Efficacy of telaprevir-based therapy in stable liver
transplant patients with chronic genotype 1 hepatitis C
Xavier Forns,1 Didier Samuel,2 David Mutimer,3 Stefano Fagiuoli,4 Miquel Navasa,1 Kosh Agarwal,5 Marina Berenguer,6 Massimo Colombo,7 Kerstin Herzer,8 Frederik Nevens,9 Bjorn Daems,10 Katrien Janssen,10 Sivi Ouwerkerk-Mahadevan,10 Holly Kimko,11 Erkki Lathouwers,10 James Witek,11 Rodica Van Solingen-Ristea11
1 Liver Unit, Hospital Clinic, CIBEREHD and IDIBAPS, University of Barcelona, Barcelona, Spain. 2 Centre Hepatobiliaire, Hospital Paul Brousse, University Paris South Villejuif, Paris, France. 3 Queen Elizabeth Hospital and NIHR BRU, Birmingham, UK. 4 Gastroenterology and Transplant Hepatology Papa Giovanni XXIII Hospital, Bergamo, Italy. 5 Kings College Hospital, London, UK. 6 La Fe University Hospital and Ciberehd, Valencia, Spain. 7 Fondazione IRCCS Ca’Granda Ospedale Maggiore Policlinico, Universita degli Studi di Milano, Milan, Italy. 8 Department of General, Visceral and Transplantation Surgery and Department of Gastroenterology and Hepatology,
University Hospital Essen, University Duisburg-Essen, Essen, Germany.
9 University Hospitals KU Leuven, Leuven, Belgium. 10 Janssen Infectious Diseases BVBA, Beerse, Belgium. 11 Janssen Research & Development LLC, Titusville, NJ, USA.
A B S T R A C T A B S T R A C T A B S T R A C T A B S T R A C T A B S T R A C T
Background and rationale. Background and rationale.Background and rationale. Background and rationale.
Background and rationale. The REPLACE study (NCT01571583) investigated telaprevir-based triple therapy in patients who have recurrent genotype 1 hepatitis C virus (HCV) infection following liver transplantation and are on a stable immunosuppressant regimen of tacrolimus or cyclosporin A. Patients received telaprevir 750 mg 8-hourly with pegylated interferon 180 μg weekly and rib-avirin 600 mg daily, followed by a further 36 weeks of pegylated interferon and ribrib-avirin alone and 24 weeks of follow-up. Efficacy (sustained virological response [SVR] 12 weeks after last planned study dose), safety and tolerability of telaprevir throughout the study were assessed. Pharmacokinetics of telaprevir, tacrolimus and cyclosporin A were also examined. Results.Results.Results.Results.Results. In total, 74 pa-tients were recruited. Overall, 72% (53/74; 95% CI: 59.9 to 81.5) of papa-tients achieved SVR at 12 weeks following completion of treatment. Anticipated increases in plasma concentrations of tacrolimus and cyclosporin A occurred during telaprevir treatment and were successfully managed through immunosuppressant dose reduction and, for tacrolimus, reduced dosing frequency. Safety and tolerability of telaprevir-based triple therapy were generally comparable with previous data in non-transplant patients, although rates of reported anemia (55% [41/74]) were higher. Elevated plasma creatinine (46% [34/74]) was observed during REPLACE – consistent with the post-liver transplant population and the co-administered immunosuppressants. Conclusion. Conclusion. Conclusion. Conclusion. Conclusion. Telaprevir-based triple therapy in patients with recurrent genotype 1 HCV infection following liver transplantation produced high rates of SVR. Thera-peutic concentrations of immunosuppressants were maintained successfully through dose modification during telaprevir treatment.
Key words. Key words.Key words. Key words.
Key words. Telaprevir. Hepatitis C infection. Liver transplant.
July-August, Vol. 15 No. 4, 2016: 512-523
INTRODUCTION
Hepatitis C virus (HCV) remains the primary
indica-tion for liver transplantaindica-tion in Europe.1 HCV infection
almost invariably recurs in patients who have detectable
levels of HCV RNA prior to transplant2,3 and sets the stage
for accelerated fibrosis and dysfunction of the graft;
cir-rhosis related to HCV occurs in 20-30% of graft recipients
within 5 years of the transplant.4-6 Treatment of recurrent
HCV in liver transplant patients aims to prevent compli-cations that can lead to graft loss.7,8
After the discovery of the hepatitis C virus in 1989,9
de-velopment of new therapies was slow with only small
in-creases in SVR rates for over 20 years.10 Commonly used
The Official Journal of the Mexican Association of Hepatology, the Latin-American Association for Study of the Liver and
the Canadian Association for the Study of the Liver
Manuscript received: Manuscript received: Manuscript received: Manuscript received:
513
Telaprevir-based therapy in stable liver transplant. , 2016; 15 (4): 512-523
dual therapy of pegylated interferon (Peg-IFN, P) in com-bination with ribavirin (RBV, R) achieves sustained viro-logical response (SVR) rates as low as 40-50% in HCV
genotype 1 patients.10 In patients who have undergone
liv-er transplantation, SVR rates are even lowliv-er with rates of 23-31%.11 In 2011, adding the first-wave direct-acting
anti-virals (DAAs) telaprevir (TVR) or boceprevir (BOC) to PR resulted in marked improvements in SVR rates
com-pared with dual therapy.12-17 HCV drug treatment rapidly
evolved, and it was only three years later that the second-wave of drugs began to be approved for the treatment of HCV. These include triple therapy of simeprevir (SMV) or sofosbuvir (SOF) with PR, or interferon-free therapy of sofosbuvir in combination with simeprevir, ledipasvir
(LDV) or daclatasvir (DCV).18-21 More recently, the
cbination of ritonavir-boosted paritaprevir (PTV/r), om-bitasvir (OBV) and dasabuvir (DSV) has become available.22,23
Although these interferon-free second-wave therapies are now becoming the standard of care for treating HCV, the close proximity of approvals of first-wave DAAs to second-wave DAAs means their clinical development programs have overlapped.
Since cyclosporin A (CsA) and tacrolimus (TAC) are both substrates for both cytochrome P450 3A4 and P-glycoprotein, treating post-transplant patients with
DAAs may be challenging.24-26 TVR and BOC are both
substrates and inhibitors of cytochrome P450 3A4 (TVR is also a substrate and inhibitor of P-glycoprotein), so there is a potential for drug interactions upon co-administration
with these immunosuppressants.16,17 Indeed, drug-drug
in-teraction studies with TVR and BOC have shown that these DAAs can increase plasma concentrations of the
im-munosuppressants CsA and TAC.27-30 Drug-drug
interac-tions with CsA and TAC and the second-wave DAAs may also need to be managed as SMV, DCV and ritonavir are also inhibitors of cytochrome P450 3A4, and SMV, SOF, DCV, LDV, PTV/r, DSV are inhibitors of P-glycopro-tein.18-23 It is therefore vital that the clinical benefits of the
DAAs are examined in the liver transplantation population. By managing the drug-drug interactions between TVR, TAC and CsA through immunosuppressant dose modifi-cation, a proof-of-concept study indicated that TVR-based triple therapy was viable to use in post-liver transplant
pa-tients who have experienced HCV recurrence.27,28
Fol-lowing on from this, the REPLACE study described here aimed to determine the efficacy, safety, and tolerability of TVR in combination with PR in a large population of pa-tients with chronic, genotype 1 HCV infection, who had undergone liver transplantation and were receiving TAC or CsA.
