I certify that this work was carried out under my supervision at the Department of Epidemiology and Medical Statistics, University of Ibadan. The Steering Committee was established by the Federal Government of Nigeria in June 2001 to conduct a review of the existing disease surveillance system in the country and reach consensus on the list of priority diseases.

Statement of the Problem
Other strategies are periodic training and retraining of health workers, program officers and IDSR focal persons at all levels by a set of core trainers established at the Federal Ministry of Health with partners using WHO generic IDSR training modules adapted to Nigeria, development of a comprehensive database of twenty one priority communicable diseases of the national IDSR unit and provision of data management guidelines for use at all levels, establishment of sentinels, epidemic response committees at all levels, case-based surveillance activities and strengthening of laboratories and case management ( FMOH, Nigeria.
Justification and Rationale for the study
Health facilities thus play a very important role in disease surveillance and implementation of IDSR. In light of the fact that the functional disease surveillance and response system depends on adequate capacity building, functional laboratory, communication network and ongoing monitoring and evaluation, which may vary by location (rural/urban facilities), it will be interesting to investigate whether the location of health facilities will affect the surveillance system at this level.
Objectives
Broad Objective
In view of the fact that there are more private than public health facilities (OYSG, 2006), it is imperative that the private facilities are involved in surveillance activities, even if it is coordinated by the public sector. In light of the uncertainty of IDSR being implemented in accordance with the National Technical Guidelines for IDSR, 2002 and the Nigerian National Policy formulated in the year 2005 and the lack of information on its implementation in all health facilities in the country, it therefore becomes necessary to assess the performance of health facilities for IDSR implementation in the country.
Specific Objectives
What is Integrated Disease Surveillance and Response (IDSR)?
The LGA is strategic for this function because it is the first level in the health system that is expected to have a full complement of permanent staff dedicated to all aspects of public health such as monitoring community events, mobilizing for community action, encouraging of national assistance and access to regional resources for health protection of local communities (FMOH, Nigeria. Focal points of surveillance at LGA, state and national levels collaborate with epidemic response committees at each level to plan appropriate response actions to public health and to actively seek opportunities for combining resources (FMOH, Nigeria.
The Goals and Objectives of IDSR 1. The Goal
Support the establishment of an effective communication network for the transmission of surveillance data and epidemiological information at all levels. Conduct sustained advocacy with policy and decision makers at all levels to mobilize resources and support for IDSR activities.
The Priority Diseases Targeted in IDSR
Health facility level
The health center must collect information on the priority diseases based on the disease definition. The health center must initiate a response to the suspected outbreak and also obtain laboratory confirmation through the collection of laboratory samples where appropriate.
State Government level
The local government supervisory offices should collect completed forms from the health facilities, collect them periodically as applicable and send them to the state level. Analyzes are carried out at this level and logs of outbreaks reported by the health facilities are maintained, including the intervention activities (FMOH, Nigeria.
The Federal Level
The Strategies for the Implementation of IDSR
An Epidemic Preparedness and Response Committee shall be established at all levels and strengthened where available. Rapid intervention teams equipped with adequate resources and logistics for rapid intervention shall be established at all levels.
The Global Perspectives on Disease Surveillance
The entire WHO public outbreak record between 1996 and 2009 was analyzed to identify spatio-temporal trends in the timeliness of outbreak detection and public outbreak notification relative to the estimated date of outbreak onset. Reasons cited for noncompliance include not wanting to violate patient privacy and the cumbersome reporting process (Tan H, et al 2009).
The Africa Experience in Literature
Trends of Major Disease Outbreak in the African Region
Although these trends showed an increase in the number of countries affected by cholera outbreaks, the overall case fatality rate (CFR) was on a downward trend. Dysentery has continued to be one of the major recurrent disease outbreaks in the African region with an increase in the number of countries reporting dysentery to WHO/AFRO from three in 2003 to 23 in 2007. In 1999, an estimated 871,000 deaths occurred from measles. worldwide with 61% occurring in sub-Saharan Africa.
Yellow fever is endemic in 33 countries in the African region, of which 12 countries account for approximately 75% of the total disease burden and 89%. In the African region, outbreaks of bird flu have occurred in domestic birds in Benin, Burkina Faso, Cameroon, Ivory Coast, Ghana, Niger, Nigeria and Togo.
Status of Integrated Disease Surveillance and Response (IDSR) in Africa Countries
Following the adoption of the IDSR in 1998 by the member states of the WHO African Region, Tanzania recorded baseline disease surveillance and response data between October and December 2003, and then began further data collection between January and March 2005. introduction of IDSR. There was also an increase in awareness of IDSR in several of the districts studied with improved data analysis, which was unfortunately below international standards (USAID, 2006). In 2007, in Nigeria, a team of researchers in the northern part of the country assessed the emergency preparedness and capacity of the local government area to identify disease outbreaks, comparing their findings with the recommendations of the 2002 National Technical Guidelines on IDSR.
