Annals of Hepatology 7(3) 2008: 230-234
230
www.medigraphic.com
Annals of Hepatology 2008; 7(3): July-September: 230-234
Annals of Hepatology
Original Article
Model for end stage of liver disease (MELD)
is better than the Child-Pugh score for
predicting in-hospital mortality related to
esophageal variceal bleeding
Ángel Ricardo Flores-Rendón;1 José Alberto González-González;1 Diego García-Compean;1
Héctor Jesús Maldonado-Garza;1 Aldo Azael Garza-Galindo1
1Facultad de Medicina y Centro Regional para el Estudio de
Enfermedades Digestivas. (CREED) Hospital Universitario «Dr. José Eleuterio González» UANL. Monterrey, N.L. México.
Address for correspondence: José Alberto González-González
Facultad de Medicina y Centro Regional para el Estudio de Enfermedades Digestivas. (CREED) Hospital Universitario «Dr. José Eleuterio González» UANL. Monterrey, N.L. México. Madero y Gonzalitos S/N Col. Mitras Centro, Monterrey, N.L. México.
Phone: (52)(81)83333664. Fax: (52)(81)83486068. E-mail:[email protected]
Manuscript received and accepted: 26 May and 16 July 2008
Abstract
Aim: The Child Pugh and MELD are good methods for predicting mortality in patients with chronic liver dis-ease. We investigated their performance as risk factors for failure to control bleeding, in-hospital overall mor-tality and death related to esophageal variceal bleed-ing episodes. Methods: From a previous collected data-base, 212 cirrhotic patients with variceal bleeding ad-mitted to our hospital were studied. The predictive capability of Child Pugh and MELD scores were com-pared using c statistics. Results: The Child-Pugh and MELD scores showed marginal capability for predict-ing failure to control bleedpredict-ing (the area under receiver operating characteristics curve (AUROC) values were < 0.70 for both). The AUROC values for predicting in-hospital overall mortality of Child-Pugh and MELD score were similar: 0.809 (CI 95%, 0.710 - 0.907) and 0.88 (CI 95% 0.77- 0.99,) respectively. There was no significant difference between them (p > 0.05). The AU-ROC value of MELD for predicting mortality related to variceal bleeding was higher than the Child-Pugh
score: 0.905 (CI 95% 0.801-1.00) vs 0.794 (CI 95% 0.676 – 0.913) respectively (p < 0.05). Conclusions:
MELD and Child-Pugh were not efficacious scores for predicting failure to control bleeding. The Child-Pugh and MELD scores had similar capability for predict-ing in-hospital overall mortality. Nevertheless, MELD was significantly better than Child-Pugh score for predicting in-hospital mortality related to va-riceal bleeding.
Key words: Variceal bleeding, MELD, Child-Pugh, fail-ure to control bleeding, esophageal varices.
Introduction
Esophageal variceal bleeding (EVB) in cirrhotic pa-tients is one of the most severe complications and has a mortality rate of 13% to 30 %.1-3 Patients with advanced
liver disease are at higher risk to develop complications or to die because of hypovolemic shock, infections and liver failure.4,5
Diverse methods have been used for predicting com-plications and mortality rates in cirrhotic patients over the last decades. One of the most used is the Child-Pugh (CP) score. It was developed in 1973 as a modification of the Child-Turcotte´s score, by substituting the nutrition status variable for prothrombin time.6
One limitation of the CP score is the use of two clini-cal parameters such as ascites and hepatic encephalopa-thy. The subjective assessment for grading these parame-ters can affect the reliability of the score.
Recently, a Model for End Stage of Liver Disease (MELD) was designed in order to determine the com-plication risks in patients with transjugular
intrahepat-ic portosystemintrahepat-ic shunts.7 This method comprises three
biochemical parameters: serum bilirrubin, prothrom-bin time and serum creatinine. MELD was also used in cirrhotic patients with various clinical conditions, in-cluding renal failure, gallbladder surgery, liver trans-plant and acute alcoholic hepatitis. It has proved its
Artemisa
AR Flores-Rendón et al.MELD for variceal bleeding
www.medigraphic.com
utility as an independent indicator of survival.8-12
Be-cause MELD is more accurate than CP score for pre-dicting short term (3 months) mortality, it was prompt-ly adopted by the UNOS to allocate liver grafts for transplantation.13,14
Studies assessing the efficiency of CP and MELD score in predicting mortality of any cause in cirrhotic pa-tients with EVB have also been published.15-17
Neverthe-less, to our knowledge the utility of CP and MELD score for predicting 5-day failure to control bleeding and mor-tality related to variceal bleeding episodes has not been evaluated.
