Correlation trend of quality of life and general health status. Caregivers of children with cerebral palsy over an. Cerebral palsy (CP) is one of the most crippling childhood disorders that seriously affects a child's development (Rosenbaum, 2003).
Statement of the Problem
Aims of Study
9 In the eight-month period, there would be no significant difference in the quality of life of caregivers of children with cerebral palsy. 10 There would be no significant difference in the general health status of caregivers of children with cerebral palsy over an eight-month period. Cerebral palsy (CP) has been defined as a group of developmental movement and postural disorders that cause activity limitations attributable to non-progressive disorders that occur in the developing fetal or infant brain (Bax et al, 2005).
This instrument (Appendix VIII) was developed by Boyd and Graham in 1999 and used in this study to assess selective motor control (SMC) in children with cerebral palsy in the clinic. There would be no significant difference between the quality of life of caregivers of children with cerebral palsy over an eight-month period. There would be no significant difference between the general health status of the caregivers of children with cerebral palsy over an eight-month period.
Use of gross motor function classification to optimize rehabilitation management of children with cerebral palsy. Assessment of the quality of life of mothers of children with cerebral palsy (primary caregivers).
Hypothesis
Delimitation
This study is delimited to the following subjects:. i) Children with cerebral palsy between 6 months and 6 years of age who presented at the Pediatric Neurology Clinic of the University College Hospital Ibadan, Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC). The environment for the study is delineated to the following:. i) The home of children with cerebral palsy (ii) Oni Memorial Children's Hospital. iii) Pediatric Gymnasium of each of the Department of Physiotherapy, University College Hospital Ibadan and Obafemi Awolowo University Teaching Hospitals Complex Ile-Ife. iv) Immunization Clinic of the University College Hospital Ibadan.
Significance of the Study
The GMFM was administered in the clinic and in the homes of children with cerebral palsy. Development and reliability of a system for classifying gross motor function in children with cerebral palsy.
Definition of Operational Terms
Definition
The motor deficits of cerebral palsy are often accompanied by several comorbid conditions, including epilepsy, learning disabilities, behavioral problems, and sensory deficits that are as important as the motor deficits (Rosenbaum, 2003).
Prevalence of Cerebral Palsy
Modified Tardieu Scale (MTS): The Modified Tardieu Scale (MTS) was used to assess spasticity in children with cerebral palsy. Bjornson KF, Graubert C, Mclaughan FC (1998): Test-retest reliability of the gross motor function in children with cerebral palsy .
Risk factors for Cerebral Palsy
Clinical Presentation of Cerebral Palsy
Classification of Cerebral Palsy
Cerebral palsy can be classified based on the topography of the affected body parts, the type of motor impairment involved, and the severity of the disorder. Using the type of motor impairment as a classification model, cerebral palsy can be described as spastic, ataxic, choreoathetoid, dyskinetic and dystonic types.
Management of Cerebral Palsy
It is based on the concept that children with motor disabilities learn in the same way as those without disabilities. The effectiveness of CE in improving the functional abilities of children with CP has not been proven by any controlled clinical research (Darrah et al 2004; Roth, 2004). The conductive education method is said to be as effective as conventional approaches, but not better than them. (Roth, 2004).
Motor Development
However, as a result of the pathology of damage to an immature brain, there is an alteration or delay in motor development among children with cerebral palsy (Rosenbaum, 2003). Schenker et al, 2005, in a study conducted on the participation of children with cerebral palsy in the school environment, found that functional performance is not an abstract set of skills unrelated to the environment in which the person lived, worked or walked.
Health of Caregivers
A study conducted on the mothers of children with Asperger Syndrome (AS) and High Functioning Autism (HFA) showed that they had lower SF-12 scores indicating poorer physical health than controls who were parents of apparently healthy age-matched children (Allik et al, 2006). Parents of children with Down syndrome experienced more caregiving problems, child-related stress (distractibility, demandingness, unacceptability) and parent-related stress (incompetence, depression, health problems, role limitation) than parents of typically developing children (Roach et al. al, 1999).