Apart from the availability of a budget line for emergency preparedness in the surveyed LGA, most of the other findings were rather alarming. There were no prepositioned drugs or vaccines, only 8% of staff trained in IDSR, no use of thresholds or makers, no analysis of available data at LGA level, and both timeliness and completeness of reporting were poor (Abubakar AA, et al .2010) The findings of this group of researchers were consistent with the observations of the Forum of State Epidemiologists in Nigeria as described in a communique issued by this group of professionals after their annual meeting in Enugu.
Study Area
Study Sites
It has an area of 27 km² and a population of 306,795 at the 2006 census. It is largely inhabited by non-indigenes of Ibadan and the elites. The leading university, University of Ibadan and Apex hospital in the city, University College Hospital, Polytechnic, Ibadan and many other institutions are located in this LGA. Some priority diseases reported in this LGA include malaria, diarrheal disease, measles, cholera, tuberculosis, neonatal tetanus, HIV/AIDS, Dracunculiasis, Hepatitis B, Poliomyelitis (OYSMOH, 2008).
Some priority diseases reported in this LGA include malaria, diarrheal disease, measles, cholera, tuberculosis, neonatal tetanus, HIV/AIDS, Oncocerciasis, Hepatitis B, Yellow Fever, Poliomyelitis (OYSMOH, 2008). These were the supervisory focal persons in the health facilities or the facility head or a designated staff where there was no focal person.
Study Design
Sampling size
Sampling Technique
The researcher and the research assistant asked about the focal supervision person in each health institution studied and this person was interviewed. Instead, the facility manager or a person designated by the facility manager was interviewed where key persons did not exist. A total of 126 health facilities were identified in Ibadan North LGA, excluding laboratories, eye and dental facilities.
Instrument Design and Procedure for Data Collection
This included the type and class of the facility, the occupation and designation of the respondent, the age and gender of the respondent and the years of experience of the respondent. The information sought under this section was: Knowledge of where to direct reports of priority diseases from health facilities when they are made, Identification of epidemic-prone diseases, diseases targeted for eradication and elimination, diseases of public health concern from lists of diseases. This section explored the opinion of the respondent about IDSR and their view of the process (whether cumbersome, easy or enjoyable), whether they think IDSR has helped reduce burden of priority diseases or not, and whether they need more information about IDSR or not.
Are priority diseases reported from the institution and to whom they are reported. Availability of a list of communication devices, a clinical register for keeping disease records in the institution.
Statistical Analysis
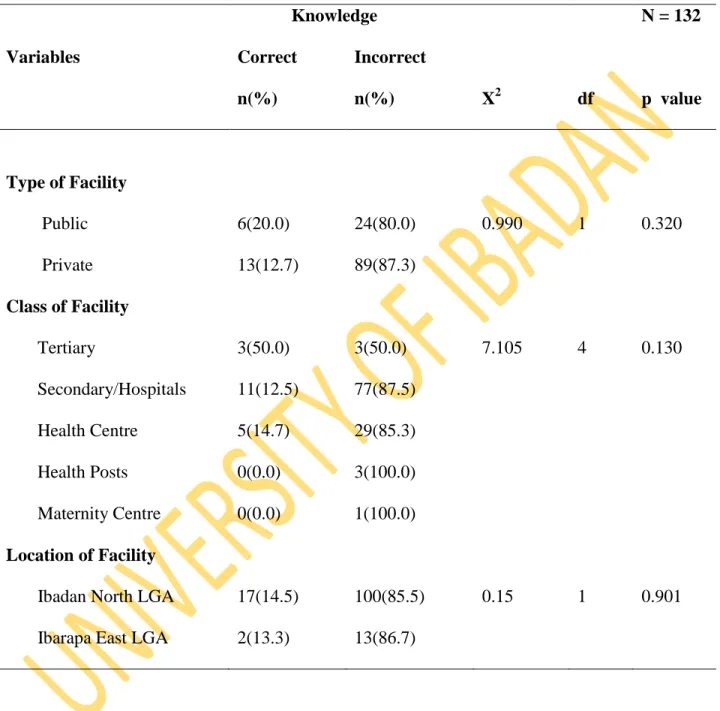
The frequencies and cumulative frequencies of each of the composite scores were generated from which conclusions about the level of knowledge or practice of the study population for each aspect were derived. Similarly, these composite scores were used to perform bivariate analysis (student's „t‟-test and chi square) to compare the public and private health facilities and urban and rural areas.