Patients and methods
All cirrhotic patients from a database with a diagno-sis of an acute EVB episode admitted to our hospital between 2003 and 2006 were studied. The inclusion criteria were: adult patients with diagnosis of hepatic cirrhosis of any etiology (diagnosed by liver biopsy, clinical manifestations and/or imaging studies) and acute EVB (hematemesis and/or melena occurred dur-ing a period of 24 hrs before admission due to endo-scopically confirmed esophageal varices). We exclud-ed non-cirrhotic patients with EVB or cirrhotic pa-tients with any other source of bleeding such as gastric varices, congestive gastropathy or ectopic varices and as well as patients with hepatocellular carcinoma. Vari-ables such as age, gender, comorbid entities, etiology of cirrhosis and type of haemostatic treatment were re-corded for each patient. The variceal size was defined by the Paquet classification.18
Liver function at admission was assessed using the CP and MELD scores. The CP score was determined using the classical parameters: ascites, encephalopathy, serum albumin, total bilirubin and prothrombin time. The pa-tients were classified as CP stages A (5-6 points), B (7-9 points) and C (10 or more points).6 The MELD was
calcu-lated using the following formula: 3.8 log e (serum bi-lirubin mg/dL) + 11.2 log e (INR) + 9.6 log e (serum crea-tinine mg/dL) + 6.4.6
During hospitalization the following variables were determined: a) 5-day failure to control bleeding: which was defined according to Baveno IV19 as fresh
hemateme-sis > 2 hrs after performing an endoscopic treatment or the administration of vasoactive drugs, 3 g drop in Hb and death in a time frame of 120 hours; b) overall mor-tality:which was defined as death due to any cause
dur-ing the hospitalization and c) mortality related to an
EVB episode: which was defined as death due to cardio-vascular failure and/or hemodynamic instability as a re-sult of uncontrollable hemorrhage during admission or rebleeding episode (fresh hematemesis > 2 hrs after ini-tial treatment or a 3 g drop in Hb) occurring any time dur-ing the hospitalization despite new endoscopic of phar-macologic treatment.
Statistical analysis
The continuous variables were expressed as mean, range and standard deviation. For relative proportions the 95% confidence intervals were calculated. The per-formance of CP and MELD scores for predicting the rates of failure to control bleeding, overall mortality and mortality related to EVB was evaluated by mea-surement of their discriminative ability, estimated by the concordance c-statistic (area under the Receiving Operating Characteristics (AUROC) curves. An AUROC value of > 0.70 was considered as clinically relevant. Statistical differences between both scores were as-sessed comparing the AUROC values by means of the Z test. An alpha value of < 0.05 was considered statistical significant. The program SPSS v 13.0 was used for the statistical analysis.
Results
Clinical and biochemical characteristics of patients
(Table I)
Two hundred twelve patients were included into the study: 145 were male (68%) with a mean age of 53 years old (range 27 – 91 years). The most frequent etiology of cirrhosis was alcohol abuse (73%). Thirty five patients (17%) showed renal impairment mani-fested by serum creatinine > 1.5 mg/dL. Only one pa-tient had a history of chronic renal failure non treat-ed with dialysis.
Using the CP score 38 patients (18%) were on stage A, 108 patients (51%) on stage B ad 66 (31%) on stage C. The Meld mean value was 15 + 7.
Table I. Clinical and biochemical features of patients.
Patients, N 212
Gender (M/F) 145/65
Age, mean ± SD 53 ± 12
Etiology of cirrhosis, n (%)
Alcohol 154 (73)
Virus B/C 15 (7)
Autoimmune 7 (3)
Other 38 (17)
Biochemical tests, mean ± SD
Hemoglobin, g/DL 8.7 ± 2.8
Total bilirubin, mg/DL 2.5 ± 3.2 Serum creatinine, mg/DL 1.1 ± 1
INR, mg/DL 1.9 ± 2.1
Child-Pugh stage, n (%)
A 38 (18)
B 108 (51)
C 66 (31)
Child-Pugh score, mean ± SD 9 ± 3
MELD, mean ± SD 15 ± 8
www.medigraphic.com
Endoscopic findings and treatment of bleeding
(Table II)
The esophageal variceal size was determined as Grade I in one patient (0.5%), Grade II in 90 (42.5%), Grade III in 104 (49%) and Grade IV in 17 patients (8%). There were 155 patients (73%) with recent stigmata of variceal bleeding, 39 had active variceal bleeding (oozing or spurting from a varix) and 18 had blood in the stomach without any other source of bleeding.
