www.elsevier.es/rmuanl
ORIGINAL
ARTICLE
Risk
factors
and
the
relation
of
lactic
acid
to
neonatal
mortality
in
the
first
week
of
life
I.
Rodríguez-Balderrama
∗,
P.J.
Ostia-Garza,
R.D.
Villarreal-Parra,
M.
Tijerina-Guajardo
NeonatologyServiceatthe‘‘Dr.JoséEleuterioGonzález’’UniversityHospitaloftheAutonomousUniversityofNuevoLeónin Monterrey,NuevoLeón,Mexico
Received19August2015;accepted17December2015 Availableonline8May2016
KEYWORDS Lacticacid; Neonatalmortality; Preterm;
Mechanical ventilation; Mexico
Abstract
Objective: Todeterminetherelationshipbetweenlacticacidlevelsandneonatalmortalityin thefirstweekoflife,inpatientsadmittedtotheNeonatalIntensiveCareUnit(NICU)ofthe ‘‘Dr.JoséE.González’’UniversityHospital.
Materialandmethods: Prospective,observationalanddiagnostictestperformedinthe neona-talwardofthe‘‘Dr.JoséEleuterioGonzález’’UniversityHospital.Weincludedalllivepreterm infantsonmechanicalventilationwhowereadmittedtotheNICUfromNovember1,2011to October31,2012.
Results:Onehundredandfiftyfourpatientsmettheinclusioncriteria.At72h,wefoundthat thebestsensitivity(95%)waswhenlactatewaslessthan1.5mmol/landthebestspecificity (89%)waspresentwhenlactatelevelsweregreaterthan2.5mmol/l.ThepH<7.25hada sen-sitivityof76%andspecificityof96%.At168h(7days)wefoundthatthebestsensitivity(91%) waswhenlactatelevelswerelessthan1.5mmol/l,andthatthebestspecificity(96%)waswhen lactatelevelsweregreaterthan2.5mmol/l.WefoundthatthepH<7.25hadasensitivityof 36%andspecificityof91%.
Conclusion: Thelactateserum,at1.5mmol/l,hasasensitivity(tobekilled)of95%onthethird dayand91%ontheseventhday.WhenthepHisgreaterthan7.25thereisaspecificity(tobe alive)of96%onthethirddayand91%ontheseventhday.67%ofthedeadwereunder1500g, andwere61%under28gestationalweeks.
©2016PublishedbyMassonDoymaM´exicoS.A.onbehalfofUniversidadAut´onomadeNuevo Le´on.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons. org/licenses/by-nc-nd/4.0/).
∗Correspondingauthorat:ServiciodeNeonatologíadelHospitalUniversitario‘‘Dr.JoséEleuterioGonzález’’delaUANL,AvenidaFrancisco
IMaderoyGonzalitos,s/n,Col.MitrasCentro,códigopostal64460Monterrey,N.L.,Mexico.
E-mailaddress:[email protected](I.Rodríguez-Balderrama).
http://dx.doi.org/10.1016/j.rmu.2015.12.001
Introduction
Lactic acid is a terminal product of the anaerobic metabolismofglucose,anditisobtainedbyareductionof pyruvicacidinareactioncatalyzedbythelactic dehydro-genaseenzyme,whereadinucleotideadeninenicotinamide (NAD)coenzymegoesfromitsreducedformtoitsoxidized form.1---3
Undernormalconditions,serumlevelsareat2mEq/Lor lower.However,exercisecanelevateitupto4mEq/L.Most lactateisefficientlyeliminatedbytheliverandisutilizedin gluconeogenesisorintheproductionofenergy.When con-siderableincreasesinlactateserumnumbersareproduced, withareductioninlactatetopyruvatemetabolism conver-sion,metabolicacidosisoccurs,whichisusuallysevereand mayleadtopatientdeath.4
Lactic acid is increased in situations of tissue hypoxia---ischemia.Different studies conductedin adults,5 aswellasinchildren6,7andnewborns,8haveshownthatin criticalsituations,lacticacidlevelsatthemomentofthe patient’s admittance tothe ICU and its evolution have a positivecorrelationwiththeriskofdeath.9
Lactic acid can increase for several causes other than tissuehypoxia.Within thecontext ofthe ICU, inorderof frequency,amongstthemost probablearethoseof hemo-dynamiccauses,10 whichdetermine tissuehypoxia,11 asin the case of sepsis, heart failure, shock (cardiogenic and septic)andmultipleorgandysfunction.11Amongstthe non-hemodynamic causes thereare12,13: the useof biguanides in diabetic patients, the use of pharmaceuticals such as adrenalin and nitroprusside, seizures, intestinal infarc-tion, or in general, patients with intestinal hypomotility, shortbowels,thiaminedeficiency,liverdiseasesingeneral, ethanoloverdoses,methanol,salicylatesandethylene gly-col.