Ethical Considerations
Demographic Structure of Studied Sites and Population
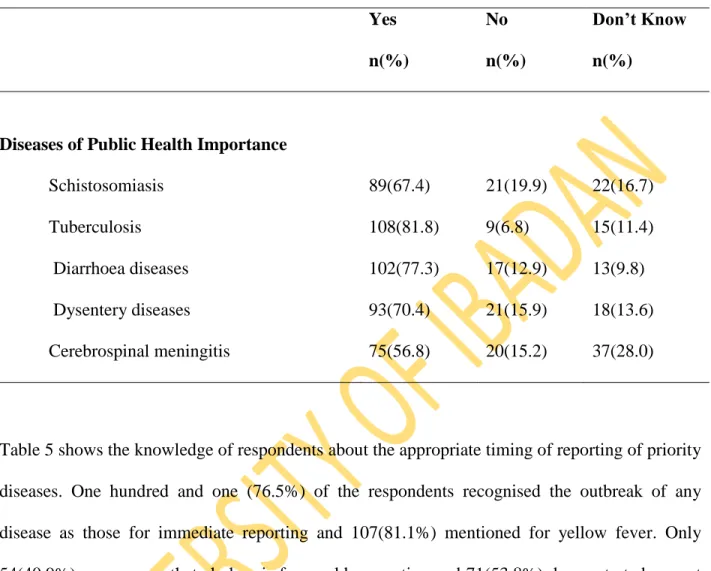
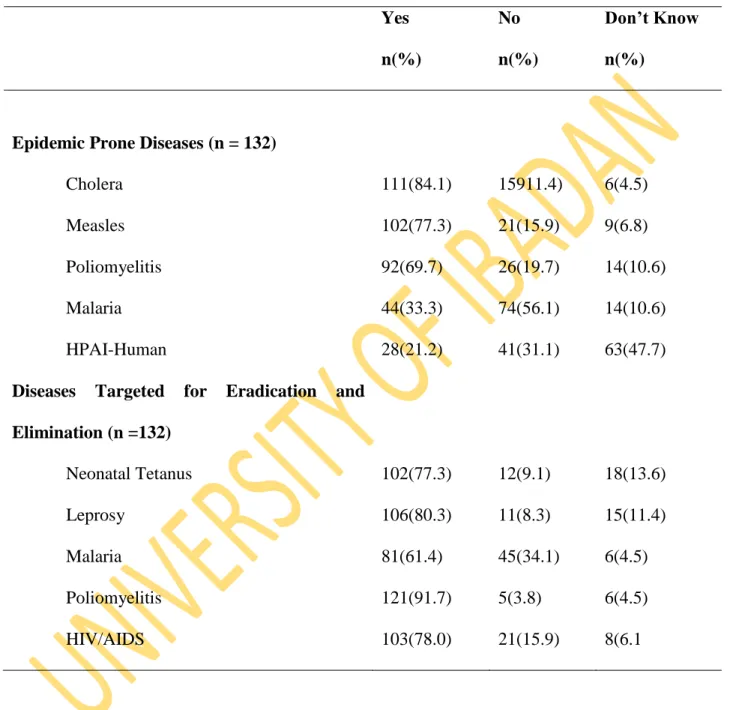
Adequate knowledge of where priority disease reports should be directed (LGA PZC department) was demonstrated by some respondents. Other inappropriate responses and response frequencies are shown in Table 2 below. The knowledge of the epidemiological classifications of the disease demonstrated by the respondents is shown in Tables 3 and 4, respectively.
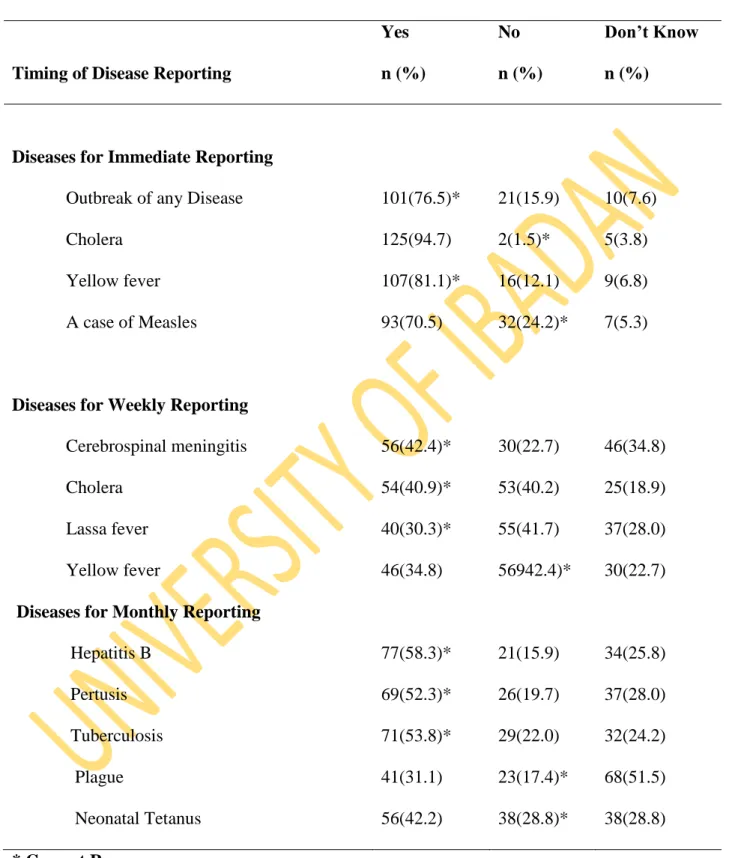
Only 54 (40.9%) were aware that cholera is intended for weekly reporting and 71 (53.8%) demonstrated that they had appropriate knowledge of tuberculosis as a disease for monthly reporting. The pattern of responses to other diseases assessed for knowledge of the appropriate time of reporting is shown in Table 5.