As well as providing information on TVR in transplant patients, given the lack of data in this population, the
re-sults of our study can also be used to inform the examina-tion of future DAAs in this patient populaexamina-tion.
Objectives
The main study objective was to determine the efficacy of TVR 750 mg every 8 hours (q8h) in combination with PR in patients with chronic, genotype 1 HCV infection who had undergone liver transplantation and were receiv-ing TAC or CsA. Efficacy was assessed as the number of patients achieving SVR12, defined as having undetectable HCV RNA 12 weeks following the last planned dose of study medication.
Secondary objectives included the comparison of SVR rates in the REPLACE study with historical control rates of SVR with dual therapy, the evaluation of safety and tol-erability of TVR in combination with PR and TAC or CsA, the pharmacokinetics of TVR and the immunosup-pressant drugs TAC and CsA when co-administered, the comparison of pre- and post-treatment liver graft histolo-gy, and the dose requirements for TAC and CsA.
MATERIAL AND METHODS
Study design
In this open-label, single-arm, multicenter, Phase IIIB study, patients received TVR 750 mg every 8 h (q8h) in
combination with Peg-IFN 180 μg/week, and an initial
Patients
Patients had received a first-time liver transplant > 6 months to 10 years prior to enrolling in the study, with a primary pre-transplant diagnosis of chronic, genotype 1 HCV infection that had recurred following transplanta-tion. HCV treatment-naïve patients and patients who had been treated with PR prior to transplant were included. Only patients with METAVIR F0-3 fibrosis were en-rolled, and patients with F0 fibrosis were only included if biopsy showed necroinflammation grade >2, or if alanine aminotransferase levels were > 2 times the upper limit of normal.
Exclusion criteria for this study included current infec-tion or co-infecinfec-tion with non-genotype 1 HCV and having received previous treatment with a DAA for HCV. Pa-tients who had received treatment for HCV with approved or investigational drugs following liver transplantation were not enrolled. Any patients with histological evidence of graft rejection on the most recent liver biopsy were ex-cluded, as were patients with contraindications to treat-ment with PR.
Immunosuppressant treatment regimen
All patients were on a stable immunosuppressant regi-men of either TAC or CsA for at least 1 month prior to the screening visit. Combination treatment of TAC or CsA with mycophenolate mofetil, and the addition of low-dose
prednisone (defined as a daily dose of ≤ 5 mg) were
per-mitted as part of the immunosuppressant regimen.
In order to minimize the risk of TAC or CsA levels becoming supra/subtherapeutic during co-administra-tion with TVR, immunosuppressant dosing, trough con-centrations, and safety parameters were assessed for the first 16 patients entering the study during the initial 4 weeks of treatment (10 receiving TAC and six receiving CsA). Results were evaluated by a Safety Monitoring Committee and used to formulate dose adjustment guid-ance for the participating investigators to use in the re-maining patients.
The guidance based on this review was that in patients
with a pre-TVR TAC dose of ≤ 5 mg daily, the suggested
TAC dose was 0.2-0.5 mg with subsequent dosing every 3 to 5 days. Data on patients receiving > 5 mg daily TAC dose prior to treatment with TVR were limited.
For patients receiving 100–200 mg CsA daily prior to initiating treatment with TVR, a lower starting dose of 25-50 mg CsA daily was suggested.
Following the end of TVR treatment, it was suggested that patients start a dose of TAC or CsA at least as high as their original dose prior to receiving TVR.
Efficacy of TVR-based triple therapy
Plasma HCV RNA was quantified using the Roche High Pure COBAS® Taqman® HCV test 2.0, which has a lower limit of quantification of 25 IU/mL and a limit of detection of 15 IU/mL. Samples of plasma for RNA quan-tification were collected during screening and on day 1 (baseline), day 7, weeks 2, 3, 4, 8, 12, 16, 24, 36, and 48 dur-ing treatment and 4, 12, and 24 weeks after completion of treatment.
Viral sequencing
Population sequencing analyses of the HCV NS3-4A protease were performed on all baseline samples and in the case of on-treatment virologic failure or relapse. HCV RNA was isolated from the plasma and the NS3-4A protease was amplified by real-time polymerase chain reaction. HCV RNA was sequenced if the values were above the limit of detection of the sequencing assay (~1,000 IU/mL). Virology analyses were performed using the list of TVR-resistant variants identified in patients enrolled in Phase II or III studies with TVR and who did not achieve a SVR.31
Pharmacokinetic analyses
Blood samples for TVR pharmacokinetic analysis were taken at weeks 2, 4, 6, and 8. Samples were analysed by liq-uid chromatography-tandem mass spectroscopy. The anal-ysis of TVR plasma concentration was performed centrally. The pharmacokinetic parameters of average
steady-state plasma concentration (Css,avg), predose plasma
concentration (Ctrough) and the area under the curve over
the dosing interval (AUCt) were calculated.
Measurement of TAC or CsA plasma concentrations were performed locally so that, in combination with safety assessments, investigators could titrate the doses of TAC or CsA according to standard treatment practices. These analyses were carried out at prespecified time points as well as at the discretion of the investigator. Descriptive statistics and graphical analyses were performed to deter-mine the effect of TVR on the plasma concentrations of TAC and CsA.
Adverse events and safety
515
Telaprevir-based therapy in stable liver transplant. , 2016; 15 (4): 512-523
Adverse events (AEs) were reported by patients and monitored by investigators throughout the study period. The severity of AEs and their relationship to TVR were recorded.
Statistical analyses
A sample size of 72 patients was considered adequate to provide 90% power to establish the superiority of the pri-mary endpoint (SVR12) over the historical control rate of 31% when an observed SVR rate of 50% is assumed. SVR was estimated with a 95% confidence interval (CI). The historical SVR rate used in the study protocol, 27% with a 95% CI of 23 to 31, was estimated through a meta-analysis of 16 previously published studies in this post-transplant
population.11 If the lower bound of the 95% CI excluded
the prespecified historical control of 31%, the null hy-pothesis was rejected.
For continuous parameters, summary descriptive statistics included a number of observations, mean, 95% CI, standard deviation (SD), standard error (SE), mini-mum, median, Q1, Q3, and maximum. For categorical pa-rameters, summary statistics included frequency and percentages.
For virological response, a non-completer was regard-ed as a virological failure (NC = F virological failure im-putation); intermittent missing values were imputed with 1
(i.e., response) if the immediate preceding and following visits demonstrated response and with 0 (i.e., no re-sponse) otherwise.
