Price Regulation in the Pharmaceutical Industry
Pharmaceutical price negotiations and copayments
In this study, we analyze the influence of patient contributions on the purchase of medicines on the price of a medicine. In particular, we believe that when the price is negotiated, the drug is quoted for the proportionate reimbursement by the patient. Indeed, the monopolist has more to gain from negotiations when patient demand is less price-elastic, ie when the level of co-payment is lower.
It is assumed that the total patient demand for the drug is reduced by the co-payment, which is proportional to the full price of the drug. In particular, we believe that in price negotiations, the drug is listed for proportionate reimbursement to patients.

Parallel imports and copayments
Therefore, the monopolist increases the price in the low-price country and lowers the price in the high-price country to discourage a certain amount of parallel imports. In this situation, the increase in consumer surplus in the high-price country more than offsets the decrease in the low-price country, and parallel trade increases total welfare. Parallel imports would cause people with a low valuation in the low-cost country to give up consuming the drug.
While in the high price country, people with a higher value start consuming the drug thanks to parallel trade. Therefore, banning parallel trade would provide a Pareto improvement by opening the market in the low-cost country without harming the market in the high-cost country (Hausman and MacKie-Mason 1988).
External referencing
We focus exclusively on the role of the level of surcharges in determining whether or not a country should engage in external referral. We assume that such patient co-payments are a fixed amount and do not depend on the final price of the drug. In approaching this question, we examine how a country's commitment to external referencing affects drug price negotiations in the reference country and ultimately determines the firm's profits.
This is troublesome, since one of the limitations of this study is that we have no real-world information about the company's point of disagreement when it bargains with a country, say F, if that country is later used as an external reference. from another country, Say N. This is a standard form of a "take it or leave it" offer and is the actual threat to the company in the case of the Netherlands. If the company respects the maximum reference price set by N, the drug is listed for reimbursement in country N, regardless of previous history. 2 Commitment and bargaining power are related but should not be confused.
Combining each of the three possibilities (a) to (c) with assumptions 1 to 3, we obtain the following three reference price policies: i) The strictest combines assumptions 1 to 3 with 4-a. The situation with an unconditional price limit shows in a very extreme way what the problem with external reference can be: it weakens the bargaining power of the reference country. Outsourcing country N improves the company's bargaining power relative to country F.
This is a key difference compared to the other two cases, as it means that in a one-on-one negotiation between a firm and country F, the point of disagreement is the same as if there were no external reference. In this case, the policy greatly improves the firm's shares, and the resulting negotiated price in F is lower than without the external reference. This is very similar to our result in the case of a weak conditional price constraint: the bargaining power of the reference country deteriorates under the external reference.
Strategic sequence of drug launches
The main difference between Pecorino's paper and ours is that it ignores the possibility of the US independently negotiating the price of its home with the company. If a company is aware that another country will use information disclosed in the first country, it will carefully choose which country to enter first. In these circumstances, the company can prevent the disclosure of this information by changing the launch sequence.
To be more precise, the circumstances in which the preceding argument rests are determined by several parameters: first, the co-payment levels in each country, which determine individual demand; second, the size of each country's population, which is a level effect that determines aggregate demand; third, the company's intertemporal discount rate, which determines the costs of strategically delaying launch in a high-demand country; fourth, the intertemporal discount rate of each agency, which determines the agency's benefits to attract an early departure; and finally, each country's prior beliefs about the company's true costs of production that determine the agencies' assessment of the risk of a high-cost company rejecting a low-price offer. We focus on a specific case where the following three hypotheses apply: (i) country A has a larger population than country B, (ii) individuals in country A have a lower payment for the drug than individuals in B, (iii) ) that of the company The discount rate is less than 1. Underlying this is the idea that the country with low demand cannot risk offering a low price, as the efficient company would reject it to hide its costs truths about the future country in high demand.