All patients received endoscopic treatment: variceal band ligation was used in 202 patients (95.5%), sclero-therapy (with Polidocanol 1.5% in 9 (4%) patients and one patient was treated with both procedures (0.5%). In 19 patients a vasoactive drug (octreotide) was adminis-tered intravenously. Antibiotic prophylaxis (with IV or PO ciprofloxacin or norfloxacin) was prescribed to all pa-tients since hospital admission and during a period of at least seven days.
The mean length of hospital stay was 5.1 days (range 1 to 32 days).
Capability of CP and MELD to predict 5-day failure to control bleeding, overall mortality and mortality relat-ed to EVB.
a) Control bleeding: seventeen (8%) patients presented failure to control bleeding. Eleven of these patients died during the first five days after admission. In 8 of them death was considered related to the bleeding event (Table II).
The AUROC values for failure to control bleeding were: for CP 0.69 (CI 95% 0.56-0.82) and for MELD 0.67 (CI 95% 0.49-0.86). No significant statistical dif-ferences were observed between both methods (p > 0.05) (Figure 1).
b) Overall mortality: Seventeen patients died (8%). Three were on CP stage B and 14 on CP stage C.
Death was attributed to the EVB episode in 10 pa-tients; to liver failure in 5 patients (three of hepatic coma and 2 of hepatorenal syndrome type 1), sepsis in one and another patient because of pulmonary com-plications (Table II).
Concerning in-hospital overall mortality rate, the AU-ROC values of CP and MELD scores were 0.80 (CI 95%, 0.71 - 0.90) and 0.88 (CI 95% 0.77- 0.99) respec-tively. Both methods significantly predicted mortali-ty, but they had similar values and no statistical sig-nificant difference was found (p < 0.05) (Figure 2). c) Mortality due to EBV: From the 10 patients whose
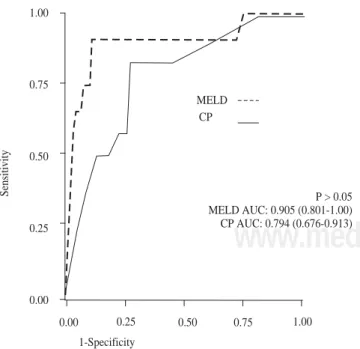
death was attributed to the EVB episode 4 died at ad-mission and 6 died during hospitalization.
Finally, the AUROC values for CP and MELD scores in regard to mortality rate induced by the EVB epi-sode were: 0.79 (CI 95% 0. 0.67 – 0.91) and 0.90 (CI 95% 0.80-1.0) respectively. Although, both scores are good predictive tools, MELD was superior to CP score (p < 0.05) (Figure 3).
Discussion
The MELD score was originally designed with the objective to predict mortality risk in patients with trans-jugular intrahepatic portosystemic shunts (TIPSS).7
Af-ter this, MELD was evaluated as prognostic score for mortality in patients with chronic liver disease in differ-ent clinical situations.8-12 In the other side, the CP score
is simpler and easier to calculate at bedside than MELD. Similar to the original Child‘s grading, neither the divi-sion of the grades nor the scoring system of CP score
were statistically validated.6 Although CP score has
proved consistency and reproducibility in many stud-ies, it has serious limitations: 1) two variables are
clini-Table II. Endoscopic findings, treatment of bleeding and outcomes of patients.
Endoscopic findings, n (%)
Active bleeding 39 (18)
White nipple sign 155 (74)
Blood in stomach and NOSB 18 (8) Treatment of bleeding, n(%)
Endoscopic treatment 100 (100)
Band ligation 202 (95.5)
Sclerotherapy 9 ( 4)
Combined 1 (0.5)
Pharmacological therapy, n (%) 19 (9) Units of blood transfused, mean ± SD 2.2 ± 1.7 Outcomes of patients, n (%)
5-day failure to control bleeding, 17 (8)
Overall deaths 17 (8)
Deaths due to variceal bleeding 10 (5)
AR Flores-Rendón et al.MELD for variceal bleeding
www.medigraphic.com
and biochemical parameters such as serum creatinine, serum sodium and encephalopathy has been proposed in order to increase its sensibility.6
Although MELD has fewer variables than CP score, its calculation is more complicated. It may require the use of a computed system or internet services. Notwithstanding the advantage of this method is the use of objective vari-ables particularly serum creatinine which is a very impor-tant prognostic risk parameter for mortality in patients with chronic liver disease.
Recently, some studies have compared CP and MELD score in cirrhotic patients on waiting lists for liver trans-plantation; in patients with TIPSS and in cirrhotic pa-tients with and without complications.7-14 In all of them,
CP and MELD scores had similar capability for predict-ing mortality, except in patients on waitpredict-ing lists for liver transplantation, in whom MELD had substantially better predictive power.
