EJPOD
Eur J Pod 2017; 3 (1): 1-7 ORIGINAL ARTICLE
The Relationship between Plantar Fasciitis and Plantar Heel Pressure
La Relación entre la Fascitis Plantar y la Presión de Talón Erica Bartolo 1, Cynthia Formosa 1*, Alfred Gatt 1.
1Departament of Podiatry, University of Malta, Malta.
* Correspondence: Cynthia Formosa (Senior Lecturer). Faculty of Health Sciences. University of Malta. Email: [email protected]
Abstract
Objective: The presence of increased medial heel plantar pressure in plantar fasciitis has been debated, with clinicians often utilizing pressure-relieving devices, such as heel pads and cups, as a means of management.
Method: Plantar pressures in a sample of 15 adult participants with chronic plantar fasciitis were compared to plantar pressures of the 15 adult participants forming the control group, who were matched for age, gender and weight.
Results: There were no significant differences in peak heel plantar pressure (p = 0.244), lateral peakplantar pressure (p = 0.876), forefoot peak plantar pressure (p = 0.576) and the Forefoot to Rearfoot peak pressure ratio (p = 0.242) between the 2 groups. However, there was a significant difference (p = 0.015) in medial heel peak plantar pressure between the 2 groups, with the plantar fasciitis group having lower medial heel pressure than the control group.
Conclusion: The findings in this study suggest that there is no relationship between peak medial heel plantar pressures and chronic medio-plantar heel pain in medio-plantar fascitis. There is also no shift in pressure from the symptomatic medio-medio-plantar heel region to the latero-medio-plantar heel and forefoot regions. As a result, pressure may not play a part in the pathophysiology of plantar fascitis.
Key Words:plantar fasciitis; plantar pressure; heel pain. Resumen
Objetivos: La presencia de incremento de presión plantar en la zona medial del talón en la fascitis plantar ha sido estudiado, y los clínicos a menudo utilizan dispositivos de alivio de la presión, como almohadillas de talón y cazoletas, como medio de manejo. Método: Las presiones plantares en una muestra de 15 participantes adultos con fascitis plantar crónica se compararon con las presiones plantares de los 15 participantes adultos que formaron el grupo control, que fueron comparados por edad, sexo y peso. Resultados: No hubo diferencias significativas en la presión plantar en el pico pico (p = 0,244), en la presión pico lateral (p = 0,876), en la presión plantar pico en el antepié (p = 0,576) Los 2 grupos. Sin embargo, hubo una diferencia significativa (p = 0,015) en la presión plantar del talón medial entre los 2 grupos, con el grupo de fascitis plantar con menor presión en el talón medial que en el grupo control.
Conclusión: Los hallazgos en este estudio sugieren que no hay relación entre el pico medial del talón de las presiones plantares y crónico medio-plantar talón dolor en la fascitis plantar. Tampoco hay cambio en la presión de la región sintomática del talón medio-plantar a las regiones del talón latero-plantar y del antepié. Como resultado, la presión puede no desempeñar un papel en la fisiopatología de la fascitis plantar.
Palabras Clave: fascitis plantar; presión plantar; dolor de talón.
Received: 29 June 2016; Acept: 17 Septembre 2016. Conflicts of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Introduction
Plantar heel pain associated with plantar fasciitis is a syndrome which has been estimated to account for ten percent of all musculoskeletal pathologies of the lower limb within the American population, including both athletes and the non-athletes (1,2).
Although plantar fasciitis has often been defined as an inflammatory condition of the plantar fascia that may involve microtears or partial rupture of fascial fibres,more recent investigations report findings that include myxoid degeneration with fragmentation and degeneration of the plantar fascia and bone marrow vascular ectasia (3). The typical chief complaint would be pain around the medio-plantar aspect of the heel during the first few steps in the morning or after prolonged inactivity during the day (4).
It is a difficult problem to manage as the mechanism of injury is poorly understood, thus optimal treatment cannot be provided (5, 6). The aetiology of plantar fasciitis is probably multifactorial (2,7) although it may be mainly secondary to a mechanical origin (8). However, there has been consistent conflict in scientific research regarding the “longitudinal traction hypothesis” versus the “vertical compression hypothesis” as the cause for plantar fasciitis (9).
Hicks (1954) initiated the idea of the plantar fascia acting as a windlass mechanism in order to provide support and tension throughout the medial longitudinal arch during weight bearing activities (10). Following on Hick’s notion, Fuller expanded on the concept of this theory. As the subtalar joint pronates and lowers the medial longitudinal arch during gait, the plantar fascia tightens, often resulting in significant traction forces applied to the insertion of the plantar fascia due to inefficient foot function, often resulting in pain and inflammation (11).