Quality of Life Caregivers of Patients with Neurological Disorders…30
Measurement of Motor of Function in Cerebral Palsy
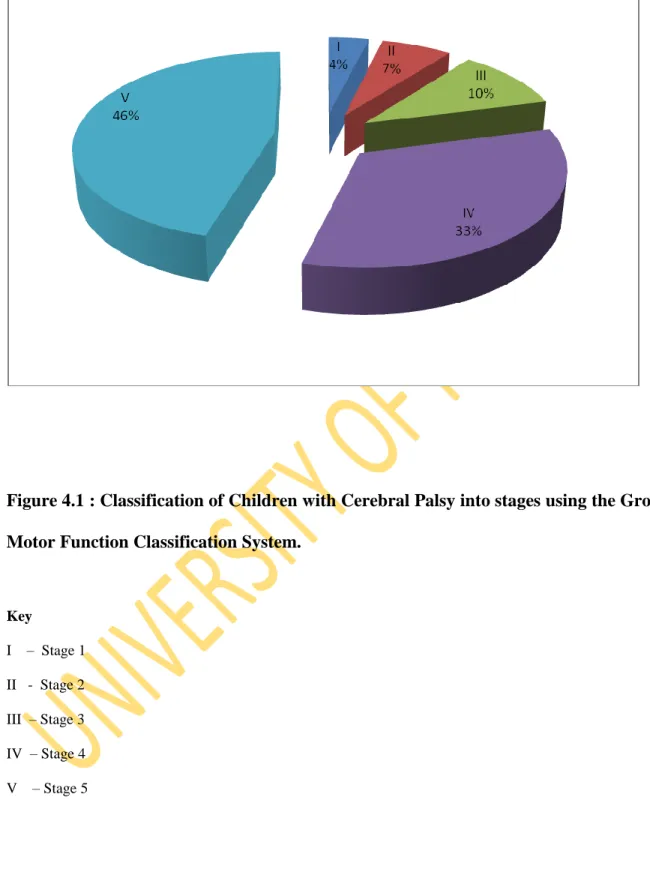
Examples include Gross Motor Function Classification System (GMFCS), Gross Motor Function Measure (GMFM), Bayley Scales of Infant Development for Cognitive Function (BSIDCF), Peabody Developmental Motor Scales (PDMS), Alberta Infant Motor Scale (AIMS), Pediatrics Evaluation Disability Inventory (PEDI). Gross Motor Function Classification System (GMFCS): The Gross Motor Function Classification System (GMFCS) was chosen by the researcher and used to classify children with cerebral palsy into their functional levels (Appendix ii). Gross Motor Function Measure (GMFM): The GMFM is a criterion-referenced measure constructed with the aim of evaluating changes in gross motor function in children with CP (Russel et al, 2000).
A total score is obtained by adding up the scores for all dimensions and dividing by 5 (ie the total number of dimensions).
Measurement of Quality of Life and General Health Status
Examples include the 36-item General Health Outcomes Study, the Brief Health Survey (SF-36), the General Health Questionnaire, etc. One hundred and seven children (64 males and 43 females) with cerebral palsy aged 1 to 6 years. were included in the study. Children with cerebral palsy who had concomitant neuromuscular or musculoskeletal diseases (eg, spinal bifida, muscular dystrophy, or myopathy) were excluded from the study.
17 primary caregivers of children with cerebral palsy who understood Yoruba or English participated in the study.
Materials
Instruments
The children met the inclusion criterion of a diagnosis of cerebral palsy made by a pediatrician and referred for physical therapy. To serve as controls for the CCWCP, 98 caregivers of age-matched children who did not have cerebral palsy and who could understand either Yoruba or English were recruited. It is a criterion-referenced measure constructed for the purpose of evaluating changes in gross motor function among children with CP (Russel et al, 1989).
General Health Questionnaire (GHQ): It was used to assess the general health status (Appendix iv) of caregivers of children with cerebral palsy and caregivers of children without cerebral palsy.
Methods
Sampling Technique and Sample Size
Research design
The study was a longitudinal study involving observation and repeated examination of gross motor function in children with cerebral palsy in the clinic and their respective homes over an eight-month period. The general health status and quality of life of caregivers of the same group of children with cerebral palsy and caregivers of typically developing children were observed and examined continuously over an eight-month period.