The results of our study were similar to those report-ed in previous studies in which the CP and MELD scores were assessed in patients with EVB for in-hospi-tal morin-hospi-tality rates due to any cause.15,16 Nevertheless, we
found that MELD was better than the CP score for pre-dicting in-hospital mortality related to the EVB epi-sode. As far as we know this issue has not been previ-ously evaluated.15-17,19
Several factors may be evoked for explaining the bet-ter performance of MELD for predicting mortality related to EVB that was observed in our study: 1) the patients who died may have had renal impairment before the oc-currence of the bleeding episode, 2) More severe bleed-ing may have given rise to acute renal failure due to he-modynamic instability and hypovolemic shock in some patients particularly those who died, 3) liver function was probably more deteriorated in patients who died. That was probably reflected by higher values of serum bi-lirubin, serum creatinine and prothrombin time.
On the other side, it is important to underline that our in-hospital mortality rate (8%) was lower than the one ob-served in other series particularly in Chalassani and Car-bonell studies. These authors reported a mortality rate of 14.2% and 14.5% respectively.2,3 These differences may
be explained by some factors: 1) in the Chalassani study only 64% of the patients were treated with antibiotic phylaxis. It is well known, that the use of antibiotic pro-phylaxis in patients with EVB reduces the in-hospital mortality rate by 9%;21 2) in the Carbonell study, the
pa-tients sample size was small (83 papa-tients) and papa-tients with gastric varices and hepatocellular carcinoma were included.2 Recently, the mortality rate during the first 7
days of hospital admission was reported to be of 9.7% which is similar to our study.22 Unfortunately, this study
was published only in abstract form and more specific de-tails were unavailable.
Finally, in our study MELD and CP scores were not efficacious tools for predicting 5-day failure to cal such as ascites and encephalopathy, therefore
impre-cision in their subjective assessment may occur; 2) The continuous variables in the CP score are categorized us-ing arbitrary cut-off points. Therefore, this gradus-ing sys-tem does not distinguish some subgroups inside each
stage («mild» grade C from «severe» grade C, etc.).6
Thus, the combination of CP score with other clinical
0.00 0.25 0.50 0.75 1.00
1-Specificity
P < 0.05 MELD AUC: 0.880 (0.770-0.990) CP AUC: 0.809 (0.710-0.907)
MELD CP 1.00
0.75
0.50
0.25
0.00
Sensitivity
Figure 2. ROC curves for overall in-hospital mortality.
Figure 3. ROC curves for mortality due to bleeding of esophageal varices.
0.00 0.25 0.50 0.75 1.00
1-Specificity
P > 0.05 MELD AUC: 0.905 (0.801-1.00) CP AUC: 0.794 (0.676-0.913) MELD
CP 1.00
0.75
0.50
0.25
0.00
www.medigraphic.com
control bleeding since their AUROC values were < than 0.70. The usefulness of MELD score for predict-ing failure to control bleedpredict-ing may be further evalu-ated in future trials.
Certainly, our study does have several limitations: 1) it is derived from a database; 2) we did not assess the in-fluence of some variables in the outcome of patients such as spontaneous bacterial peritonitis, sepsis, and hy-ponatremia. However, none of these variables are taken into account in CP and MELD scores; 3) we did not in-clude patients with gastric variceal bleeding, ectopic va-rices or hepatocellular carcinoma.
In conclusion, our results showed that the CP and MELD scores are not efficacious methods for predicting failure to control bleeding. Conversely they are equally efficient tools for predicting in-hospital overall mortali-ty. Nevertheless, MELD is significantly better than CP score for predicting mortality related to an acute EVB ep-isode. Prospective clinical trials are needed to confirm this later finding.
Acknowledgements
We would like to thanks Doctors- Rafael Castañeda-Sepulveda, Miguel Mar-Ruiz,Jorge Leal-Salazar, Edu-ardo Mendoza-Fuerte and Laura Cortez-Sanabria for the help on this work.
References
1. Graham D, Smith L. The course of patients after variceal hemor-rhage. Gastroenterology 1981; 80: 800-9.
2. Carbonell N, Pauwells A, Serfaty L, Fourdan O, Lévy VG, Poupon R. Improved survival after variceal bleeding in patients with cirrhosis over the past two decades. Hepatology 2004; 40: 652-9. 3. Chalasani N, Kahi C, Francois F, Pinto A, Marathe A, Bini EJ, Pandya P, Sitaraman S, Shen J. Improved patient survival after acute variceal bleeding: a multicenter, cohort study. Am J Gastro-enterology 2003; 98: 653-9.