Lactate has proven to be a good prognostic indica-tor in hospitalized adults and children14,15 and different typesofpatients,includingcritical,16---18andsurgical,19with sepsis20,21 and trauma.22,23 Itsmain advantageis howfast andeasyitsdeterminationis,anditsevolutionaryprognosis capability.24,25
Theobjectiveofthisstudyistodeterminethe relation-ship of lacticacid levelswith neonatalmortality rates in thefirstweekoflife,inpatientsadmittedtotheNeonatal IntensiveCareUnitatthe‘‘Dr. JoseE. Gonzalez’’ Univer-sityHospital,aswellastoquantifyneonatalmortalityrate prevalenceinthefirstweekoflifeinrelationtolacticacid levels,toknownon-pathologicalandpathologicalmaternal backgrounds,learnthenewborn’scharacteristics, to iden-tifythe main in-hospital morbidities, document the main causesofassociateddeath,andidentifylactatelevels asso-ciatedandahighermortalityrate.
Materials
and
methods
Aprospective, observational and diagnostic test was per-formed in the neonatal ward of the ‘‘Dr. José Eleuterio González’’University Hospital of the Autonomous Univer-sity of Nuevo León. We included all live preterm infants onmechanicalventilation whowereadmittedtotheNICU withintheperiodofNovember1,2011toOctober31,2012.
ThestudywasapprovedbytheUniversity’sEthics Commit-teewiththefoliono.NE12-003.
Exclusioncriteriaincluded alllivepreterm infantswho didnotrequiremechanicalventilationadmittedtotheNICU betweenNovember1,2011andOctober31,2012,patients transferredfromotherhospitalunits,andthosewhodidnot meettherequirementsofthefile.
Variableswere the following: theevaluatednewborns’ characteristicswereweightatbirth,andwereclassifiedinto <1000g, 1001---1500g, 1501---2500g and 2501---4000g cate-gories. Also,gestational age wasevaluated and classified accordingtothenumberofweeksofgestationas<28weeks, 28---33weeks,and34---36weeksofgestation.Trophismwas evaluatedandclassifiedasadequateweightforgestational ageandlowweightforgestationalage.26Theyweredivided bymaleandfemale,accordingtogender,andwere evalu-atedandclassifiedaccordingtotheirAPGARscoreat5min in0---3,4---6and7---10points.
Withinthesevariables,the studyincluded pathological andnon-pathologicalmaternalfamilyhistory:nofamily his-tory,smoking,alcoholism,drugaddictionandtattoosonthe mothers of the newborns, the number of sexual partners wasstudied,dividedintoone,two,threeormore. Accord-ing to the mother’s health during pregnancy, they were dividedintohealthy, or whetherthemotherpresentedan ailment,suchashighbloodpressure,infections, preeclamp-sia,eclampsiaorgestationaldiabetes,amongothers.Also, itwasdeterminedwhetherornotthepatientscarriedout properprenatalcare.
Additionally,themothers’agewasevaluatedanddivided asfollows:under18yearsold,from19to30yearsold,and over 30 yearsold.Theywere dividedintosingle,married and the consensual union, according to theirmarital sta-tus.Regardingschooling,theclassificationswereilliterate, elementary,juniorhighschool,highschool,andbachelor’s degree. Also, a classification according to their occupa-tionwasmade,dividingthemasfollows:housewife,worker and student. Among the evaluatedvariables were causes ofin-hospitalmorbidityandmortality,fromwhichthe fol-lowingpathologieswerestudied:hyalinemembranedisease grades 1 through 4, pulmonary edema, meconium aspira-tion syndrome,septic shock, sepsis, extreme prematurity andperinatalasphyxia.