Conversely, Chia et al. (2009) suggested that the enthesis redistributes compressive forces, thus the pathogenesis of plantar fasciitis includes shear and compressive forces (19). According to a series of studies performed by D’Ambrogi and colleagues, plantar fasciitis causes the fascia to thicken which in turn increases stiffness of the medial longitudinal arch resulting in an increase in plantar pressures during gait. However, this relationship was seen in diabetic participants, which made the authors speculate as to whether the increase in pressure had a systemic or a mechanical origin (20-22).
Even though several studies have been performed and various hypotheses have been presented throughout the years, further investigation is necessary in order to determine the exact pathophysiology of plantar fasciitis and whether ground reaction force and regional loading of the foot is altered in this syndrome. Therefore, the aim of this study was to investigate any possible differences in plantar heel pressure between participants with chronic plantar fasciitis and participants with no history of plantar fasciitis in order to clarify the existing dilemma regarding the possible aetiology of this condition.
Materials and Methods
Permission and ethical approval was obtained by the University Research Ethics Committee. The first fifteen adult participants with chronic plantar fasciitis were selected from a Health Centre via purposive sampling and invited to participate. (23, 24).
Eur J Pod 2017; 3 (1): 1-7
Another fifteen adult participants with no history of plantar fasciitis were selected and matched for age, gender and weight to the participants in the plantar fasciitis group. Exclusion criteria included any lower limb musculoskeletal abnormalities (such as foot deformity, morton’s neuroma, tarsal tunnel syndrome, sesamoiditis and concurrent musculoskeletal foot pain) and any neurological or systemic conditions (such as rheumatoid arthritis and other arthritides, diabetes mellitus and neuropathy) which could alter gait and influence plantar pressure distribution.
A Tekscan HR Mat System (Tekscan, Boston, USA) was used to collect plantar pressure data. Before the data collection process commenced, participants were weighed in order to calibrate the system according to manufacturer’s instructions. All participants underwent a period of acclimatisation prior to testing. Each participant was instructed to stand exactly two steps behind the HR Mat™ and the two-step method was utilised, as studies have demonstrated that this protocol is the most reliable and repeatable, resulting in valid and comparable data (25-27).
Three correct trials were obtained at the participants’ own preferred speed, recording heel peak plantar pressure, medial heel peak plantar pressure, lateral heel peak plantar pressure and forefoot peak plantar pressure. The forefoot-to-rearfoot (F/R) plantar pressure ratio was calculated in order to evaluate any possible shift in pressure in the presence of plantar fasciitis (28).
Statistical analysis was performed using Statistical Package for Social Sciences Version 18. All Kolmogrov-Smirnov p-values exceeded the 0.05 level of significance, denoting that all variables had a normal distribution; thus Independent Sample T-Test and Levene’s Test for peak plantar pressures and F/R ratio measurements were utilised.
Results
Thirty participants (7 males, mean age 46years, mean weight 85.1kg and 8 females, mean age 47years, mean weight 71.75kg for the plantar fasciitis group; and 7 males, mean weight 83.6Kg and 8 females, mean weight 71kg, all with a mean age of 45years in the control group) were recruited.
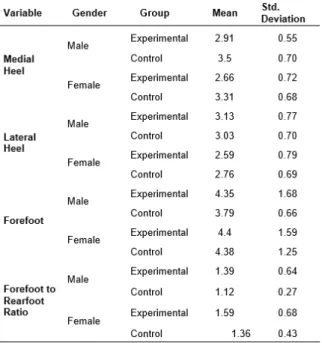
When analysing peak plantar pressures the p -values of the Levene’s test for equality of variances exceeded the 0.05 level of significance, thus equal variances were assumed. The Independent Sample T-Test showed that there were no significant differences between the experimental group and the control group in heel peak plantar pressure (p = 0.244), lateral heel peak plantar pressure (p = 0.867) and forefoot peak plantar pressure (p = 0.576).
However peak plantar pressure at medial heel was significantly higher in the control group when compared to patients with plantar fasciitis (p =
0.015) .
When analysing the F/R ratio measurements the p -value of the Levene’s test for equality of variances was p = 0.696 thus equal variances were assumed. The Independent Sample T-Test for F/R measurement demonstrated there was no significant difference between the experimental group and the control group (p = 0.142).
Table 1. Summary of Variable Distributions
Discussion
The most surprising result arising out of this study is that medio-plantar heel peak pressure was significantly less in participants with plantar fasciitis than in asymptomatic participants (p = 0.015), effectively negating the preconception that there could be an increase in pressure in symptomatic patients.
In agreement with some previous studies (14-18), this study has confirmed that there was no significant difference in peak plantar pressure between participants and control group. This conversely refutes those other studies that attribute this condition with increased pressure (20-22).