4. Park DK, Um SH, Lee JW, Lee JB, Kim YS, Park CH, Jin YT, Chun HJ, Lee HS, Lee SW, Choi JH, Kim CD, Ryu HS, Hyun JH. Clinical significance of variceal hemorrhage in recent years in patients with liver cirrhosis and esophageal varices. J Gastroenterol Hepatol 2004; 9: 1042-51.
5. D’Amico G, De Franchis R: Cooperative Study Group. Upper digestive bleeding in cirrhosis. Post-therapeutic outcome and prognostic indicators. Hepatology 2003; 38: 599-612. 6. Durand F, Valla D. Assessment of the prognosis of cirrhosis:
Child-Pugh vs MELD. J Hepatol 2005; 42: Suppl (1): 100-7. 7. Malinchoc M, Kamath PS, Gordon FD, Gordon FD, Peine CJ,
Rank J, ter Borg PC. A Model to predict poor survival in patients
undergoing transjugular intrahepatic portosystemic shunts.
Hepatology 2000; 31: 864-71. [PMID: 10733541]
8. Terra C, Guevara M, Torre A, Gilabert R, Fernández J, Martín-Llahí M, Baccaro ME, Navasa M, Bru C, Arroyo V, Rodés J, Ginès P. Renal failure in patients with cirrhosis and sepsis unre-lated to spontaneous bacterial peritonitis: value of MELD score.
Gastroenterology 2005; 129: 1944-53.
9. Perkins L, Jeffries M, Patel T. Utility of preoperative scores for predicting morbidity after cholecystectomy in patients with cir-rhosis. Clin Gastroenterol Hepatol 2004; 2: 1123-8.
10. Heuman D, Mihas A. Utility of the MELD score for assessing 3-month survival in patients with liver cirrhosis: one more positive answer. Gastroenterology 2003; 125: 992-3.
11. Dunn W, Jamil LH, Brown L, Wiesner RH, Kim WR, Menon KV, Malinchoc M, Kamath PS, Shah V. MELD accurately predicts mortality in patients with alcoholic hepatitis. Hepatology 2005; 41: 353-8.
12. Srikureja W, Kyulo NL, Runyon B, Hu KQ. MELD score is a better prognostic model than Child-Turcotte-Pugh score or Dis-criminant Function score in patients with alcoholic hepatitis. J Hepatol 2005; 42: 700-6.
13. Cholongitas E, Marelli L, Shusang V , Senzolo M, Rolles K, Patch D, Burroughs AK. A systematic review of the performance of the Model for End Stage Liver Disease (MELD) in the setting of liver transplantation. Liver Transpl 2006; 12: 1049-61.
14. Biggins S, Bambha K. MELD-Based liver allocation: Who is underserved? Semin Liver Dis 2006; 26: 211-20.
15. Lee JY, Lee JH, Kim SJ, Choi DR, Kim KH, Kim YB, Kim HY, Yoo JY. Comparison of predictive factors related to the mortality and rebleeding caused by variceal bleeding: Child Pugh score, MELD score and Rockall score. Taehan kan Hakhoe Chi 2002; 8: 458-64.
16. Chalasani N, Kahi C, Francois F, Pinto A, Marathe A, Bini EJ, Pandya P, Sitaraman S, Shen J. Model for End-Stage Liver Dis-ease (MELD) for predicting mortality in patients with acute va-riceal bleeding. Hepatology 2002; 35: 1282-4.
17. Amitrano L, Guardiascione MA, Bennato R, Manguso F, Balzano A. MELD score and hepatocellular carcinoma identify patients at different risk of short-term mortality among cirrhotics bleeding from esophageal varices. J Hepatol 2005; 42: 820-5.
18. Paquet KJ. Prophylactic endoscopic sclerosing treatment of the oesophageal wall in varices: a prospective controlled random-ized trial. Endoscopy 1982; 14: 4-5.
19. De Franchis R. Evolving Consensus in Portal Hypertension. Re-port of the Baveno IV consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol 2005; 43: 167-76.
20. Saab S, Landaverde C, Ibrahim AB , Durazo F, Han S, Yersiz H, Farmer DG, Ghobrial RM, Goldstein LI, Tong MJ, Busuttil RW. The MELD score in advanced liver disease: association with clini-cal portal hypertension and mortality. Exp Clin Transplant 2006; 4: 395-9.
21. Bernard B, Grange JD, Khac EN, Amiot X, Opolon P, Poynard T. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: A meta-analy-sis. Hepatology 1999; 29: 1655-61.