Statistical analyses were carried out using SAS software v9.2, with the exception of the pharmacokinetic analysis, which was conducted via non-linear mixed-effects model-ling with NONMEM software version VII level 2.0.
RESULTS
Baseline patient characteristics
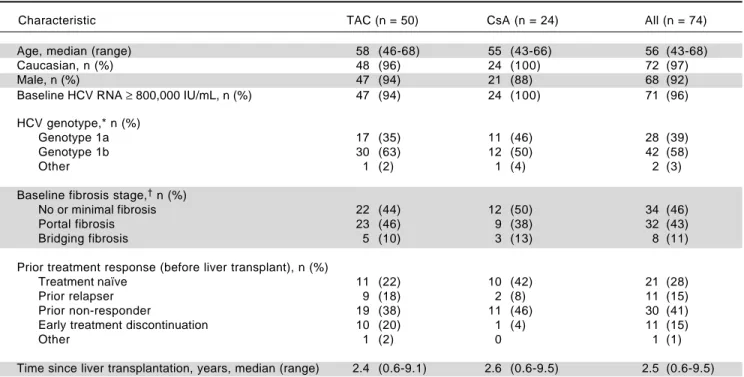
In total, 74 patients were enrolled in the study and the majority of patients were male (92%) and Caucasian (97%), with a median age of 56 years (Table 1). The ma-jority of patients (58%) had HCV genotype 1b, and 96%
of patients had HCV RNA levels ≥ 800,000 IU/mL at
baseline (Table 1). Overall, 28% (21/74) of patients were HCV treatment naïve; of the remaining 53 patients who had received HCV treatment prior to transplantation, 57% (30/53) were prior relapsers, and 21% (11/53) were prior non-responders (Table 1). Patients with no or minimal fibrosis made up 46% of the patients enrolled in the study, 43% of patients had portal fibrosis, and the re-maining 11% had bridging fibrosis (Table 1). Of the 74 patients enrolled in the study, 88% completed the TVR treatment phase.
Table 1. Baseline patient characteristics for all patients, by immunosuppressant regimen and overall.
Characteristic TAC (n = 50) CsA (n = 24) All (n = 74)
Age, median (range) 58 (46-68) 55 (43-66) 56 (43-68)
Caucasian, n (%) 48 (96) 24 (100) 72 (97)
Male, n (%) 47 (94) 21 (88) 68 (92)
Baseline HCV RNA ≥ 800,000 IU/mL, n (%) 47 (94) 24 (100) 71 (96)
HCV genotype,* n (%)
Genotype 1a 17 (35) 11 (46) 28 (39)
Genotype 1b 30 (63) 12 (50) 42 (58)
Other 1 (2) 1 (4) 2 (3)
Baseline fibrosis stage,† n (%)
No or minimal fibrosis 22 (44) 12 (50) 34 (46)
Portal fibrosis 23 (46) 9 (38) 32 (43)
Bridging fibrosis 5 (10) 3 (13) 8 (11)
Prior treatment response (before liver transplant), n (%)
Treatment naïve 11 (22) 10 (42) 21 (28)
Prior relapser 9 (18) 2 (8) 11 (15)
Prior non-responder 19 (38) 11 (46) 30 (41)
Early treatment discontinuation 10 (20) 1 (4) 11 (15)
Other 1 (2) 0 1 (1)
Time since liver transplantation, years, median (range) 2.4 (0.6-9.1) 2.6 (0.6-9.5) 2.5 (0.6-9.5)
Virological response
The primary endpoint of SVR12 was achieved by 72% (53/74, 95% CI: 59.9 to 81.5) of all patients enrolled in the study, 66% (33/50, 95% CI: 51.2 to 78.8) of patients receiv-ing TAC, and 83% (20/24, 95% CI: 62.6 to 95.3) of patients receiving CsA achieved SVR12 (Table 2). The difference in SVR rates between TAC and CsA is not significant giv-en the small sample size and lack of randomization to im-munosuppressant. Rates of efficacy by prior response to treatment showed 62% (13/21) of treatment-naïve patients, 82% (9/11) of prior relapsers and 73% (22/30) of prior non-responders achieved SVR12 (Table 2).
In patients who had received a liver transplant 1-3 years prior to study enrollment, 32/43 (74%; 95% CI: 58.8 to 86.5) patients achieved SVR12, as did 19/25 (76%; 95% CI: 54.9 to 90.6) patients who had received a transplant > 3 years prior to the study start. Too few patients had re-ceived a liver transplant < 1 year prior to enrollment (n = 2) to allow meaningful comparison of SVR12 rates (Supple-mentary Figure 2).
SVR12 rates were similar in patients with HCV geno-type 1b (71%, 95% CI: 55.4 to 84.3) and genogeno-type 1a
infec-tion (68%, 95% CI: 47.6 to 84.1). In terms of IL28B status,
the highest SVR12 rates were seen in patients with the CC genotype (94%, 95% CI: 69.8 to 99.8) compared with the CT and TT genotypes (68%, 95% CI: 50.9 to 81.4 and 61%, 95% CI: 35.7 to 82.7, respectively).
Overall, 31% (23/74) of patients had rapid virological response (RVR), defined as HCV RNA < 25 IU/mL, tar-get not detected at week 4. Of the patients receiving TAC, 38% (19/50) achieved RVR, as did 17% (4/24) of those re-ceiving CsA (Table 2). All patients who achieved RVR (23/74)
went on to achieve extended RVR (eRVR), defined as HCV RNA < 25 IU/mL, target not detected at weeks 4 and 12 (Table 2).
Virology
On-treatment virologic failure was observed in three (14%) treatment-naïve patients, one prior relapser (9%) and three (10%) prior non-responders. Five of the seven patients (71%), who experienced on-treatment virologic failure and also had sequencing data, had high-level tel-aprevir-resistant variants at the time of failure. One patient (14%) had lower-level telaprevir-resistant variants and one patient (14%) had wild-type virus.
All four patients with HCV genotype 1a virus who ex-perienced on-treatment virologic failure had higher-level telaprevir-resistant variants V36M+R155K. Of the pa-tients with HCV genotype 1b virus who experienced on-treatment virologic failure, one patient had a higher-level telaprevir-resistant variant (T54S+A156S), one patient had a lower-level telaprevir resistant variant (V36L+T54S/T), and one patient had wild-type virus.
In patients who relapsed, one patient was treatment naïve (5%) and three patients (10%) were prior non-re-sponders. Overall, lower-level telaprevir-resistant variants were present in three of these four patients (75%) at the time of relapse, one patient had wild-type virus, and all four of these patients had HCV genotype 1b.