Comparisons of Knowledge of Disease Surveillance between the categories of Respondents
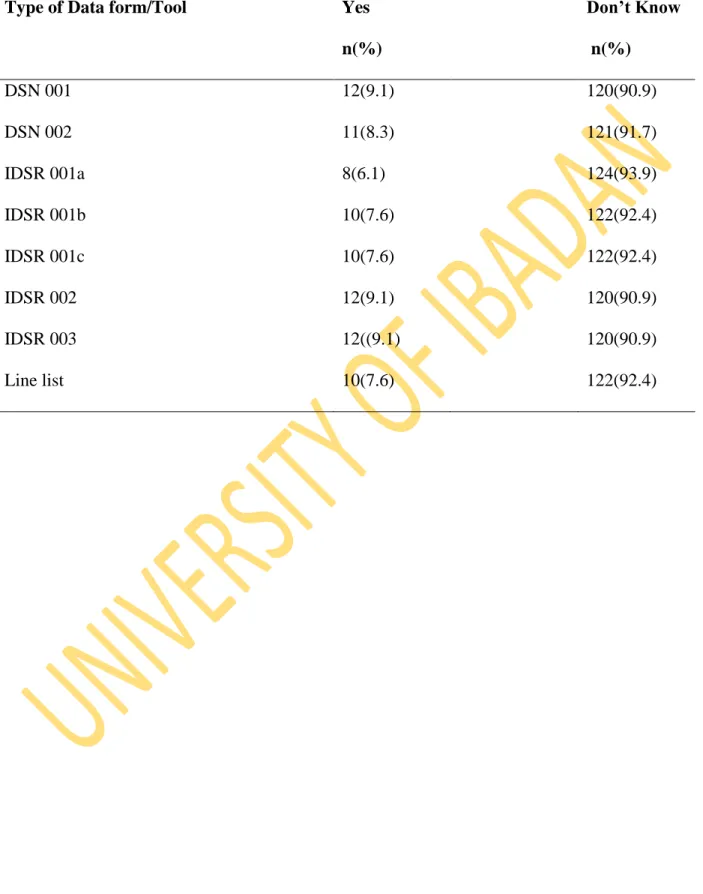
Knowledge of Reporting forms and Tools used in IDSR
Knowledge of Case Definitions of Diseases
The Composite Scores for Knowledge of Disease Surveillance
Surveillance Practice
IDSR Implementation Score
Surveillance Focal Person
Appropriateness and Timeliness of Reporting
After verification of claims by checking relevant records according to standard guidelines, only 2 facilities (1.5%) were established to practice IDSR both timely and appropriately. It was a public health facility in Ibadan North LGA and a private health facility in Ibarapa East LGA. The different forms used by the facilities that claimed to report are as shown in Table 15.
The outbreak preparedness indices studied showed that there was no record or evidence of outbreak preparedness in any of the health facilities studied during this study period.
Training and Logistics Issues
Of the 2.1 million registered nurses in the United States, only about 1.5% are men. A good number of respondents also showed correct knowledge of the appropriate time to report certain priority diseases. Another identified disease surveillance knowledge gap among the study population was poor knowledge of reporting forms and tools demonstrated by respondents.
There was no difference in knowledge of case definitions across the spectrum of the study population. This low level of reporting is consistent with reports from other parts of the world. 12. The report of priority diseases by Health Institutions when made, should be to which of the following government agents.
Have any facility staff attended training on IDSR in the past one year.
ETHICAL APPROVAL)
IDSR FORM OO1A)
IDSR FORM 001B)
IDSR FORM 002)
IDSR FORM 003)
RECOMMENDED CASE DEFINITIONS OF PRIORITY DISEASES)
LIST OF LOCAL GOVERNMENT AREAS IN OYO STATE)