The research indeed shows that in this case the company prefers to enter the small demand country first. The reason is that Danzon assumes that information spillovers will occur and therefore the natural choice for the impatient company (since prices will be low anyway) is to enter the high demand country first and wait with the entering the low demand country. This argument ignores the fact that being the first to enter the small country can prevent information spillovers to the benefit of the company.
The crucial assumptions for the main result are: first, that countries differ in copayment rates; second, that the agency in the country with a large population/low excess (A) has a discount rate below one. 3If prior beliefs are very high, both countries offer low prices and the company is indifferent to all possible launch sequences. If prior beliefs are very low, both countries will offer a high price and then the company will choose to launch first in the country with high demand.
International sharing of R&D expenses
A provider who accepts such conditions may enroll in the network of the managed care organization. In the first stage, the third-party payer (be it an NHS or private insurance companies) offers health insurance contracts to consumers. Finally, in the third stage of the game, suppliers compete in prices and qualities in the market.
In the first phase of the game, individuals face several possible situations (for example, being healthy or sick). The optimal value of the price to be announced in the "any willing supplier" contract is the lowest price that makes it possible for both suppliers to accept it. Accordingly, prices will be lower than the price required in the case of "any willing supplier" to generate the acceptance outcome.
If the surplus per capita grows (decreases) with the number of providers in the market, then “every willing provider” should be observed more often (less). We assume that the profits of both providers weigh equally in the objective function of the association. Therefore, empirical assessments of the role of unused capacity in the public sector should take into account whether negotiations with the private sector exist.
The main finding of the analysis is that whenever the surplus to be shared in the agreement is relatively high, the third-party payer prefers the "any willing provider" system. This is so because simply announcing the price in the case of "any willing bidder" constitutes an implicit commitment to be tough. Price Discrimination for Pharmaceuticals: Welfare Effects in the US and the EU.” International Journal of Business Economics.
Negotiation Mechanisms in Healthcare Markets
Bargaining in healthcare markets
- Introduction
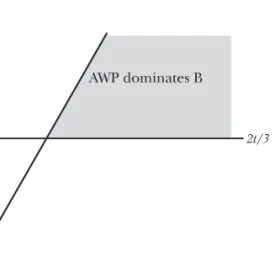
- Choosing between AWP and simultaneous bargaining
- Explicit simultaneous bargaining
- The preferred negotiation format
- Extension 1: Maintaining idle capacity
- Extension 2: Bargaining with an association
- Extension 3: Providers competing for partners
"Any willing provider" contracts cause the third-party payer to announce a price and leave (symmetric) providers the option of joining the deal.12 Providers are assumed to be equal in relevant dimensions except for location in the feature space. and (possibly) prices. This optimal price is also lower than the cost per unit distance when no provider is located at the preferred point of the characteristic space t, which guarantees that the third payer pre-. Consider now the case when only an offeror accepts the price determined in the negotiation process.
In other words, we enforce a conservative behavior on the third party payer, in the sense that we do not allow it to announce a price in the inter-. The gain to the NHS from negotiation is given by the difference in the net surplus under negotiation. Otherwise, in the absence of capacity constraints and equal efficiency in public and private facilities, the third-party payer would trivially only provide treatment in the public sector.
In the capacity subgame, decisions take into account the continuation of the game and how they will affect the negotiated price. 18 Further details on the role of health care provider associations are presented in the next section. In such a circumstance, the third-party payer would prefer to buy in the private market.19 Each of these marginal changes in return values resulting from capacity decisions is weighed by the bargaining power of each party.
Negotiating with the most efficient provider is better when the third-party payer, after failing to negotiate with the more efficient provider, negotiates with the less efficient provider and excludes the former from coverage. Due to the elements of moral hazard involved in health insurance contracts, third-party payers implement mechanisms to control costs. With the first, the country approves the importation of drugs by a third party, even without the consent of the patent holder.
In the latter case, the terms of the contract are announced by the third-party payer, and providers either accept the terms and join the network of providers affiliated with that third-party payer, or they decline and stay out of the network. She has held academic positions at the University of East Anglia (UK) and City University London (UK).
Findings