Pharmacokinetic analyses of TVR
The steady-state predose (C0h) and maximal (Cmax,ss)
concentrations of TVR, and area under the curve 24 hours
Table 2. Virological response in patients, by immunosuppressant regimen and overall.
n/N (%) TAC (n = 50) CsA (n = 24) All (n = 74)
RVR 19/50 (38) 4/24 (17) 23/74 (31)
eRVR 19/50 (38) 4/24 (17) 23/74 (31)
SVR12
All 33/50 (66) 20/24 (83) 53/74 (72)
Treatment naïve 4/11 (36) 9/10 (90) 13/21 (62)
Prior relapser 7/9 (78) 2/2 (100) 9/11 (82)
Prior non-responder 14/19 (74) 8/11 (73) 22/30 (73)
Genotype 1a* 11/17 (65) 8/11 (73) 19/28 (68)
Genotype 1b* 19/30 (63) 11/12 (92) 30/42 (71)
No or minimal fibrosis 26/34 (77)
Portal fibrosis 21/32 (66)
Bridging fibrosis 6/8 (75)
517
Telaprevir-based therapy in stable liver transplant.
, 2016; 15 (4): 512-523
D. D. D. D. D.
Cyclosporin plasma concentration over time.
Cyclosporin plasma concentration (ng/mL)
700
600
500
400
300
200
100
0
Baseline
Day 2
Day 3
Day 5
Day 7
Week 2
Week 3
Week 4
Week 8
Week 10
Week 12
Last TVR + Day 1
Last TVR + Day 2
Last TVR + Day 3
Last TVR + Day 4
Last TVR + Day 5
Last TVR + Day 6
Last TVR + Day 7
Last TVR + Day 8
Week 16
Week 48
C.C.C.C.C
. Tacrolimus plasma concentration over time.
Tacrolimus plasma concentration (ng/mL)
30
25
20
15
10
5
0
Baseline
Day 2
Day 3
Day 5
Day 7
Week 2
Week 3
Week 4
Week 8
Week 10
Week 12
Last TVR + Day 1
Last TVR + Day 2
Last TVR + Day 3
Last TVR + Day 4
Last TVR + Day 5
Last TVR + Day 6
Last TVR + Day 7
Last TVR + Day 8
Week 16
Week 48
Figure 1.Figure 1.Figure 1.Figure 1.Figure 1.
Mean
daily dose of
AAAAA
) tacrolimus and
BBBBB
) cyclosporin A and the mean plasma concentrations of
CCCCC
) tacrolimus and
DDDDD
) cyclosporin A during the
study. Dashed lines denote the therapeutic range of concentrations.
Total daily dose (mg)
300
250
200
150
100
50
B.B.B.B.B
. Cyclosporin dose over time.
Screening
Baseline
Day 2
Day 3
Day 5
Day 7
Week 2
Week 3
Week 4
Week 6
Week 8
Week 10
Week 12
Week 16
Week 20
Week 24
Week 28
Week 36
Week 48
Follow-up Week 4
Follow-up Week 12
Follow-up Week 24
Total daily dose (mg)
A.A.A.A.A
. Tacrolimus dose over time.
20
15
10
5
0
Screening
Baseline
Day 2
Day 3
Day 5
Day 7
Week 2
Week 3
Week 4
Week 6
Week 8
Week 10
Week 12
Week 16
Week 20
Week 24
Week 28
Week 36
Week 48
Follow-up Week 4
Follow-up Week 12
Follow-up Week 24
Time point Time point
Time point
after dosing (AUC24) were comparable between the patients receiving TAC and CsA (Table 3). The mean
steady-state concentrations of TVR (Css,avg) were similar
between patients receiving TAC and CsA, and within the expected ranges when TVR is dosed q8h (Table 3).
Dose adjustments for TAC and CsA
At screening, the mean (SE) daily dose of TAC was 2.34 (0.222) mg, which was reduced to 1.87 (0.236) mg at baseline and further reduced on day 2 of treatment to 0.72 (0.217) mg. The lowest mean dose of TAC when coadministered with TVR was 0.21 (0.045) mg at week 3 (Figure 1A). Fol-lowing the completion of the telaprevir treatment phase, mean daily doses of TAC ranged from 3.25 (0.275) mg/day to 3.56 (0.478) mg/day; in some patients, this TAC dose was higher than the initial pre-TVR dosing.
The mean dose of CsA at screening was 151.0 (11.00) mg, which was reduced to 86.3 (11.90) mg at baseline. Fur-ther reductions of the mean daily CsA dose to between 47.3 (3.96) mg and 57.6 (8.53) mg occurred during the TVR treatment phase (Figure 1B). Following the end of the TVR administration, mean daily doses of CsA were in-creased to between 150.2 (9.80) mg and 165.3 (7.13) mg, which were in the range of pre-TVR doses.
Therapeutic levels of TAC and CsA were largely main-tained by the investigator during TVR treatment by adjust-ing the dose of TAC or CsA and prolongadjust-ing the TAC dosing interval. Investigator-directed reductions in immu-nosuppressant dose made at baseline for all patients ensured maintenance of therapeutic concentrations of TAC and CsA throughout the TVR treatment period (Figure 1C and 1D).
Safety
Discontinuation of treatment with TVR due to AEs was infrequent with a rate of 5% (four patients: one case each of neutropenia and thrombocytopenia, abdominal pain, cholestasis, and urinary tract infection). Discontinuation of PR treatment due to AEs occurred in 12 (16%) patients.
Overall, AEs were reported by 100% of patients, with 12% (9/74) reporting serious AEs (SAEs). No patients died in the study. The most commonly reported AEs during the
TVR treatment phase were anemia (55%, 41/74), pruritus (46%, 34/74), anorectal symptoms (45%, 33/74), and rash (39%, 29/74). AEs of grade 3 or greater were reported by 49% (36/74) of patients, and 11% (8/74) of patients expe-rienced grade 4 AEs (Table 4).
Of the patients who experienced anemia, 37% (27/74) had a reduction in RBV dose and 47% (35/74) required supportive treatment, with 42% (31/74) receiving an eryth-ropoiesis-stimulating agent and 22% (16/74) receiving a blood transfusion.
Elevated serum creatinine levels occurred in 46% (34/74) of patients during the TVR treatment phase, with most be-ing grade 1 (26%, 19/74) in severity (defined as ≥ 1.1 - ≤ 1.3 times the upper limit of normal) and occurring with a similar incidence between the TAC and CsA groups. Only one patient (1%) experienced an increase in creatinine that was considered grade 3 in severity (defined as > 1.8 - ≤ 3.4 times the upper limit of normal).
Graft rejection occurred in six patients (8%) during the study, three of whom were receiving CsA and three who were receiving TAC. Graft rejection did not occur during the TVR treatment phase, and none of these cases resulted in graft loss or were considered by investigators to be relat-ed to TVR. Of the patients receiving CsA, one patient with a grade 2 acute liver rejection at week 29 continued on the same PR dose, and two patients with a grade 3 event discon-tinued PR permanently at weeks 24 (liver transplant rejec-tion) and 35 (suspected graft rejecrejec-tion), respectively. In the patients receiving TAC, one patient experiencing a grade 2 liver graft rejection at week 20 permanently discontinued PR. At week 24 and 25, two other patients experienced grade 3 and 4 liver graft rejection events, respectively, but continued treatment with no changes to PR dosing. Patients who received systemic corticosteroids to treat the rejection stopped PR treatment per protocol; for the patients contin-uing PR treatment, no dosage changes were made. All the patients recovered without liver graft loss.