LactateandpHwerestudiedat72h (3days),assessing sensitivity, specificity, positive predictive value and nega-tivepredictivevalueoflactatelevels>1.5mmol/l,2mmol/l and lactate at 2.5mmol/l, as well as pH <7.25 and <7.30.
Similarly,lactateandpHwerestudiedat168h(7days), assessing sensitivity, specificity, positive predictive value andnegativepredictivevalueoflactatelevels>1.5mmol/l and2mmol/landlactateat2.5mmol/l,aswellaspH<7.25 and<7.30.
Qualitativevariableswereusedinthestatisticalanalysis. Thechisquare(non-parametric)testswereutilizedtotest thehypothesis.Analphavalueof0.05wasusedandthenull hypothesiswasrejectedwhenthecriticalvaluewasunder 0.05.
Sensitivity, specificity, and both positive and negative predictionvaluesweredeterminedwitha2×2contingency
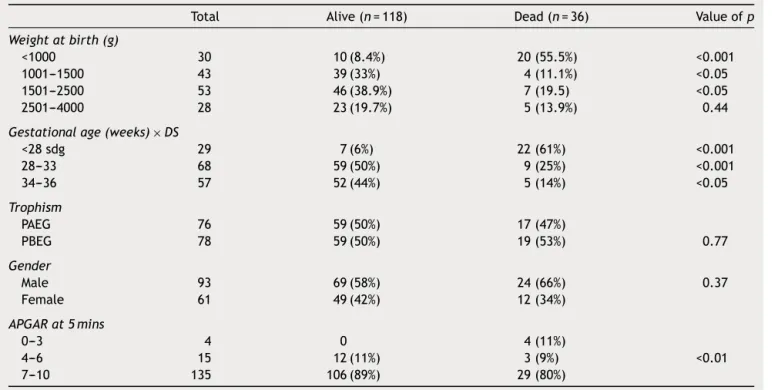
Table1 Newborncharacteristics.
Total Alive(n=118) Dead(n=36) Valueofp Weightatbirth(g)
<1000 30 10(8.4%) 20(55.5%) <0.001 1001---1500 43 39(33%) 4(11.1%) <0.05 1501---2500 53 46(38.9%) 7(19.5) <0.05 2501---4000 28 23(19.7%) 5(13.9%) 0.44
Gestationalage(weeks)×DS
<28sdg 29 7(6%) 22(61%) <0.001
28---33 68 59(50%) 9(25%) <0.001
34---36 57 52(44%) 5(14%) <0.05
Trophism
PAEG 76 59(50%) 17(47%)
PBEG 78 59(50%) 19(53%) 0.77
Gender
Male 93 69(58%) 24(66%) 0.37
Female 61 49(42%) 12(34%)
APGARat5mins
0---3 4 0 4(11%)
4---6 15 12(11%) 3(9%) <0.01
7---10 135 106(89%) 29(80%)
were lactate levels >1.5mmol/l, 2mmol/land lactate at 2.5mmol/l,aswellaspH<7.25and<7.30.
Results
Withintheperiodoftimeoutlinedinthisstudy,therewere 2657births.363(13.6%)ofthesewereadmittedtotheNICU. Outofthe363admittedtotheNICU,226(67.2%)were pre-mature.Outoftheprematureones,154mettheinclusion criteria,fromwhich36diedand118survived.
When comparingtheir weight at birth, we areable to findthatthereweremorechildrenunder1000ginthedead group (p<0.001) and there were more children between 1000and2500ginthealivegroup(p<0.05).Regarding ges-tational age, there were more children under 28 weeks of gestation in the dead group with (p<0.001) and more children with a gestationalage of 28---33 weeks of gesta-tion(p<0.001)and34---36weeksofgestation(<0.05)inthe alivegroup.Concerning trophismand gender,both groups were similar (NS). When comparing APGAR scores, there weremoredeadchildrenwithalowAPGAR(p<0.001)(see Table1).
When comparing non-pathological and pathological maternalhistory,weareabletofindthatthereweremore mothers without anyhistory in thealive group (p<0.001) and there was a greater link of alcoholism (<0.05), drug addiction(<0.05)andtattoos(<0.001)inmothersofthose patientswhodied.Regardingthenumberofsexualpartners, thosewith3ormoresexpartnerswerehigherinthedead group(<0.05).