Many clinicians often assume that the major contributing factor of this condition is an increase in pressure, which needs to be deviated from the symptomatic region or minimised for the condition to improve (19-22). Indeed, in the clinic, heel cushions and heel cups are popular initial treatment modalities for most types of heel pains. However, the effectiveness of this intervention is poorly understood (29-32).
Following the high prevalence of plantar fasciitis, but lack of evidence in research, the need to conduct this study was deemed important.
The analysis of heel peak plantar pressure (p = 0.244), lateral heel peak plantar pressure (p = 0.867), forefoot peak plantar pressure (p = 0.576) and F/R ratio (p = 0.242) shows that there is no compensation or shift in pressure from the symptomatic region to other areas of the foot during gait. This result does not conform with the study by Wearing, Smeathers and Urry (2003) who concluded that pressure in the forefoot elevates as a protective mechanism to the painful rearfoot region (33).
This result does not conform to the hypothesis of vertical compression which is claimed to cause an increase in pressure, resulting in plantar fasciitis (19-22). As discussed previously, various researchers have speculated that plantar fasciitis may be due to longitudinal traction, that is, increased tensile forces acting on the plantar fascia during gait and dysfunction of the windlass mechanism (13-18). However excessive tensile forces may not only exist due to overpronation and lowering of the medial longitudinal arch (12) but also due to excessive supinatory forces and pescavus (2, 13, 34). Obesity may result in greater flattening of the medial longitudinal arch which in turn creates further tensile forces on the plantar fascia (9, 35-37).
Eur J Pod 2017; 3 (1): 1-7
As regards the management of these painful, and often chronic, heel conditions, clinicians should initially investigate the true nature of the causative factor, whether pressure related or due to tension. Once plantar fasciitis is suspected, treatment strategies apart from cushioning should be considered. One should also have a high clinical suspicion of plantar fasciitis if management with cushioned pads has not been effective after a prolonged period of use.
Like other studies, this study had some limitations, the major one being the small sample size which however was due to the difficulties encountered in recruiting and matching participants. Additionally, the controlled laboratory protocol adopted, in order to conform with other study protocols, may have altered participants’ gait, possibly also affecting the results.
Conclusions
Results of this study confirm there is no relationship between heel peak plantar pressure and plantar fasciitis. These results, combined with other scientific data already found in literature, suggest that peak pressure does not play a part in the pathophysiology of this painful multifactorial condition, and some other internal compensatory mechanism may be present.
References
1. Sweeting D, Parish B, Hooper B, Chester R. The effectiveness of manual stretching in the treatment of plantar heel pain: A systemic review. J Foot Ankle Res, 2011; 19:(4).
2. Panchbhavi VK. (2010). Plantar Heel Pain. Retrieved August, 16, 2011, from, http://emedicine.medscape.com/article/1233178-overview#a0199
3. Lemont H, Ammirati KM, Usen N. Plantar Fasciitis. A Degenerative Process (Fasciosis) Without Inflammation.J Am Podiatr Med Assoc 2003; 93(3): 234-237.
4. Riddle DL, Pulisic M, Pidcoe P, Johnson RE.
Risk factors for plantar fasciitis: A matched
case-control study. J Bone Joint Surg Am, 2003; 85(5), 872–877.
5. Changemail R, Rodrigues PA, Van Emmerik R, Hamill J. Multi-segment foot kinematics andground reaction forces during gait of individuals with plantar fasciitis. J Biomech, 2014; 40(1): 274-277.
6. Hunt GC, Sneed T, Hamann H, Chisam S. Biomechanical and histiological considerations for development of plantar fasciitis and evaluation of arch taping as a treatment option to control associated plantar heel pain: A single-subject design. The Foot, 2004; 14: 147-153.
7. Martinelli N, Bonifacini C, Romeo G. Current therapeutic approaches for plantar fasciitis. Orthop Res Rev, 2014; 6: 33-40.
8. Thomas JL, Christensen JC, Kravitz SR, Mendicino RW, Schuberth JM, Vanore JV, Weil LS, Zlotoff JL, Bouché R, Baker J. The diagnosis and treatment of heel pain: A clinical practice guideline. J Foot Ankle Surg, 2010; 3(49): 1-19. 9. Conti, S.F. & Jain, D.K. (2009). Managing plantar fasciitis and plantar heel pain. J Musculo Med, 26(3).
10. Hicks JH. The mechanics of the foot: The plantar aponeurosis and the arch. Journal of Anatomy, 1954; 1(88); 25-30.
11. Fuller EA. The windlass mechanism of the foot: A mechanical model to explain pathology. JAPMA, 200; 1 (90): 35-46.
12. Aranda Y, Munuera PV. Plantar fasciitis and its relationship with hallux limitus. J American Pod Med Assoc, 2014; 104(3): 263-268.