Liver graft histology
The majority of liver graft biopsies taken from patients 24 weeks after treatment completion (67%, 34/51) showed no change in METAVIR fibrosis stage; 18% (9/51)
Table 3. Telaprevir concentrations and exposure in the study population.
Mean (SD) TAC (n = 45) CsA (n = 22) Total (n = 67)
AUC24, ng•h/mL 85,633 (22,131) 87,168 (18,433) 86,100 (20,900)
Css,avg, ng/mL 3,570 (924) 3,631 (767) 3,590 (870)
C0h, ng/mL 3,100 (876) 3,164 (725) 3,120 (825)
Cmax,ss, ng/mL 3,824 (951) 3,855 (792) 3,840 (896)
AUC24: area under the plasma concentration-time curve over 24 h. Css,avg: average steady-state plasma concentration. C0h: trough plasma concentration.
519
Telaprevir-based therapy in stable liver transplant. , 2016; 15 (4): 512-523
showed improvement and 16% showed progression of fibrosis (8/51). A similar trend was seen for METAVIR overall inflammatory activity, whereas Ishak-assessed in-flammatory activity improved between pre- and post-treatment in the majority of patients, and in more patients receiving TAC compared with CsA. There was no differ-ence in fibrosis seen between genotype 1a and 1b patients, but more patients with genotype 1a than 1b experienced an improvement in overall inflammatory activity (45% com-pared with 20%).
In terms of graft rejection, no biopsies showed defini-tive histological evidence of acute or chronic rejection or plasma cell hepatitis 24 weeks after the last actual dose of study drugs, although two specimens showed indetermi-nate or uncertain evidence of acute rejection.
DISCUSSION
Patients who develop chronic HCV infection can progress to develop severe liver disease and may require a liver transplant. Following transplantation, recurrence of HCV infection is almost universal, and associated with an accelerated progression of graft fibrosis. Eradicating HCV infection in these patients is therefore a priority.
In this study, SVR12 rates of 72% (53/74, 95% CI: 59.9 to 81.5) were achieved in post-liver transplant patients without cirrhosis with recurrent HCV treated with TVR
in combination with PR. This indicates improved efficacy
over treatment with PR alone.11 The findings in our larger
cohort are consistent with an initial small study treating recurrent HCV in post-transplant patients with TVR-based triple therapy that demonstrated improved rates of SVR over historical rates with PR, with five out of nine
patients achieving SVR24.28 The SVR rates in patients with
F0-1 and F2 fibrosis were relatively similar, but it should be noted that patients enrolled in the REPLACE study had less advanced fibrosis, with F3 fibrosis present in only 11% of patients, in contrast to other studies which en-rolled a higher proportion of patients with advanced
fibro-sis and cirrhofibro-sis.32,33 Higher SVR12 rates were seen in the
REPLACE study than in two other recently published studies evaluating virological response to TVR-based ther-apy in more ‘difficult-to-treat’ groups of post-liver trans-plant patients; those patients had more severe liver disease (42-53% had F3-F4 fibrosis) and, in some cases, had al-ready received previous dual therapy for post-transplant
recurrence of HCV infection.31,32
Overall, low numbers of patients experienced on-treat-ment virological failure (11%) or relapse (5%). These data and the resistance profile of patients who experienced re-lapse or on-treatment virologic failure are consistent with findings in non-transplant patients treated with triple ther-apy, where approximately 10% of patients experienced on-treatment virological failure and approximately 10%
Table 4. Adverse events reported during the telaprevir treatment phase.
n (%) TAC (n = 50) CsA (n = 24) All (n = 74)
Any AE 50 (100) 24 (100) 74 (100)
SAEs 7 (14) 2 (8) 9 (12)
Deaths 0 0 0
Any ≥ grade 3 AE 25 (50) 11 (46) 36 (49)
Grade 3 anemia SSC 12 (24) 4 (17) 16 (22)
Grade 3 rash SSC 0 0 0
Any grade 4 AE 8 (16) 0 8 (11)
Most commonly reported AEs*
Anemia SSC 27 (54) 14 (58) 41 (55)
Pruritus SSC 28 (56) 6 (25) 34 (46)
Anorectal SSC 23 (46) 10 (42) 33 (45)
Rash SSC 21 (42) 8 (33) 29 (39)
Asthenia 16 (32) 11 (46) 27 (36)
Headache 17 (34) 8 (33) 25 (34)
Fatigue 16 (32) 5 (21) 21 (28)
Diarrhea 17 (34) 2 (8) 19 (26)
Thrombocytopenia 15 (30) 4 (17) 19 (26)
Nausea 11 (22) 6 (25) 17 (23)
Pyrexia 10 (20) 5 (21) 15 (20)
Any AE leading to permanent discontinuation of TVR 4 (8) 0 4 (5)
relapsed.12-14 The study size did not allow for investigation
into predictive factors of SVR response in patients receiv-ing TVR in combination with PR.
Safety findings in this study with TVR in combination with PR in liver transplant recipients were consistent with previous studies, which showed more safety and tolera-bility issues than in non-transplant patients;27,28,34,35
over-all, 12% of patients reported SAEs, 49% (36/74) reported grade 3 or higher AEs and 11% experienced grade 4 AEs. However, only four patients (5%) permanently discontin-ued treatment with TVR due to an AE, which is similar to non-transplant patients.12-14
Consistent with previous findings that anemia is a com-mon occurrence in liver transplant recipients treated for
recurrent HCV infection with PR therapy alone,36 the
RE-PLACE study demonstrated an increased rate of anemia in patients receiving TVR in combination with PR compared with non-transplant patients, despite using a lower RBV dose. However, the rates of measured hemoglobin de-crease between transplant and non-transplant patients were similar.12-14 These data are also consistent with a
pre-vious study where 65% (23/35) of patients treated with TVR-based triple therapy, and 78% (32/41) of patients re-ceiving BOC-based triple therapy developed anemia, and 63% of the total patient population received a reduced
dose of RBV.30 Rates of creatinine elevation in the
RE-PLACE study were consistent with the post-liver trans-plant population studied and the co-administered immunosuppressants. Renal dysfunction is not uncom-mon in post-transplant patients and calcineurin inhibitor nephrotoxicity is frequently the cause. However, it is not the only source of post-liver transplantation dysfunction. A review of 23 biopsies taken from 54 (out of a total of 2100) liver transplant patients from a single center from 1996 onwards demonstrated several different causes of
renal dysfunction resulting in increased creatinine.37
The histological findings from these biopsies showed cal-cineurin inhibitor nephrotoxicity (48%), hypertensive changes (44%), membranoproliferative glomerulonephri-tis (17%), immunoglobulin A nephropathy (9%), diabetic nephropathy (9%), crescentic glomerulonephritis (4%) and acute tubular necrosis (4%).