When comparingthemothers’healthduringpregnancy, resultsshowthatinthedeadgroupthereweremoremothers withhighbloodpressure(<0.001)andgestationaldiabetes (p<0.05) and the presence of infections, preeclampsia,
eclampsiaandotherdiseaseswasnotsignificant(NS). Pre-natalcarewassimilarinbothgroups(NS)(seeTable2A).
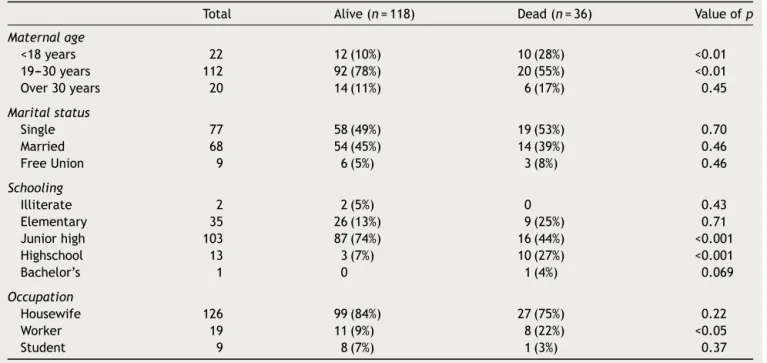
When comparingassociatedmaternal age, weareable toobservemore mothers<18 yearsoldinthedead group (p<0.01) andmore mothersbetween 19and 30yearsold (p<0.01) in the alive group. Maritalstatus was similarin both groups (NS). Regarding schooling, there were more childrenin the dead groupwhose mothers hascompleted highschool(p<0.001),whereasinthealivegroup elemen-taryschoolwaspredominant(p<0.001).Thereweremore workingmothersinthedeadgroup(p<0.05)(seeTable2B). When comparing in-hospital morbidity and mortality causes,weareabletoobservethatthereweremoredead childrenwithgrade3and4hyalinemembranedisease diag-nosis (p<0.001), septic shock (p<0.01) and prematurity (p<0.001). On the other hand, sepsis was higher in the alivegroup(p<0.05).Thepresenceofgrade1and2HMD, pulmonaryedema,meconiumaspirationsyndromeand peri-natalasphyxiawerenotsignificant(NS)(seeTable3).
At72h,findingsshowthebestsensitivity(95%)waswhen lactatewaslowerthan1.5mmol/landthebestspecificity (89%) waswith lactatelevels higher than 2.5mmol/l; pH <7.25hadasensibilityof76%andaspecificityof96%(see Table4).
At 168h (7 days), findings show the best sensitivity (91%)waswhenlactatewaslowerthan1.5mmol/landthe bestspecificity (96%) was with lactatelevels higher than 2.5mmol/l;pH <7.25hadasensibilityof36% anda speci-ficityof91%(seeTable5).
Discussion
Table2A Pathologicalandnon-pathologicalmaternalantecedents.
Total Alive(n=118) Dead(n=36) Valueofp Non-pathologicalantecedents
None 119 104(88%) 15(42%) <0.001
Smoking 13 7(6%) 5(14%) 0.10
Alcoholism 5 2(2%) 3(8%) <0.05
Drugaddiction 11 5(4%) 6(16%) <0.05
Tattoos 7 0 7(20%) <0.001
Numberofsexualpartners
One 148 115(97%) 33(92%)
Two 4 3(3%) 1(2%) <0.05
Threeormore 2 0 2(6%)
Maternalhealthduringpregnancy
Healthy 115 92(77%) 23(64%) 0.089
Art.hypertension 8 2(2%) 6(17%) <0.001
Infections 2 2(2%) 0 0.88
Preeclampsia 12 9(8%) 3(9%) 0.43
Eclampsia 2 2(2%) 0 0.88
Gestationaldiabetes 5 2(2%) 3(9%) <0.05
Other 10 9(8%) 1(4%) 0.30
Prenatalcontrol
Yes 135 102(85%) 33(92%) 0.40
No 19 16(14%) 3(8%)
levels are at 2mEq/L or lower.4 Lactic acid is increased in situations of tissue hypoxia---ischemia,5---8 and its levels haveahighcorrelationwithmortality.9---11Thecauseswhich provokean increaseoflacticacidcanbehemodynamicor non-hemodynamic.12---25
Thenumberofprematurebirthscontinuestoincreasein developedcountries,aswellastherelatedlowweight,with anincreasedmortalityrateforpatientsthatweighlessthan
1500g.27,28Withinthefindingsofourstudy,whencomparing weightatbirth,wefoundthatthereweremorechildrenthat weighedlessthan1000ginthedeadgroup.