Ethical Consideration
Procedure
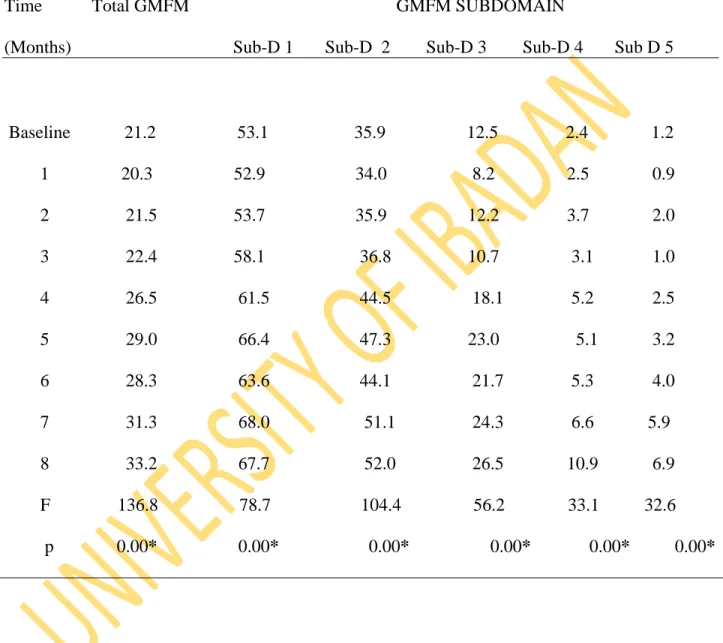
2 Friedman's ANOVA was calculated to determine the trend in gross motor functional development in children with cerebral palsy over an eight-month period. 6 Mann Whitney U was calculated to compare the general health status of caregivers of children with cerebral palsy and the control group over an eight-month period. 7 Mann Whitney U was calculated to compare the quality of life of caregivers of children with cerebral palsy and the control group over an eight-month period.
The GHQ score of caregivers of children with cerebral palsy also showed a statistically significant decrease over eight months.
Hypotheses Testing
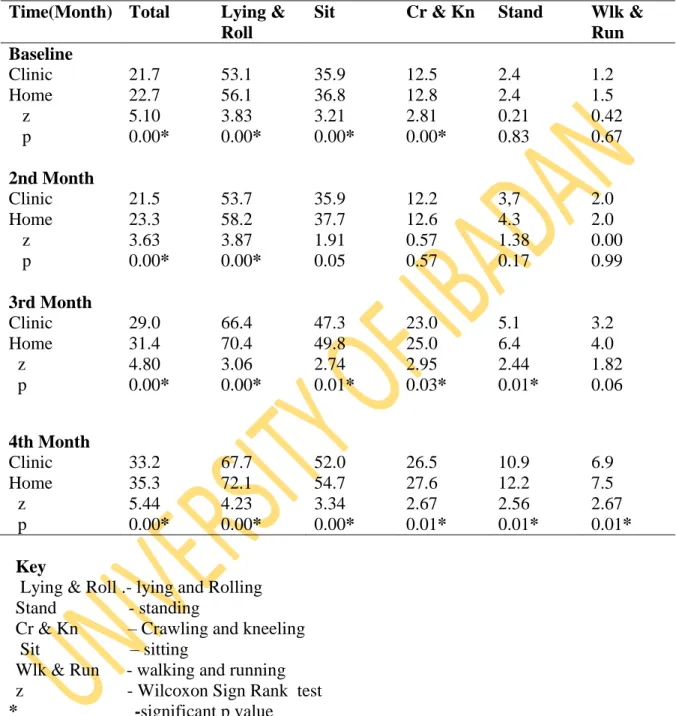
In children with cerebral palsy, there would be no significant difference in the sitting subdomain score of the GMFM over an 8-month period. In children with cerebral palsy, there would be no significant difference in the continuous subdomain score on the GMFM over an 8-month period. There would be no significant difference between gross motor function in children with cerebral palsy assessed in different environmental settings (such as hospital/clinic and at home) over an 8-month period.
There would be no significant difference between the standing score on the GMFM in children with cerebral palsy assessed in different settings ((clinic and home) over an 8-month period.