As many DAAs are substrates and/or inhibitors of cyto-chrome P450 (CYP) 3A4 and P-glycoprotein, triple thera-py of recurrent HCV is burdened by significant potential for drug-drug interactions with the immunosuppressants
TAC and CsA.14, 17-23 Mean plasma concentrations of TAC
and CsA are known to increase upon co-administration
with TVR,27,28 yet increases in serum levels of
immuno-suppressant drugs have successfully been managed with
dose modification of TAC and CsA.27 The REPLACE
study demonstrated that, with adequate knowledge and in-formation to support accurate anticipation of the extent of
drug-drug interactions with TAC and CsA, investigators were able to successfully implement the necessary dose reductions. Additionally for TAC, decreased dose fre-quency at initiation of TVR treatment and incremental dose increases at the end of TVR treatment were also im-plemented. Accordingly, plasma concentrations were maintained at therapeutically active levels and no inci-dence of graft rejection or graft loss occurred during treat-ment with TVR. Overall, the rate of rejection in this study was similar to previously published studies using PR
(5%).6 The effective use of TVR in this stable liver
trans-plant patient population receiving TAC and CsA illus-trates that it is possible to manage drug interactions between DAAs and immunosuppressants. These data may be enlightening in the design of future studies with DAAs in this population.
While data on the efficacy of second-generation treat-ments in a post-transplant setting is now becoming availa-ble,38-40 not all countries will have access to these
treatments. As such, TVR may remain a useful therapeutic option in treating particular subsets of patients.
In summary, although drug-drug interactions impact dosing of CsA and TAC, these interactions can be managed clinically through modifications in TAC and CsA dose and TAC dosing intervals. TVR-based triple therapy in post-liv-er transplant patients with recurrent HCV infection is an ef-fective therapy, with safety and tolerability profiles generally consistent with previous studies of TVR-based triple therapy in the post-liver transplant study population on calcineurin inhibitors. Rates of reported anemia were higher in this study than previous TVR-based triple therapy studies in non-transplant patients.
ABBREVIATIONS
• AE: adverse event.
• AUC24: area under the curve 24 hours after dosing.
• AUCt: area under the curve over the dosing interval.
• C0h: initial concentration.
• CI: confidence interval.
• Cmax,ss: maximal steady-state concentration.
• CsA: cyclosporin A
• Css,avg: average steady-state plasma concentration. • Ctrough: pre-dose plasma concentration.
• CYP: cytochrome P450.
• DAA: direct-acting antiviral.
• eRVR: extended RVR.
• HCV: hepatitis C virus.
• LLOQ: lower limit of quantification. • Peg-IFN/P: pegylated interferon.
• q8h: every 8 hours.
• RBV/R: ribavirin.
521
Telaprevir-based therapy in stable liver transplant. , 2016; 15 (4): 512-523
• SAE: serious AE.
• SD: standard deviation.
• SE: standard error.
• SVR: sustained virologic response.
• TAC: tacrolimus.
• TVR: telaprevir.
CONFLICTS OF INTEREST
X Forns has received unrestricted grant support from
Janssen Pharmaceuticals, and acted as an advisor for
AbbV-ie, Janssen Pharmaceuticals, and Gilead Sciences; D Samuel
has been a consultant for AbbVie, Astellas, Gilead Sciences, Janssen Pharmaceuticals, Merck Sharp & Dohme, and Novartis; D Mutimer has been a speaker/consultant to Janssen Pharmaceuticals and other pharmaceutical companies;
S Fagiuoli has acted as consultant/speaker for Abbvie,
Astellas, Bayer, Biotest Pharmaceuticals, Bristol-Myers Squibb, Gilead Sciences, Grifols, Kedrion, Janssen Phar-maceuticals, Merck Sharp & Dohme, Novartis, and Roche;
M Navasa has received unrestricted grant support from
Novartis and has acted as an advisor for Novartis; K Agarwal
has received grant support from Astellas, Gilead Sciences, and Roche and been a consultant/speaker for AbbVie, Astellas, Bristol-Myers Squibb, Gilead Sciences, Glaxo-SmithKline, Janssen Pharmaceuticals, Merck Sharp &
Dohme, Novartis, and Roche; M Berenguer has been a
speaker/consultant for AbbVie, Janssen Pharmaceuticals,
Merck Sharp & Dohme, Novartis, and Roche; M Colombo
has been a speaker/consultant for AbbVie, Alfa Wasser-mann, Bristol-Myers Squibb, Bayer, Boehringer Ingelheim, Gilead Sciences, GlaxoSmithKline, Janssen Pharmaceu-ticals, Jennerex Biotherapeutics Incorporated, Merck, Novartis, Roche, and Vertex, and has received grant/ research support from Bristol-Myers Squibb, Gilead
Sciences, and Roche; K Herzer has received grant support
from Astellas, Biotest, and Novartis, and been a consultant/ speaker for AbbVie, Biotest, Bristol-Myers Squibb, Gilead Sciences, Janssen Pharmaceuticals, Novartis, and Roche;
F Nevens has received grant support from Astellas, Ipsen,
Janssen Pharmaceuticals, Merck Sharp & Dohme, and
Roche; B Daems, K Janssen, H Kimko, E Lathouwers,
S Ouwerkerk-Mahadevan, R Van Solingen-Ristea, and J Witek
are employees of Janssen Pharmaceuticals and may be Johnson & Johnson stockholders.
FINANCIAL SUPPORT
This study was sponsored by Janssen Pharmaceuticals. Writing assistance was provided by Stephanie Gibson (Medical Writer) of Zoetic Science, an Ashfield company, part of UDG Healthcare plc, Macclesfield, UK; this sup-port was funded by Janssen Pharmaceuticals.
The REPLACE study was registered with ClinicalTrials.gov (NCT01571583).
AUTHORS’ CONTRIBUTIONS
Xavier Forns, Didier Samuel, David Mutimer, Kosh Agarwal, James Witek and Rodica Van Solingen-Ristea contributed to the conception and design of this study. Xavier Forns, Didier Samuel, David Mutimer, Stefano Fagiuoli, Miquel Navasa, Kosh Agarwal, Marina Berenguer, Massimo Colombo, Kerstin Herzer and Frederik Nevens recruited patients into the study and participated in data collection. All authors contributed to data analysis. All authors critically reviewed the article for important intellec-tual content and approved the final content for submission.
ACKNOWLEDGEMENTS
We express our gratitude to the patients and their fami-lies, the REPLACE study investigators including: Pietro Andreone, Rafael Barcena Marugan, Susanne Beckbaum, Luca Belli, Patrizia Burra, José Luis Calleja, Luis Castells, Maria Francesca Donato, Francois Durand, Peter Ferenci, Guido Gerken, Dominique Guyader, Marianne Latournerie, Andreas Maieron, Zoe Mariño, Christophe Moreno, George-Philippe Pageaux and Heiner Wedemeyer, Andrew Bathgate for his role in the Safety Monitoring Committee, and Stefan G. Hübscher for analysing the patient biopsy samples.