13. Young C. (2014). Plantar fasciitis. Retrieved
July, 12, 2014, from,
http://emedicine.medscape.com/article/86143-overview
14. Ribeiro AP, Trombini-Souza F, Tessutti VD, Lima FR, João SMA, Sacco ICN. The effects of plantar fasciitis and pain on plantar pressure distribution of recreational runners. ClinBiomech, 2011; 2(26): 194-199.
15. Lorkowski J, Hladki W, Galicka-Latala D, Trybus M.
Brongel L. Underfoot pressure distribution of female
patients with obesity and plantar fasciitis. PrzeglLek, 2009; 66(9): 513-518.
16. Liddle D, Rome K, Howe T. Vertical ground reaction forces in patients with unilateral plantar heel pain: A pilot study. Gait & Posture, 2000; 1(11): 62-66.
17. Bedi HS, Love BR. Differences in impulse distribution in patients with plantar fasciitis. Foot Ankle Int, 1998; 19(3): 153-156.
18. Kelly A, Wainwright A, Winson I. Spur formation and heel pain. ClinOrthopRelat Res, 1995; (319): 330.
19. Chia JKK, Suresh S, Kuah A, Ong, JLJ, Phua JMT. Seah, AL. Comparative trial of the foot pressure patterns between corrective orthotics, formthotics, bone spur pads and flat insoles in patients with chronic plantar fasciitis. Annals Academy of Medicine, 2009; 38: 869-875.
20. Giacomozzi C, D’Ambrogi E, Uccioli L, Macellari V. Does the thickening of Achilles tendon and plantar fascia contribute to the alteration of diabetic foot loading? ClinBiomech, 2005; 5(20): 532-539.
21. D’Ambrogi E, Giacomozzi C, Macellari V, Uccioli L. Abnormal foot function in diabetic patients: the altered onset of Windlass mechanism. Diabetic Medicine, 2005; 12(22): 1713-1719.
22. D’Ambrogi E, Giurato L, D’Agostino MA, Giacomozzi C, Macellari V, Caselli A, Uccioli L.Contribution of Plantar Fascia to the Increased Forefoot Pressures in Diabetic Patients. Diabetes Care, 2003; 5(26): 1525-1529.
23. Trochim WMK. Research Methods Knowledge Base: Descriptive Statistics (3rd ed.). Mason, OH: Thomson, 2006. 24. Patton MQ. Qualitative evaluation and research methods (2nd ed.). California: Sage Publications, 1990.
25. Chevalier TL, Hodgins H, Chockalingam N. Plantar pressure measurements using an in-shoe system and a pressure platform: A comparison. Gait & Posture, 2010; 3(31): 397-399.
26. Van der Leeden M, Dekker JHM., Siemonsma PC, Lek-Westerhof SS, Steultjens MPM. Reproducibility of plantar pressure measurements in patients with chronic arthritis: A comparison of one-step, two-step, and three-step protocols and an estimate of the number of measurements required. Foot Ankle, 2004; 10(25): 739-744.
Eur J Pod 2017; 3 (1): 1-7
28. Caselli A, Pham H, Giurini JM, Armstrong DG, Veves
A. The forefoot-to- rearfoot plantar pressure ratio is
increased in severe diabetic neuropathy and can predict foot ulceration. Diabetes Care, 2002; 6(25); 1066-1071. 29. Rosenbaum AJ, DiPreta JA, Misener D. Plantar heel pain. Med Clin North Am, 2014; 98(2): 339-352.
30. Crawford F, Thomson CE. Interventions for treating
plantar heel pain. Cochrane Database System
Revision, 2010: (1) CD000416.
31. Cotchett MP, Landorf KB, Munteanu SE. Effectiveness of dry needling and injections of myofascial trigger points associated with plantar heel pain: A
systematic review. J Foot Ankle Res, 2010; 18(3).
32. Michelsson O, Konttinen YT, Paavolainen P, Santavirta S. Plantar heel pain and its 3-mode 4-stage treatment. Modern Rheumatology, 2005; 5(15): 307-314. 33. Wearing SC, Smeathers JE; Urry SR. The effect of plantar fasciitis on vertical foot-ground reaction force. ClinOrthopRel Res, 2003; (409), 175-185.
34. Bolgla LA, Malone TR. Plantar fasciitis and the windlass mechanism: A biomechanical link to clinical practice. J Athl Train, 2004; 39(1): 77-82.
35. Borrelli AH. Percutaneous plantar fasciotomy for the surgical treatment of refractive plantar fasciitis. Tech Foot Ankle Surg, 2011; 2(10): 49-55.
36. Kiritsi O, Tsitas K, Malliaropoulos N, Microulis G. Ultrasonographic evaluation of plantar fasciitis after low-level laser therapy: Results of a double-blind, randomized, placebo-controlled trial. Lasers in Medical Science, 2010; 2(25): 275-281.