Discussion
- Physical Characteristics of Participants
- Trend of Gross Motor Function in Children with Cerebral Palsy
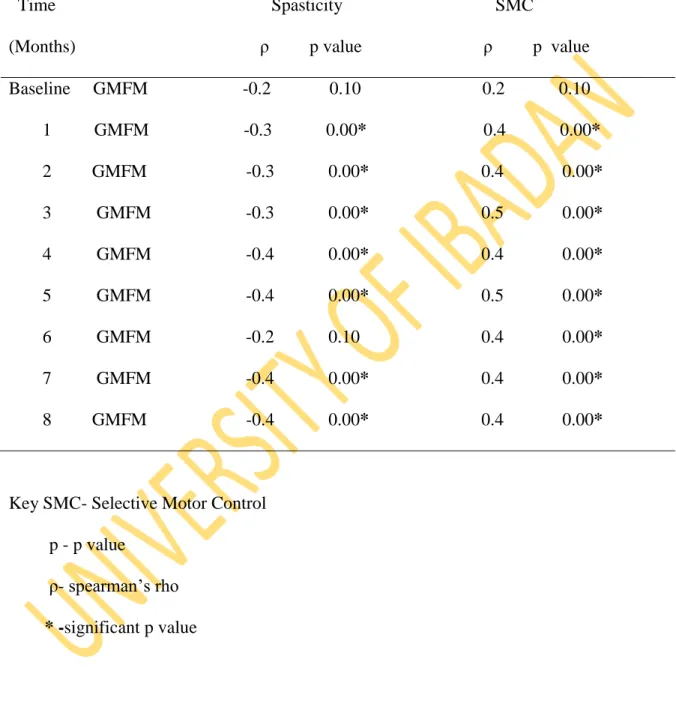
- Relationship between Gross Motor Function and Selected
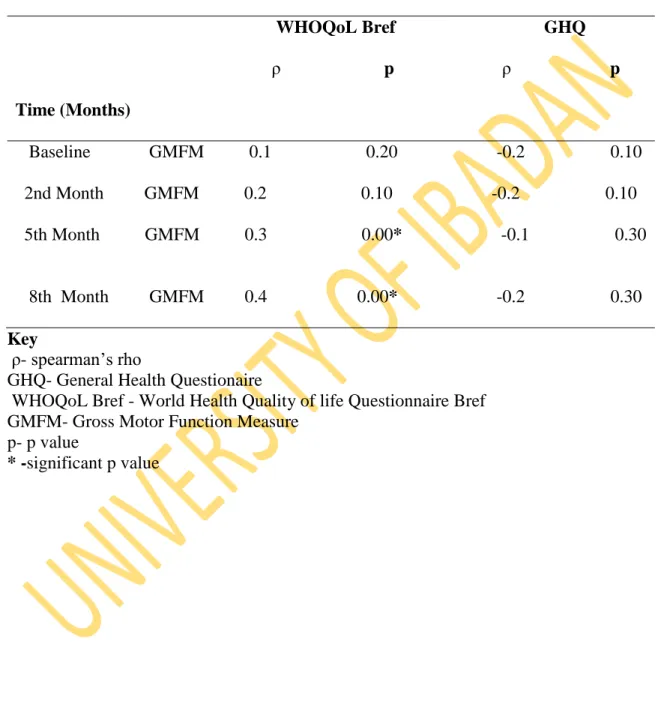
- Trend of Quality of Life and General Health Status of the
- Comparison of the Quality of Life and General Health Status
- The Relationship between Gross Motor Function in
- Comparison of the gross motor function in children with
The GHQ was used in this study to assess the general health status of the caregivers. Furthermore, 48.1% of children with cerebral palsy were their parents' first-born children. From the fifth month of the study, a strong simultaneous improvement in gross motor skills in children with cerebral palsy and the quality of life of their caregivers was obtained.
This could explain the significant positive association between caregivers' quality of life and motor function in children with cerebral palsy.
Summary
Cerebral palsy has also been reported to be the most common condition treated in neuro-pediatric clinics in different parts of Nigeria (Izuora and Ileoje, 1989; Nottidge and Okogbo, 1991; Wammanda et al, 2007; Peters et al, 2008; Ogunlesi et al. al, 2008). Baseline gross motor function of CWCP was assessed in the clinic and their respective homes using the Gross Motor Function Measure (GMFM) and repeated monthly for eight consecutive months to see the influence of the environment on their motor function. The GMFM score increased significantly over the 8 months with significant difference between baseline and first month, 3rd and 4th, 5th and 6th and between 7th and 8th month.
A significant positive correlation (r = between 0.4 and 0.5) between the GMFM and the SMC from the first month to the eighth month was also obtained.
Conclusions
Recommendations
Collagen accumulation in the muscles of children with cerebral palsy and correlation with the severity of spasticity. The relationship between spasticity in young children (18 months old) with cerebral palsy and their gross motor development. Harvey A and Martin L (2009): Recent developments in physiotherapy for children with cerebral palsy: what is the evidence base.
Ketelaar, M and Vermeer, A (1998): Functional motor skills of children with cerebral palsy: a systematic literature review of assessment measures. The impact of environmental factors on the mobility of children with cerebral palsy; Research results and clinical implications. How do changes in body functions and structures, activity and participation relate in children with cerebral palsy?