REFERENCES
1. European Association for the Study of the Liver. The burden of liver disease in Europe. Available from: http:// w w w . e a s l . e u / m e d i a s / E A S L i m g / D i s c o v e r / E U / 54ae845caec619f_file.pdf [accessed 18.09.15].
2. Teixeira R, Pastacrolimusaldi S, Papateodoridis GV, Bur-roughs AK. Recurrent hepatitis C after liver transplantation.
J Med Virol 2000; 61: 443-54.
3. Garcia-Retortillo M, Forns X, Feliu A, Moitinho E, Costa J, Navasa M, Rimola A, et al. Hepatitis C virus kinetics during and immediately after liver transplantation. Hepatology 2002; 35: 680-7.
4. Berenguer M, Ferrell L, Watson J, Prieto M, Kim M, Rayón M, Córdoba J, et al. HCV-related fibrosis progression following liver transplantation: increase in recent years. J Hepatol
2000; 32: 673-84.
5. Berenguer M. Hepatitis C after liver transplantation: risk fac-tors, outcomes, and treatment. Curr Opin Organ Transplant
2005; 10: 81-9.
6. Crespo G, Mariño Z, Navasa M, Forns X. Viral hepatitis in liv-er transplantation. Gastroenterology 2012; 142: 1373-83. 7. Braks RE, Ganne-Carrié N, Fontaine H, Paries J,
8. Carrion J, Navasa M, Garcia-Retortillo M, García-Pagan JC, Crespo G, Bruguera M, Bosch J, et al. Efficacy of antiviral therapy on HCV recurrence after liver transplantation: A randomised-controlled study. Gastroenterology 2007; 132: 1746-56.
9. Choo QL, Kuo G, Weiner AJ, Overby LR, Bradley DW, Houghton M. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science 1989; 244: 359-62.
10. Wilby KJ, Partovi N, Ford JA, Greanya E, Yoshida EM. Re-view of boceprevir and telaprevir for the treatment of chron-ic hepatitis C. Can J Gastroenterol 2012; 26: 205-10. 11. Wang CS, Ko HH, Yoshida EM, Marra CA, Richardson K.
In-terferon-based Combination anti-Viral therapy for Hepatitis C Virus after liver transplantation: A review and quantitative analysis. Am J Transplant 2006; 6: 1586-99.
12. Jacobson IM, McHutchison JG, Dusheiko G, Di Bisceglie AM, Reddy KR, Bzowej NH, Marcellin P, et al. Telaprevir for pre-viously untreated chronic hepatitis C virus infection. New Engl J Med 2011; 364: 2405-16.
13. Sherman KE, Flamm SL, Afdhal NH, Nelson DR, Sulkowski MS, Everson GT, Fried MW, et al. Response-guided telapre-vir combination treatment for hepatitis C telapre-virus infection. New Engl JMed 2011; 365: 1014-24.
14. INCIVO (telaprevir) EU Summary of Product Characteristics. Available from: http://www.ema.europa.eu/docs/en_GB/ document_library/EPAR_-_Product_Information/human/ 002313/WC500115529.pdf [accessed 18.09.2015].
15. Poordad F, McCone J Jr, Bacon BR, Bruno S, Manns MP, Sulkowski MS, Jacobson IM, et al. Boceprevir for untreated chronic HCV genotype 1 infection. N Engl J Med 2011; 364: 1195-206.
16. Bacon BR, Gordon SC, Lawitz E, Marcellin P, Vierling JM, Zeuzem S, et al. Boceprevir for previously treated chronic HCV genotype 1 infection. N Engl J Med 2011; 364: 1207-17. 17. VICTRELIS (boceprevir) EU Summary of Product
Character-istics. Available from: http://www.ema.europa.eu/docs/ en_GB/document_library/EPAR_-_Product_Information/hu-man/002332/WC500109786.pdf [accessed 18.09.2015]. 18. OLYSIO (simeprevir) EU Summary of Product
Characteris-tics. Available from: http://www.ema.europa.eu/docs/ en_GB/document_library/EPAR_-_Product_Information/hu-man/002777/WC500167867.pdf [accessed 18.09.2015]. 19. SOVALDI (sofosbuvir) EU Summary of Product
Characteris-tics. Available from: http://www.ema.europa.eu/docs/ en_GB/document_library/EPAR_-_Product_Information/hu-man/002798/WC500160597.pdf [accessed 18.09.2015]. 20. DAKLINZA (daclatasvir) EU Summary of Product
Character-istics. Available from: http://www.ema.europa.eu/docs/ en_GB/document_library/EPAR_-_Product_Information/hu-man/003768/WC500172848.pdf [accessed 18.09.2015]. 21. HARVONI (ledipasvir/sofosbuvir) EU Summary of Product
Characteristics. Available from: http://www.ema.europa.eu/ docs/en_GB/document_library/EPAR_-_Product_Information/ human/003850/WC500177995.pdf [Accessed 18.09.2015]. 22. VIEKIRAX (partiaprevir/ritonavir/ombitasvir) EU Summary of
Product Characteristics. Available from: http://ec.europa.eu/ health/documents/community-register/2015/20150115130406/ anx_130406_en.pdf [Accessed 18.09.2015].
23. EXVIERA (dasabuvir) EU Summary of Product Characteristics. Available from: http://ec.europa.eu/health/documents/commu-nity-register/2015/20150115130446/anx_130446_en.pdf [ac-cessed 18.09.2015].
24. Campana C, Regazzi MB, Buggia I, Molinaro M. Clinically sig-nificant drug interactions with cyclosporin. An update. Clin Pharmacokinet 1996; 30: 141-79.
25. Mignat C. Clinically significant drug interactions with new im-munosuppressive agents. Drug Saf 1997; 16: 267-78. 26. Shiraga T. Oxidative metabolism of tacrolimus and its
metab-olite by human cytochrome P450 3A subfamily. Drug Metab Pharmacokinet 1999; 14: 277-85.
27. Werner CR, Egetemeyr DP, Lauer UM, Nadalin S, Königsrain-er A, Malek NP, BKönigsrain-erg CP, et al. Telaprevir-based triple thKönigsrain-era- thera-py in liver transplant patients with Hepatitis C virus: A 12-Week pilot study providing safety and eficacy data. Liver Transpl 2012; 18: 1464-70.
28. Werner CR, Egetemeyr DP, Lauer UM, Nadalin S, Königsrain-er A, Malek NP, BKönigsrain-erg CP, et al. Feasibility of telaprevir-based triple therapy in liver transplant patients with Hepatitis C vi-rus: SVR 24 results. PLOS One 2013; 8: e80528.
29. Garg V, van Heeswik R, Lee JE, Alves K, Nadkarni P, Luo X. Effect of telaprevir on the pharmacokinetics of cyclosporine and tacrolimus. Hepatology 2011; 54: 20-7.