A very important relation between a high number of deaths and a gestational age of 28---31 weeks has been reported in various studies, showing that they present a higherriskofcomplicationsandmortalityduringtheirtime in the NICU.28,29 Within our findings, upon comparison of
Table2B Pathologicalandnon-pathologicalmaternalantecedents.
Total Alive(n=118) Dead(n=36) Valueofp Maternalage
<18years 22 12(10%) 10(28%) <0.01 19---30years 112 92(78%) 20(55%) <0.01
Over30years 20 14(11%) 6(17%) 0.45
Maritalstatus
Single 77 58(49%) 19(53%) 0.70
Married 68 54(45%) 14(39%) 0.46
FreeUnion 9 6(5%) 3(8%) 0.46
Schooling
Illiterate 2 2(5%) 0 0.43
Elementary 35 26(13%) 9(25%) 0.71
Juniorhigh 103 87(74%) 16(44%) <0.001
Highschool 13 3(7%) 10(27%) <0.001
Bachelor’s 1 0 1(4%) 0.069
Occupation
Housewife 126 99(84%) 27(75%) 0.22
Worker 19 11(9%) 8(22%) <0.05
Table3 Causesofintrahospitalmorbidity.
Total Alive(n=118) Dead(n=36) Valueofp HMD
Degree1and2 8 8(7%) 0 0.10
Degree3and4 89 76(64%) 13(36%) <0.01
PE 8 8(7%) 0 0.10
MAS 1 1(0.9%) 0 0.57
Septicshock 2 0 2(5.5%) <0.01
Sepsis 12 12(10%) 0 <0.05
Extremeprematurity 29 9(7.5) 20(56%) <0.001
Perinatalasphyxia 5 4(3.5%) 1(2.5%) 0.85
Table4 LactateandpHofthepatientsat72h(3days).
Sensibility Specificity VPP VPN
Lactate>1.5mmol/l 95% 60% 35% 98%
Lactate>2mmol/l 83% 76% 45% 95%
Lactate>2.5mmol/l 75% 89% 62% 94%
pH>7.25 76% 96% 82% 94%
pH>7.30 29% 80% 24% 83%
Table5 Lactateandphofthepatientsat168h(7days).
Sensibility Specificity VPP VPN
Lactate>1.5mmol/l 91% 70% 35% 98%
Lactate>2mmol/l 75% 85% 68% 89%
Lactate>2.5mmol/l 52% 96% 86% 83%
pH>7.25 36% 91% 62% 78%
pH>7.30 22% 75% 93% 71%
gestationalages,we foundthat thereweremorechildren at less than 28 weeks (p<0.001) in the dead group, and morechildrenat28---33weeksand34---36weeksinthealive group(p<0.001).
Itisworthconsideringthatsomestudieshavefoundan association between the masculine gender and a risk of death.2,14,16,23---25,27,28 The studies saythat whencomparing genders in relation to mortality, it is commonly observed thatthedeathrateofmalesishigherthanthatoffemalesat allages.Inourstudy,whencomparinggenders,bothgroups weresimilar(NS).
TheAPGARscorehasbeenconsideredanimportant pre-dictivevariableofneonatalmortality.Thisvariableismore directly relatedto thequality ofattention at delivery,in spite of the influence of previous conditionsof the new-born during theintrauterineperiod, which determinesits vitalityatbirth.Thisscorehasbeenmentionedbyvarious authors23---25,27,28 as an important variable which is closely relatedtotheriskofdeathwhenscores oflessthan7are obtainedatthefirstandfifthminutes.Withinourfindings, weobservedthatthereweremoredeadinthelowAPGAR category(p<0.001).
The important increaseof neonataldeathrates dueto thehighprevalenceofprematurebirthsandlowweightat birthhasbeenmentionedinvariousstudies.27,28Theseare
closelyrelatedtootherindicators inthemothers,suchas theintakeofalcohol,tobaccoandillicit drugs.Withinour pathologicalandnon-pathologicalfindingsonthemothers, wefoundthatthemothersofdeceasedpatientspresented a greater relation to alcoholism (<0.05), drug addiction (<0.05)andtattoos(<0.001).
