain in the bone indefinitely, and most expert groups do not recommend starting bisphosphonate therapy for the prevention of osteoporosis in women aged 50 to 59 years. , increases with the duration of therapy.
Since hot flashes are caused by changes in the thermoregulatory neutral zone, removing layers of clothing, using fans, keeping the bedroom cool (30), avoiding alcohol and spicy food, and reducing stress can be effective. The interpretation of studies on the efficacy of hedetures requires an understanding of an important confounding factor. There is a strong, consistently reported placebo effect that averages 30% (range, 4–57%; Figure 4) and occurs more frequently in women with high anxiety and stress scores (215–220).
Clinical trials with paroxetine, venlafaxine, desvenlafaxine, citalopram and escitalopram demonstrate statistically significant efficacy with a reduction in hot flash frequency ranging from 25 to 69% (Figure 4). Other agents such as sertraline and fluoxetine are associated with non-statistically significant trends toward the reduction of hot flashes and inconsistent results (221-223). Meta-analyses and a Cochrane review concluded that SSRIs and SNRIs have mild to moderate effects in reducing hot flashes in women with a history of breast cancer.
Each of these agents appears to have similar effects in breast cancer survivors as in healthy postmenopausal women, although the studies are small. Choice of SSRI/SNRI vs gabapentin/pregabalin A randomized, crossover, multicenter trial comparing recommended doses of venlafaxine vs gabapentin, 300 mg three times daily (243), reported that both agents reduced hot flushes by 66%, but two-thirds of patients preferred venlafaxine over gabapentin. None of the RCTs established statistically significant superiority of one treatment regimen over another.
Clinical trials with these agents have reported efficacy inconsistent with placebo, but in individual patients. In a randomized study of 187 symptomatic menopausal women, clinical hypnosis was associated with a 74.2% reduction in hot flashes compared with 17.1%. Caution is advised because some of these agents, when consumed as supplements, may exert estrogenic effects, a concern in breast cancer survivors, although dietary soy appears to have no adverse effects on breast cancer prognosis (248).

Treatment of genitourinary syndrome of menopause
Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: a randomized controlled trial of the Women's Health Initiative. CAVE. Szmuilowicz ED, Manson JE, Rossouw JE, et al. Vasomotor symptoms and cardiovascular events in postmenopausal women. Menopause. Manson JE, Chlebowski RT, Stefanick ML, et al. Hormonal therapy in menopause and health outcomes during intervention and.
Lobo RA, Davis SR, De Villiers TJ, et al. Prevention of diseases after menopause. Climacteric. Bakken K, Fournier A, Lund E, et al. Menopausal hormone therapy and breast cancer risk: impact of different treatments. Chen WY, Manson JE, Hankinson SE, et al. Unopposed estrogen therapy and the risk of invasive breast cancer. Arch Intern Med.
Chlebowski RT, Anderson GL, Gass M, et al. Estrogen plus progestin and the incidence and mortality of breast cancer in postmenopausal women. JAMA. Anderson GL, Chlebowski RT, Rossouw JE, et al. Prior hormone therapy and breast cancer risk in the Women's Health Initiative randomized trial of estrogen plus progestin. maturitas. Chlebowski RT, Manson JE, Anderson GL, et al. Estrogen plus progestin and the incidence and mortality of breast cancer in the Women's Health Initiative observational study. J Natl Cancer Inst.
Steinauer JE, Waetjen LE, Vittinghoff E, et al. Postmenopausal hormone therapy: does it cause incontinence? Obstet Gynecol. Espeland MA, Rapp SR, Shumaker SA, et al. Conjugated equine estrogens and global cognitive function in postmenopausal women: Women's Health Initiative Memory Study.JAMA. Cushman M, Kuller LH, Prentice R, et al. Estrogen plus progestin and risk of venous thrombosis. JAMA.
Pinkerton JV, Harvey JA, Pan K, et al. Effects of bazedoxifene-conjugated estrogens on the breast: a randomized controlled trial. Obstet Gynecol. Cummings SR, Ettinger B, Delmas PD, et al. Effects of tibolone in older postmenopausal women. N Engl J Med. Kroenke CH, Caan BJ, Stefanick ML, et al. Effects of dietary intervention and weight change on vasomotor symptoms in the Women's Health Initiative. Menopause.
Rahn DD, Good MM, Roshanravan SM, et al. Effects of preoperative local estrogen in postmenopausal women with prolapse: a randomized trial. J Clin Endocrinol Metab. Van Patten CL, Olivotto IA, Chambers GK, et al. Effect of soy phytoestrogens on hot flashes in postmenopausal women with breast cancer: a randomized, controlled clinical trial. J Clin Oncol.