30. Faisal N, Yoshida EM, Bilodeau M, Wong P, Ma M, Burak KW, Al-Judaibi B, et al. Protease inhibitor-based triple ther-apy is highly effective for hepatitis C recurrence after liver transplant: a multicenter experience. Ann Hepatol 2014; 13: 525-32.
31. Kieffer TL, De Meyer S, Bartels DJ, Sullivan JC, Zhang EZ, Tigges A, Dierynck I, et al. Hepatitis C viral evolution in geno-type 1 treatment-naïve and treatment-experienced patients receiving telaprevir-based therapy in clinical trials. PLOS One 2012; 7: e34372.
32. Coilly A, Dumortier J, Botta-Fridlund D, Latournerie M, Leroy V, Pageaux GP, Agostini H, et al. Multicenter experience with boceprevir or telaprevir to treat Hepatitis C recurrence after liver transplantation: When present becomes past, what les-sons for future? PLoS One 2015; 10: e0138091.
33. Burton JR, O’Leary JG, Verna EC, Saxena V, Dodge JL, Stravitz RT, Levitsky J, et al. A US multicenter study of hep-atitis C treatment of liver transplant recipients with protease-inhibitor triple therapy. J Hepatol 2014; 61: 508-14.
34. Giusto M, Rodriguez M, Navarro L, Rubin A, Aguilera V, San-Juan F, Ortiz C, et al. Anemia is not predictive of sustained virological response in liver transplant recipients with hepati-tis C virus who are treated with pegylated interferon and rib-avirin. Liver Transpl 2011; 17: 1318-27.
35. Gordon FD, Kwo P, Vargas HE. Treatment of hepatitis C in liver transplant recipients. Liver Transpl 2009; 15: 126-35. 36. Bzowej N, Nelson DR, Tarrault NA, Everson GT, Teng LL,
Prabhakar A, Charlton MR, et al. PHOENIX: A randomized controlled trial of peginterferon alfa-2a plus ribavirin as a prophylactic treatment after liver transplantation for hepatitis C virus. Liver Transpl 2011; 17: 528-38.
37. O’Riordan A, Dutt N, Cairns H, Rela M, O’Grady JG, Heaton N, Hendry BM, et al. Renal biopsy in liver transplant recipients.
Nephrol Dial Transplant 2009; 24: 2276-82.
38. Gutierrez JA, Carrion AF, Avalos D, O’Brien C, Martin P, Bha-midimarri KR, Peyton A. Sofosbuvir and simeprevir for treat-ment of hepatitis C virus infection in liver transplant recipients. Liver Transpl 2015; 21: 823-30.
39. Poordad F, Schiff ER, Vierling JM, Landis C, Fontana RJ, Yang R, McPhee F,et al. Daclatasvir, sofosbuvir, and ribavi-rin combination for HCV patients with advanced cirrhosis or post-transplant recurrence: ALLY-1 Phase 3 study. Pre-sented at the 50th Annual Meeting of the European Associa-tion of the Liver. (InternaAssocia-tional Liver Congress™ 2015). Vienna, Austria, April 22-26. Abstract L08.
Prelimi-523
Telaprevir-based therapy in stable liver transplant. , 2016; 15 (4): 512-523
nary results of the prospective SOLAR 2 trial. Presented at the 50th Annual Meeting of the European Association of the Liver. (International Liver Congress™ 2015). Vienna, Aus-tria, April 22-26. Abstract G02.
Correspondence and reprint request:
Xavier Forns, M.D.
Liver Unit, Hospital Clinic, Villarroel 170, 08036 Barcelona, Spain. Tel.: +34 93 227-5753
E-mail: [email protected]
Time since liver transplant Time since liver transplantTime since liver transplant Time since liver transplant Time since liver transplant < 1 year 1-3 years > 3 years Prior treatment status Prior treatment status Prior treatment status Prior treatment status Prior treatment status Treatment naïve Prior relapser Prior non-responder Early discontinuation Other I L 2 8 B I L 2 8 B I L 2 8 B I L 2 8 B I L 2 8 B C C C T T T Genotype subtype Genotype subtype Genotype subtype Genotype subtype Genotype subtype 1a 1b 1d Stage of fibrosis Stage of fibrosis Stage of fibrosis Stage of fibrosis Stage of fibrosis No or minimal fibrosis Portal fibrosis Bridging fibrosis HCV RNA at baseline HCV RNA at baselineHCV RNA at baseline HCV RNA at baselineHCV RNA at baseline < 800,000 IU/mL ≥ 800,000 IU/mL
Supplementary Figure 2. Supplementary Figure 2.Supplementary Figure 2.
Supplementary Figure 2.Supplementary Figure 2. SVR12 rates by subgroups according to baseline disease characteristics. Dashed reference line: SVR rate of the overall popula-tion: 71.62%. n: number of patients with SVR. N: number of patients with data. LLC: lower limit of the 95% CI. ULC: upper limit of the 95% CI.
n N % LCL UCL
2 6 33.3 4.3 77.7 32 43 74.4 58.8 86.5 19 25 76.0 54.9 90.6
13 21 61.9 38.4 81.9 9 11 81.8 48.2 97.7 22 30 73.3 54.1 87.7 9 11 81.8 48.2 97.7
0 1 0 0 97.5
15 16 93.8 69.8 99.8 27 40 67.5 50.9 81.4 11 18 61.1 35.7 82.7
19 28 67.9 47.6 84.1 30 42 71.4 55.4 84.3 2 2 100.0 15.8 100.0
26 34 76.5 58.8 89.3 21 32 65.6 46.8 81.4 6 8 75.0 34.9 96.8
3 3 100.0 29.2 100.0 50 71 70.4 58.4 80.7
0 20 40 60 80 100
SVR12 rate, % Supplementary Figure 1.
Supplementary Figure 1.Supplementary Figure 1.
Supplementary Figure 1.Supplementary Figure 1. AAAAA) REPLACE study design and BBBBB) patient disposition. B BB BB
Assessed for eligibility: N = 128
Lost to follow up: N = 1
Completed treatment: N = 64
• Tacrolimus: n = 43. • Cyclosporin: n = 21. Proceeded to treatment: N = 74
• Tacrolimus: n = 50. • Cyclosporin: n = 24.
Excluded: N = 54
• Not meeting inclusion criteria. • Declined to participate. • Other reasons.
Discontinuations: N = 9
• Adverse event: n = 4. • Meeting a stopping rule: n = 3. • Other: n = 2.
A A A A A
Start date: Q4 2011 End date: Q2 2014 TVR12/PR48
n = 74
0 4 8 12 16 36 48 60 72
↑ SVR12 assessment TVR
TVR TVR TVR TVR +++++ Peg-IFN Peg-IFN Peg-IFN Peg-IFN Peg-IFN alfaalfaalfaalfaalfa 2a2a2a2a2a
+ ++