Regarding prematurity, various studies have reported thatitis afactor inrisksassociatedwithneonataldeath, malnutrition,infections, iatrogenicprematurity, hyperten-sionandtheprematureruptureofmembranes,amongother things.17,27---29Inourstudy,weobservedthatthereweremore motherswitharterialhypertension(<0.001)andgestational (p<0.05)diabetesinthedeadgroup.Thepresenceof infec-tions,preeclampsia,eclampsiaandotherdiseaseswerenot significant(NS).
themotherswithlessthan5consultationshavea2.5times higherriskthantheothers.Inthefindingsofourgroup,upon comparisonof prenatal control, both groups were similar (NS).
deFátimaAlmeidaetal.,28 intheirstudyperformedat theFederal University of Espíritu Santo in Brazil, studied neonataldeathsaswellastheriskfactorsassociatedwith them,findingariskofdeath3timeshigherinmothersthat wereless than15yearsold(OR=2.97;IC95%).This bears acloseresemblance toour study,whichfound that there weremoremotherthatwerelessthan18yearsoldinthe deadgroup(p<0.01).
Maternaleducationis considered an indicatorof social status.Themother’slevelofeducationcanbeconsidereda factorrelatedtoherculturalprofileandconductofhealth care, which has an important effect on the determina-tionofmortality.23,27,28Thisinvestigationhasdemonstrated, through an analysis of the correlation between maternal educationandobstetricalindicators,thatthereisa statisti-callysignificantassociationbetweenalowlevelofeducation andlowweightatbirth,anelevatednumberofpremature birthsandalessernumberofprenatalconsultations. Mater-nal educationcan beconsidered to bean obstetrical risk factorforpregnantwomenandnewborns.Theanalysisalso signifiedthatthesignificant associationbetween neonatal mortalityandaninferioreducationwiththesewomenmay beduetolowersocialconditionsandlimitedaccesshealth services.28
Withinthefindingsofourstudy,uponcomparisonof edu-cationallevels,wefoundthattherewereagreaternumber ofchildreninthedeadgroupofmotherswithahighschool education(p<0.001) andthereweremore childreninthe alivegroup of mothers withan elementary school educa-tion(p<0.001).Withinthefindingsofourstudy,wefound that,at 72h, the bestsensitivity (95%)was when lactate waslower than 1.5mmol/land the best specificity (89%) waswithlactatelevelshigherthan2.5mmol/l, whichisin accordancewithmedicalliterature.
Conclusion
Accordingtoourfindings, we canconclude thefollowing: thestudyofriskfactorsinmothersisimportantinorderto preventprematurebirthsas well asitsstrong connection withlowweightatbirthandalowergestationalage,since resultsshowthat67%ofdeathswereunder1500gandthat 61%wereunder28weeksofgestation.
Lactateover1.5mmol/lhasasensitivity(tobedead)of 95%atday3and91%atday7.
WhenpHishigherthan7.25thereisaspecificity(tobe alive)of96%atday3and91%atday7.
Conflict
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Funding
Nofinancialsupportwasprovided.
References
1.GarcíaSC,RupérezL,López-HerceCid,etal.Valorpronóstico delapuntuaciónPIM(Índicepediátricodemortalidad)ydel ácidolácticoenni˜noscríticamenteenfermos.AnEspPediatr. 2002;57:394---400.
2.HaterillM,McIntyreAG,WattieM,etal.Earlyhyperlactataemia incriticallyillchildren.IntensiveCareMed.2000;26:314---8.
3.Singarajah C, Carlson RW. A review of the role of blood lactate measurements in the ICU. J Intensive Care Med. 1998;13:218---28.
4.HenningRJ,WeilMH,WeinerF.Bloodlactateasaprognostic indicatorofsurvivalinpatientswithacutemyocardial infarc-tion.CircShock.1982;9:307---15.
5.Aduen J, Bernstein W, Khastgir T, et al. The use and clinical importance of a substrate-specific electrode for rapid determination of blood lactate concentrations. JAMA. 1994;272:1678---85.
6.SauaiaA,MooreF,MooreE,etal.Earlypredictorsofpostinjury multipleorganfailure.ArchSurg.1994;129:39---45.
7.DrummondAJ, BernardGR, RussellJA. Decreasinglactate is associatedwith lower mortalityin patientswho have sepsis syndrome.Chest.1993;104:157.
8.HatherillM,SajjanharT,TibbySM,etal.Serumlactateas a predictorofmortalityafterpaediatriccardiacsurgery.ArchDis Child.1997;77:235---8.
9.ShimeN,KaageyamaK,AshidaH,etal.Perioperative assess-mentofbloodlactatelevelsinpediatricheartsurgery.Masui. 2001;50:752---7.
10.DeshpandeSA,PlattMP.Associationbetweenbloodlactateand acid---basestatusand mortalityinventilatedbabies.ArchDis ChildFetalNeonatal.1997;76:F15---20.
11.CaridadSM.Acidosisláctica.RevCubanaMed.2000;39:115---9.
12.MizockBA.Controversiesinlacticacidosisimplicationsin criti-callyillpatients.JAMA.1987;258:497---501.
13.SolimanHM,VincentJL.Prognosticvalueofadmissionserum lactateconcentrationsinintensivecareunitpatients.ActaClin Belg.2010;65:176---81.
14.ZhouX,XuZY,FanJH,etal.Relationshipbetweenbloodlactate leveland diseaseseverity in criticallyill children. Zhongguo DangDaiErKeZaZhi.2012;14:114---6.
15.NadeemM,ClarkeA,DempseyEM.Day1serumlactatevalues inpreterminfantslessthan32weeksgestation.EurJPediatr. 2010;169:667---70.
16.BasaranM,Sever K, KafaliE,et al.Serum lactate levelhas prognosticsignificance afterpediatriccardiac surgery.J Car-diothoracVascAnesth.2006;20:43---7.
17.KoliskiA,CatI,GiraldiDJ,etal.Lactatoséricocomomarcador prognósticoemcrianc¸asgravementedoentes.JPediatr(RioJ). 2005;81:287---92.
18.MurtuzaB,WallD,ReinhardtZ,etal.Theimportanceofblood lactateclearance asa predictorofearly mortalityfollowing the modified Norwood procedure. Eur J Cardiothorac Surg. 2011;40:1207---14.
19.BorchersA,WilkinsPA,MarshPM,etal.Associationofadmission l-lactate concentrationin hospitalisedequine neonates with presentingcomplaint,periparturientevents,clinicaldiagnosis andoutcome:aprospective multicentrestudy.EquineVetJ. 2012;44:57---63.
20.MoralesSHN,GarzaAAG,RodríguezVI,etal.Índicesderiesgo demortalidad(PRISMyPIM)enni˜nosconrespectoa la con-centracióndelactatoa suingresoauna UnidaddeCuidados Intensivos.RevMexPediatr.2010;77:111---4.
21.Kirschenbaum LA, Asitiz ME, Rackow HC. Interpretation of bloodlactateconcentrations inpatientswithsepsis.Lancet. 1998;352:921---2.
23.StraneyLD,LimSS,MurrayCJ.Disentanglingtheeffectsofrisk factorsandclinicalcareonsubnationalvariationinearly neona-talmortalityintheUnitedStates.PLoSONE.2012;7:e49399,
http://dx.doi.org/10.1371/journalpone.004939.
24.TomashekKM,Shapiro-MendozaCK,DavidoffMJ,etal. Differ-encesin mortalitybetweenlate-preterm and termsingleton infantsintheUnitedStates.JPediatr.2007;151:450---6.
25.Kramer MS, Demissie K, Yang H, et al. The contribution of mildand moderatepretermbirth toinfant mortality. JAMA. 2000;284:843---9.
26.Rodríguez-BonitoR,Gonzalez-GarciaM.Clasificacióndelrecién nacido.In:RodríguezBR,editor.Manualdeneonatología.2ned. México:McGraw-HillInteramericana;2012.p.4---12.
27.MehaffeyK,HigginsonA,CowanJ,etal.Maternalsmokingat firstprenatalvisitasamarkerofriskforadversepregnancy out-comesintheQikiqtaaluk(Baffin)Region.RuralRemoteHealth. 2010;10:1484.
28.deFátimaAlmeidaLE,InêsSA,HarterGR,etal.Riskfactors forneonatalmortalityinthecityofSerra,EspíritoSanto.Rev BrasEnferm,Brasília.2012;65:578---85.